Right Bundle Branch Block with Q Waves in V1 and V2
Right Bundle Branch Block with Q Waves in V1 and V2
Right Bundle Branch Block with Q Waves in V1 and V2
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
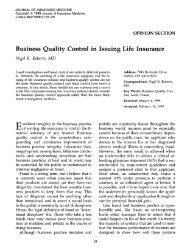
Journal of Insurance Medic<strong>in</strong>e Volume 2 I, No. 2 I £89Interest<strong>in</strong>g Electrocardiogram<strong>Right</strong> <strong>Bundle</strong> <strong>Branch</strong> <strong>Block</strong> <strong>with</strong>Q <strong>Waves</strong> <strong>in</strong> <strong>V1</strong> <strong>and</strong> <strong>V2</strong>M. Irend Ferrer, M.D.Consultant <strong>in</strong> Cardiology Metropolitan Life Insurance CompanyProfessor Emeritus of Cl<strong>in</strong>ical Medic<strong>in</strong>e, College of Physicians <strong>and</strong> Surgeons, Columbia UniversityConsultant Electrocardiographer, Presbyterian Hospital, Columbia Presbyterian Medical Center, New York, N.Y.A review of this trac<strong>in</strong>g of a 79-year-old man, taken <strong>in</strong> a preoperativerout<strong>in</strong>e evaluation when he entered the hospitalfor surgery, allows us to consider the evaluation of complete<strong>Right</strong> <strong>Bundle</strong> <strong>Branch</strong> <strong>Block</strong> (RBBB) <strong>in</strong> asymptomatic patients.The rhythm <strong>in</strong> the ECG is normal s<strong>in</strong>us at 75/m<strong>in</strong>. <strong>with</strong> aprolonged PR <strong>in</strong>terval (0.25 sec. <strong>in</strong> lead II). There are alsoatrial premature beats (APC), some of which are blocked <strong>and</strong>followed by a pause <strong>and</strong> a junctional escape beat (whoserhythmicity is 43/m<strong>in</strong>.). Such a sequence is marked <strong>with</strong> anarrow <strong>in</strong> V4. A conducted APC is marked <strong>in</strong> lead II.The IV conduction defect is of more serious nature. Note thatthe trac<strong>in</strong>g shows complete RBBB <strong>with</strong> a marked left axisdeviation (axis = -68 °) <strong>in</strong>dicat<strong>in</strong>g left anterior fascicularblock (LAFB). Of special importance <strong>in</strong> this record is thepresence of wide Q waves <strong>in</strong> <strong>V1</strong> <strong>and</strong> <strong>V2</strong> permitt<strong>in</strong>g thediagnosis of anteroseptal myocardial <strong>in</strong>farction. In summary,there is tri-fascicular block (RBBB, LAFB <strong>and</strong> prolonged PR).The etiology of this IV conduction defect is the anteroseptalmyocardial <strong>in</strong>farction. Thus coronary artery disease is present.Were this record to be submitted for <strong>in</strong>surance purposes therewould be little problem. However, the evaluation of anelectrocardiogram show<strong>in</strong>g only RBBB has undergoneconsiderable change <strong>in</strong> recent years. A recent review of thissubject from the Gerentology Research Center, NationalInstitute on Ag<strong>in</strong>g, National Institutes of Health 1 emphasizesfirstly that RBBB does not constitute a homogeneous cl<strong>in</strong>icaldisorder, <strong>and</strong> prognosis essentially depends on the nature<strong>and</strong> extent of the underly<strong>in</strong>g etiology. The study was made(on men only) on long term prognosis (8.4 years) <strong>and</strong>addresses the question whether RBBB of itself presagessubsequent cardiovascular disease <strong>and</strong> mortality. They foundthat cardiovascular morbidity <strong>and</strong> mortality are not <strong>in</strong>creased<strong>in</strong> asymptomatic men <strong>with</strong> RBBB as compared to matchedcontrols. The benign nature of simple RBBB is thusreaffirmed. However, although no <strong>in</strong>creased risks were noted<strong>in</strong> uncomplicated RBBB, if marked left axis deviation <strong>with</strong>or <strong>with</strong>out a prolonged PR <strong>in</strong>terval appeared <strong>in</strong> later life thereappears to be the likelihood of primary conduction systemdisease (calcification <strong>and</strong> sclerosis locally <strong>in</strong> the IV septum).This condition is age-related. Nevertheless, it is a benigndisorder <strong>in</strong> no way related to coronary disease.The solution <strong>in</strong> this trac<strong>in</strong>g is simple as coronary disease isclearly present.~ The evaluation of uncomplicated RBBBrequires considerable <strong>in</strong>vestigation <strong>in</strong> order to avoid anyexcess rat<strong>in</strong>g.ReferenceFleg, J.L.; Das, D.N.; LaKatta, E.G. <strong>Right</strong> <strong>Bundle</strong> <strong>Branch</strong> <strong>Block</strong>: Long Term Prognosis <strong>in</strong> Apparently Healthy Men. J. Am. Coll. Cardiol., 1(3)887-892, 1983.ErratumRegrettably a typesett<strong>in</strong>g omission <strong>and</strong> an error occurred <strong>in</strong> the text of Dr. Ferrer’s Interest<strong>in</strong>g Electrocardiogram <strong>in</strong> the previousissue of JIM: Pre-excitation <strong>and</strong> Cardiomyopathy (<strong>with</strong> a note on Myocardial Bridges), Vol. 21, No. 2, 1989 page 49.In the second paragraph, the sentence beg<strong>in</strong>n<strong>in</strong>g on l<strong>in</strong>e 20 should have read: "S<strong>in</strong>ce there is no WPW pattern present (whichdistorts the record) the ST-T abnormalities <strong>in</strong> Leads II, III, AVF, <strong>and</strong> V3-V6 emerge as evidence of underly<strong>in</strong>g myocardial disease.The electrocardiogram of 8/1/72 (on no digitalis) differs very little from that of 4/14/83 taken years later."131 m
Volume 2 I, No. 2 I £8£ Interest<strong>in</strong>g ElectrocardiogramInterest<strong>in</strong>g ElectrocardiogramTrac<strong>in</strong>g~VR,~’JL,~UFILl- IIIIllllttllIllllllllltllllltl~ ~m IIII II11 lill Ilil III11Illlll~! !ill illi:~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~/1111il !1II ~~~~~~IIIIIIIIIIIIIIIIIIIIIIIIIIIIIit111111111111111111It1111111tt11111tt1111t111111111t11111~. ih u~.~, ;IT ,~,~i- "~.1 ~ IlL ,..il ’iVI,VZ,V3~ ~ ~ III 111I III IIIWIIliJ~Nlliillitllitllltiltltlltlltlllltllltllllttltttllltlmtlltittttlttt!~ Ill]il~llllltll Ilililtllllltilit tiilillltiillltiliitilliliili~liiltl!til~7~ [~ ~ I}It!l~~l}ll~lllitllttllllllililtili!,ltllilliillil’"’",~,~J.’"’~,d IIIIIIIUIIW Jill I’,1 I1~ ll~;LL ~ ill ~i~i~~i~~iR~~i~i~i~j’"’"’"’"’m~mmm IIIIIIIIIIIIIII ............... Itlil~ ~ ~ " m ~[UN~~NNI~i~i~l~I~i~!~ ~I,... II tll -,,’llllllii, iii iii illIIIII Nil llll IIIill~ ~~ ]i~i~i~I~.~i~~~i~.~I~.~j~i~~i~~~"~N~~~~NN~i"’iii tlllllll.llll~lllll~~~ltllllllltlt I I tlllltltllltltllllllttllllllliliilil!~ ~ ~llli~llllllllllllllilllllllllltllllllllllilllllllllllli~lNltttlltltilll~tlill ’,~ Ill ~L~]~i}]~i~i~[il~~~~i~i~i~i~hi,it~~~11111~~~!lllll~ll~ll~llli[llllllll!llllllllll!ll !lllllllltlllllllilllllllttlttllltt!lt.ii!l!ilil~ ~lI}llllllll!lllllitllllll illllll!lllllllllltltllllilltllllltltlliiliiiil~II1111111 ~llllltllllll!lllllll~lllillliU"l~,~i i~.~ ~I.132