Cover Florida Application - Florida Blue
Cover Florida Application - Florida Blue
Cover Florida Application - Florida Blue

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Cover</strong> <strong>Florida</strong>PO Box 45074 • Jacksonville, FL 32232-5016(1) APPLICANT NAME (LAST NAME, FIRST NAME, MIDDLE INITIAL)KEY CODE 9860(2) APPLICANT ADDRESS (STREET ADDRESS, CITY, COUNTY, STATE, ZIP CODE)SECTION A(3) OTHER MAILING ADDRESS IF DIFFERENT THAN IN QUESTION #2 ■ Billing Only ■ Correspondence & BillingAddress: City: State: Zip:(4) MARITAL STATUS ■ SINGLE ■ MARRIED(5) GENDER ■ M ■ F(6) This information is optional and is for data collection only. It will not determine eligibility, rating orclaim payment. Language Preference: ■ English ■ Spanish ■ Other: ____________________________(7) TELEPHONE NUMBER( )Social Security Number(or Tax ID if no SSN issued)Date of Birth(MM/DD/YYYY)AgeZip CodePremium(As quoted on website)$SECTION BPlease refer to the eligibility requirements in Section D.(1) Will the coverage being applied for replace your current medical insurance? ■ Yes ■ No If yes, please complete the following information.Name of Company: _______________________________________________________________ Policy Number: ________________________Effective Date of Current <strong>Cover</strong>age: ___________________________ Termination Date of Current <strong>Cover</strong>age: _______________________________(MM/DD/YYYY)(MM/DD/YYYY)Mailing Address of Company: ______________________________________________________________________(2) If coverage in #1 was not in effect for at least 12 months, please provide additional coverage information.Name of Company: _______________________________________________________________ Policy Number: ________________________Effective Date of Current <strong>Cover</strong>age:____________________________ Termination Date of Current <strong>Cover</strong>age _______________________________(MM/DD/YYYY)(MM/DD/YYYY)Mailing Address of Company: ____________________________________________________________________________________________SEC.C(1) BENEFIT OPTION SELECTED:■ Plan I ■ Plan II(2) Are you interested in the Automatic Payment Option (APO)? ■ Yes ■ NoIf yes, please complete the Automatic Payment Option Form and return with your application.SECTION DSECTION EI hereby apply for the coverage selected on this application form. I understand that the coverage shall not become effective until this application is accepted, the initial premium paid, and an effective date is assigned to mycoverage by BCBSF. The coverage effective date will be the first available BCBSF billing date (1st, 8th, 15th or 23rd) after approval of this application unless an advance effective date is specified below. I have read thisapplication carefully and I represent that the information I have provided in this application is true and complete. I understand that this information is the basis for determining the issuance or denial of coverage and anymisstatement or omission may result in the denial of benefits and/or the termination of coverage. I understand that from time to time a rate adjustment may be necessary for any given product and that the premium ratefor my coverage may change on the product anniversary date due to an increase in my age. I understand that if any additional premium is required, my billing notice will reflect the additional premium. I understand that anyperson who knowingly and with intent to injure, defraud or deceive any insurer files a statement of claim or application containing any false, incomplete or misleading information is guilty of a felony of the third degree. Ifurther understand that there will be no continuation of benefits (continuous coverage) if I purchase another BCBSF policy and any condition that may have occurred under this policy may be treated as a pre-existing conditionunder the subsequent policy. I understand that this product provides limited benefits and is not considered major medical coverage.I authorize any physician, medical practitioner, hospital, clinic or other medical or medically-related provider, insurance company, employer or other organization, institution or person that has medical records or any otherknowledge of me to release such information to BCBSF. This release specifically includes, but is not limited to, authorization to release any and all medical records and information associated with (or with reference to) thefollowing conditions: exposure to HIV infection, ARC, AIDS, alcohol or drug dependency, and mental and nervous disorders.I understand that BCBSF may cancel this coverage for all individuals covered by it after giving 90 days notice and that any unearned premiums will be returned to me. I also understand that such action will not be taken solelybecause of the amount of claims paid under this contract.67650 0109<strong>Cover</strong>age under this contract will be provided without evidence of insurability if: (1) I am uninsured at the time of application and between the ages of 19 and 64; and (2) I am not covered by a private insurance policy; and (3)I am not eligible for coverage through a public health insurance program unless that eligibility has lapsed due to no longer meeting income or categorical requirements; and (4) I have not been covered by any health insuranceprogram at any time during the six months immediately prior to applying for this coverage unless coverage under such program was terminated due to: (a) loss of a job that provided an employer-sponsored health benefit plan;or (b) exhaustion of coverage that was continued under COBRA or continuation of coverage requirements under <strong>Florida</strong> Statutes; or (c) reaching the limiting age under the policy; or (d) death of or divorce from a spouse whowas provided an employer-sponsored health benefit plan.I understand <strong>Cover</strong> <strong>Florida</strong> Plan II has a 12-month pre-existing condition limitation for any condition, regardless of the cause of the condition, for which medical advice, diagnosis or treatment was recommended or receivedwithin the 6-month period immediately prior to my effective date of coverage. I understand the 12-month pre-existing condition limitation may be reduced if I have prior creditable coverage that was in effect within 63 daysof the effective date of my coverage under <strong>Cover</strong> <strong>Florida</strong>.Requested Effective Date ________________________________ This date cannot be prior to the application date. Available dates are the 1st, 8th, 15th and 23rd of each month.Applicant’s Signature ___________________________________ Licensed Agent ________________________ Agent Code ________________ Date _____________For BCBSF only(PRINTED AND SIGNATURE)Initial PaymentPlease include a check made payable to <strong>Blue</strong> Cross and <strong>Blue</strong> Shield of <strong>Florida</strong>. The initial payment should match the Premium in Section A above.The application and check should be mailed to: <strong>Blue</strong> Cross and <strong>Blue</strong> Shield of <strong>Florida</strong>, PO Box 45074, Jacksonville, <strong>Florida</strong> 32232-5016.Initial Payment $ _______________________________ (Amount Enclosed)This initial payment is subject to all terms, conditions and representations contained in the application and the coverage applied for. If my application isdenied, I understand that I will not receive a contract and my initial payment will be refunded to me.
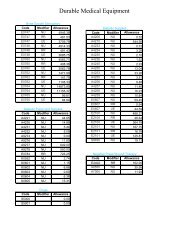
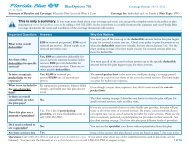
<strong>Cover</strong> <strong>Florida</strong> Disclosure FormI understand that the benefits provided under the <strong>Cover</strong> <strong>Florida</strong> limited benefit plans contain limitationsand exclusions as described in the <strong>Cover</strong> <strong>Florida</strong> Contract. The following is a selected list of some of thoselimitations and exclusions.Benefit Option Selected (check one): [ ] Plan I[ ] Plan IIPlan I – Non-Catastrophic <strong>Cover</strong>ageLimitations include, but are not limited to:• Physician Office, Urgent Care Center andConvenient Care Center visits paid up to $50• Inpatient and Outpatient Hospital covered onlyfor Complications of Pregnancy, up to $50• Durable Medical Equipment, Prosthetics, andOrthotics limited to $500 Per Calendar Year• Outpatient Mental Health Services limited to$500 Per Calendar Year• Prescriptions paid up to $15• Dental Preventive and Basic Services paidup to $50Exclusions include, but are not limited to:• Inpatient and Outpatient Hospital• Emergency Room• Advanced Imaging Services• Substance Dependency• Maternity Care• Ambulance• Home Health Care• Skilled Nursing Facility• HospicePlan II – Catastrophic <strong>Cover</strong>ageLimitations include, but are not limited to:• Physician Office, Urgent Care Center andConvenient Care Center visits paid up to $50• Outpatient Hospital Facility services limitedto Surgical Services only• Inpatient Hospital Services and OutpatientSurgery at a Hospital, Physician’s Office or anEmergency Room• Inpatient Mental Health Services limited to$2,000 Per Calendar Year• Outpatient Mental Health Services limited to$500 Per Calendar Year• Per Admission Deductible $500• Calendar Year Maximum Benefit $25,000• Calendar Year Deductible In-Network $3,000Out-of-Network $6,000• Lifetime Maximum $50,000• Prescriptions paid up to $15• Dental Preventive and Basic Services paidup to $50Exclusions include, but are not limited to:• Substance Dependency• Maternity Care Services• Outpatient Rehabilitative Services andSpinal Manipulations• Skilled Nursing Facility• Pre-existing conditionsThis Disclosure Form must be submitted along with your application to: <strong>Blue</strong> Cross and <strong>Blue</strong> Shield of <strong>Florida</strong>,PO Box 45074, Jacksonville, <strong>Florida</strong> 32232-5016._________________________________________________________________________________________________Signature of ApplicantDate_________________________________________________________________________________________________Printed Name67658-0109
Automatic Payment OptionTake advantage of convenience, security and savings with our Automatic Payment Option.When you enroll in the Automatic Payment Option, we’ll deduct your premium on the date it’s due. Exception: If your duedate is the 1st, your payment will be deducted on the 3rd.Please allow up to four weeks for the completion of the automatic deduction process. If you receive a bill during this time,please pay it as you normally would. Your account will be updated to include that payment. If your payment will be withdrawnfrom an account other than the applicant, the person making your payments (the account holder) should completedthe Authorization form.Easy enrollment1. Complete the Authorization Form2. Print and mail the completed form along with your <strong>Cover</strong> <strong>Florida</strong> application to: <strong>Blue</strong> Cross and <strong>Blue</strong> Shield of <strong>Florida</strong>,PO Box 45074, Jacksonville FL 32232-5016Automatic Payment Authorization Form______________________________________________________________________________________Primary Applicant Name__________________________________________________________________________________Social Security Number____________________________________________________________________________________________________________________________________________________________________________Financial Institution Name____________________________________________________________________________________________________________________________________________________________________________Financial Institution Street Address City State Zip______________________________________________________________________________________ Type of Account: ■ Checking ■ SavingsName on Account______________________________________________________________________________________Account Number______________________________________________________________________________________Routing NumberBy signing up for the Automatic Payment Option, you candecide the frequency of your premium payments.Please choose from one of the following options:■ Monthly (pay every month)■ Bi-monthly (pay every other month)■ Quarterly (pay every three months) ■ Semi-Annually (pay twice a year) ■ Annually (pay once a year)I authorize <strong>Blue</strong> Cross and <strong>Blue</strong> Shield of <strong>Florida</strong> to initiate debits to the financial institution account for the premiumamount. This authority will remain in effect until cancelled by me or with my consent by the financial institution. Thisauthorization is automatically revoked upon cancellation of my coverage. I understand that by revoking the AutomaticPayment Option, my health care coverage payments will change to bi-monthly (every other month) premium billing.________________________________________________________________________________________________________________________Account Holder’s Signature____________________________________________Date________________________________________________________________________________________________________________________Account Holder’s Signature____________________________________________Date54947 0209