Application Form for Provisional Registration of Clinical ...
Application Form for Provisional Registration of Clinical ...
Application Form for Provisional Registration of Clinical ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
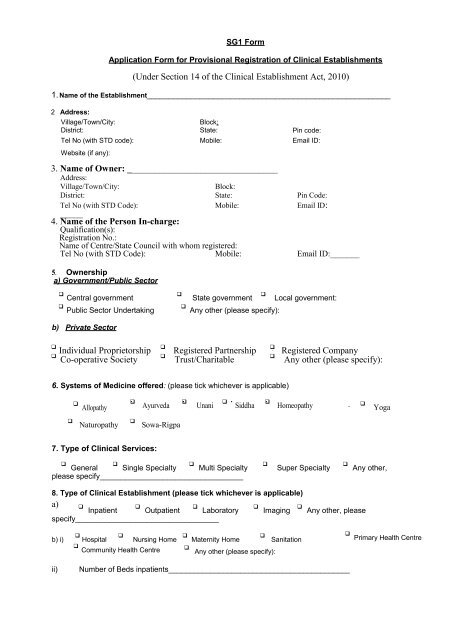
SG1 <strong>Form</strong><strong>Application</strong> <strong>Form</strong> <strong>for</strong> <strong>Provisional</strong> <strong>Registration</strong> <strong>of</strong> <strong>Clinical</strong> Establishments(Under Section 14 <strong>of</strong> the <strong>Clinical</strong> Establishment Act, 2010)1. Name <strong>of</strong> the Establishment_______________________________________________________2 Address:Village/Town/City:Block:District: State: Pin code:Tel No (with STD code): Mobile: Email ID:Website (if any):3. Name <strong>of</strong> Owner: _________________________________Address:Village/Town/City:Block:District: State: Pin Code:Tel No (with STD Code): Mobile: Email ID:_____4. Name <strong>of</strong> the Person In-charge:Qualification(s):<strong>Registration</strong> No.:Name <strong>of</strong> Centre/State Council with whom registered:Tel No (with STD Code): Mobile: Email ID:_______5. Ownershipa) Government/Public Sector Central government Public Sector UndertakingState government Local government: Any other (please specify):b) Private Sector Individual ProprietorshipCo-operative SocietyRegistered PartnershipTrust/CharitableRegistered CompanyAny other (please specify):6. Systems <strong>of</strong> Medicine <strong>of</strong>fered: (please tick whichever is applicable) AllopathyAyurveda UnaniSiddha Homeopathy YogaNaturopathySowa-Rigpa7. Type <strong>of</strong> <strong>Clinical</strong> Services: General Single Specialty Multi Specialtyplease specify__________________________________Super Specialty Any other,8. Type <strong>of</strong> <strong>Clinical</strong> Establishment (please tick whichever is applicable)a) Inpatient Outpatient Laboratoryspecify__________________________________ Imaging Any other, pleaseb) i) Hospital Nursing Home Maternity Home Sanitation Community Health Centre Any other (please specify): Primary Health Centreii)Number <strong>of</strong> Beds inpatients___________________________________________