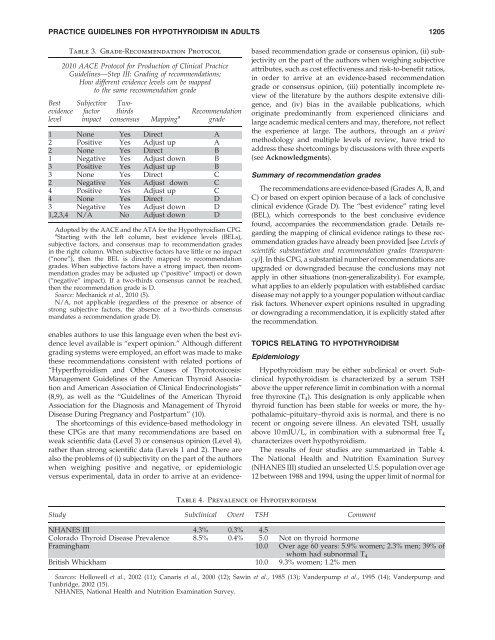
PRACTICE GUIDELINES FOR HYPOTHYROIDISM IN ADULTS 1205BestevidencelevelTable 3. Grade-Recommendation Protocol2010 AACE Protocol <strong>for</strong> Production of <strong>Cl<strong>in</strong>ical</strong> <strong>Practice</strong><strong>Guidel<strong>in</strong>es</strong>—Step III: Grad<strong>in</strong>g of recommendations;How different evidence levels can be mappedto the same recommendation gradeSubjectivefactorimpactTwothirdsRecommendationconsensus Mapp<strong>in</strong>g a grade1 None Yes Direct A2 Positive Yes Adjust up A2 None Yes Direct B1 Negative Yes Adjust down B3 Positive Yes Adjust up B3 None Yes Direct C2 Negative Yes Adjust down C4 Positive Yes Adjust up C4 None Yes Direct D3 Negative Yes Adjust down D1,2,3,4 N/A No Adjust down DAdopted by the AACE and the ATA <strong>for</strong> the <strong>Hypothyroidism</strong> CPG.a Start<strong>in</strong>g with the left column, best evidence levels (BELs),subjective factors, and consensus map to recommendation grades<strong>in</strong> the right column. When subjective factors have little or no impact(‘‘none’’), then the BEL is directly mapped to recommendationgrades. When subjective factors have a strong impact, then recommendationgrades may be adjusted up (‘‘positive’’ impact) or down(‘‘negative’’ impact). If a two-thirds consensus cannot be reached,then the recommendation grade is D.Source: Mechanick et al., 2010 (5).N/A, not applicable (regardless of the presence or absence ofstrong subjective factors, the absence of a two-thirds consensusmandates a recommendation grade D).enables authors to use this language even when the best evidencelevel available is ‘‘expert op<strong>in</strong>ion.’’ Although differentgrad<strong>in</strong>g systems were employed, an ef<strong>for</strong>t was made to makethese recommendations consistent with related portions of‘‘Hyperthyroidism and Other Causes of Thyrotoxicosis:Management <strong>Guidel<strong>in</strong>es</strong> of the American Thyroid Associationand American Association of <strong>Cl<strong>in</strong>ical</strong> Endocr<strong>in</strong>ologists’’(8,9), as well as the ‘‘<strong>Guidel<strong>in</strong>es</strong> of the American ThyroidAssociation <strong>for</strong> the Diagnosis and Management of ThyroidDisease Dur<strong>in</strong>g Pregnancy and Postpartum’’ (10).The shortcom<strong>in</strong>gs of this evidence-based methodology <strong>in</strong>these CPGs are that many recommendations are based onweak scientific data (Level 3) or consensus op<strong>in</strong>ion (Level 4),rather than strong scientific data (Levels 1 and 2). There arealso the problems of (i) subjectivity on the part of the authorswhen weigh<strong>in</strong>g positive and negative, or epidemiologicversus experimental, data <strong>in</strong> order to arrive at an evidencebasedrecommendation grade or consensus op<strong>in</strong>ion, (ii) subjectivityon the part of the authors when weigh<strong>in</strong>g subjectiveattributes, such as cost effectiveness and risk-to-benefit ratios,<strong>in</strong> order to arrive at an evidence-based recommendationgrade or consensus op<strong>in</strong>ion, (iii) potentially <strong>in</strong>complete reviewof the literature by the authors despite extensive diligence,and (iv) bias <strong>in</strong> the available publications, whichorig<strong>in</strong>ate predom<strong>in</strong>antly from experienced cl<strong>in</strong>icians andlarge academic medical centers and may, there<strong>for</strong>e, not reflectthe experience at large. The authors, through an a priorimethodology and multiple levels of review, have tried toaddress these shortcom<strong>in</strong>gs by discussions with three experts(see Acknowledgments).Summary of recommendation gradesThe recommendations are evidence-based (Grades A, B, andC) or based on expert op<strong>in</strong>ion because of a lack of conclusivecl<strong>in</strong>ical evidence (Grade D). The ‘‘best evidence’’ rat<strong>in</strong>g level(BEL), which corresponds to the best conclusive evidencefound, accompanies the recommendation grade. Details regard<strong>in</strong>gthe mapp<strong>in</strong>g of cl<strong>in</strong>ical evidence rat<strong>in</strong>gs to these recommendationgrades have already been provided [see Levels ofscientific substantiation and recommendation grades (transparency)].In this CPG, a substantial number of recommendations areupgraded or downgraded because the conclusions may notapply <strong>in</strong> other situations (non-generalizability). For example,what applies to an elderly population with established cardiacdisease may not apply to a younger population without cardiacrisk factors. Whenever expert op<strong>in</strong>ions resulted <strong>in</strong> upgrad<strong>in</strong>gor downgrad<strong>in</strong>g a recommendation, it is explicitly stated afterthe recommendation.TOPICS RELATING TO HYPOTHYROIDISMEpidemiology<strong>Hypothyroidism</strong> may be either subcl<strong>in</strong>ical or overt. Subcl<strong>in</strong>icalhypothyroidism is characterized by a serum TSHabove the upper reference limit <strong>in</strong> comb<strong>in</strong>ation with a normalfree thyrox<strong>in</strong>e (T 4 ). This designation is only applicable whenthyroid function has been stable <strong>for</strong> weeks or more, the hypothalamic–pituitary–thyroidaxis is normal, and there is norecent or ongo<strong>in</strong>g severe illness. An elevated TSH, usuallyabove 10 mIU/L, <strong>in</strong> comb<strong>in</strong>ation with a subnormal free T 4characterizes overt hypothyroidism.The results of four studies are summarized <strong>in</strong> Table 4.The National Health and Nutrition Exam<strong>in</strong>ation Survey(NHANES III) studied an unselected U.S. population over age12 between 1988 and 1994, us<strong>in</strong>g the upper limit of normal <strong>for</strong>Table 4. Prevalence of <strong>Hypothyroidism</strong>Study Subcl<strong>in</strong>ical Overt TSH CommentNHANES III 4.3% 0.3% 4.5Colorado Thyroid Disease Prevalence 8.5% 0.4% 5.0 Not on thyroid hormoneFram<strong>in</strong>gham 10.0 Over age 60 years: 5.9% women; 2.3% men; 39% ofwhom had subnormal T 4British Whickham 10.0 9.3% women; 1.2% menSources: Hollowell et al., 2002 (11); Canaris et al., 2000 (12); Saw<strong>in</strong> et al., 1985 (13); Vanderpump et al., 1995 (14); Vanderpump andTunbridge, 2002 (15).NHANES, National Health and Nutrition Exam<strong>in</strong>ation Survey.
1206 GARBER ET AL.TSH as 4.5 mIU/mL (11). The prevalence of subcl<strong>in</strong>ical diseasewas 4.3% and of overt disease was 0.3%. The Coloradothyroid disease prevalence survey, <strong>in</strong> which self-selected <strong>in</strong>dividualsattend<strong>in</strong>g a health fair were tested and an uppernormal TSH value of 5.0 mIU/L was used, reported a prevalenceof 8.5% and 0.4% <strong>for</strong> subcl<strong>in</strong>ical and overt disease,respectively, <strong>in</strong> people not tak<strong>in</strong>g thyroid hormone (12). In theFram<strong>in</strong>gham study, 5.9% of women and 2.3% of men over theage of 60 years had TSH values over 10 mIU/L, 39% of whomhad subnormal T 4 levels (13). In the British Whickham survey9.3% of women and 1.2% of men had serum TSH values over10 mIU/L (14,15). The <strong>in</strong>cidence of hypothyroidism <strong>in</strong> womenwas 3.5 per 1000 survivors per year and <strong>in</strong> men it was 0.6 per1000 survivors per year. The risk of develop<strong>in</strong>g hypothyroidism<strong>in</strong> women with positive antibodies and elevated TSHwas 4% per year versus 2%–3% per year <strong>in</strong> those with eitheralone (14,15). In men the relative risk rose even more <strong>in</strong> eachcategory, but the rates rema<strong>in</strong>ed well below those of women.Primary and secondary etiologiesof hypothyroidismEnvironmental iod<strong>in</strong>e deficiency is the most commoncause of hypothyroidism on a worldwide basis (16). In areasof iod<strong>in</strong>e sufficiency, such as the United States, the mostcommon cause of hypothyroidism is chronic autoimmunethyroiditis (Hashimoto’s thyroiditis). Autoimmune thyroiddiseases (AITDs) have been estimated to be 5–10 times morecommon <strong>in</strong> women than <strong>in</strong> men. The ratio varies from seriesto series and is dependent on the def<strong>in</strong>ition of disease,whether it is cl<strong>in</strong>ically evident or not. In the Whickhamsurvey (14), <strong>for</strong> example, 5% of women and 1% of men hadboth positive antibody tests and a serum TSH value > 6.This <strong>for</strong>m of AITD (i.e., Hashimoto’s thyroiditis, chronicautoimmune thyroiditis) <strong>in</strong>creases <strong>in</strong> frequency with age(11), and is more common <strong>in</strong> people with other autoimmunediseases and their families (17–25). Goiter may or may notbe present.AITDs are characterized pathologically by <strong>in</strong>filtration ofthe thyroid with sensitized T lymphocytes and serologicallyby circulat<strong>in</strong>g thyroid autoantibodies. Autoimmunity to thethyroid gland appears to be an <strong>in</strong>herited defect <strong>in</strong> immunesurveillance, lead<strong>in</strong>g to abnormal regulation of immune responsivenessor alteration of present<strong>in</strong>g antigen <strong>in</strong> the thyroid(26,27).One of the keys to diagnos<strong>in</strong>g AITDs is determ<strong>in</strong><strong>in</strong>gthe presence of elevated anti-thyroid antibody titerswhich <strong>in</strong>clude anti-thyroglobul<strong>in</strong> antibodies (TgAb), anti–microsomal/thyroid peroxidase antibodies (TPOAb), andTSH receptor antibodies (TSHRAb). Many patients withchronic autoimmune thyroiditis are biochemically euthyroid.However, approximately 75% have elevated anti-thyroidantibody titers. Once present, these antibodies generallypersist, with spontaneous disappearance occurr<strong>in</strong>g <strong>in</strong>frequently.Among the disease-free population <strong>in</strong> the NHANESsurvey, tests <strong>for</strong> TgAb were positive <strong>in</strong> 10.4% and TPOAb <strong>in</strong>11.3%. These antibodies were more common <strong>in</strong> women thanmen and <strong>in</strong>creased with age. Only positive TPOAb tests weresignificantly associated with hypothyroidism (11). The presenceof elevated TPOAb titers <strong>in</strong> patients with subcl<strong>in</strong>icalhypothyroidism helps to predict progression to overt hypothyroidism—4.3%per year with TPOAb vs. 2.6% per yearwithout elevated TPOAb titers (14,28). The higher risk ofdevelop<strong>in</strong>g overt hypothyroidism <strong>in</strong> TPOAb-positive patientsis the reason that several professional societies and manycl<strong>in</strong>ical endocr<strong>in</strong>ologists endorse measurement of TPOAbs <strong>in</strong>those with subcl<strong>in</strong>ical hypothyroidism.In patients with a diffuse, firm goiter, TPOAb should bemeasured to identify autoimmune thyroiditis. S<strong>in</strong>ce nonimmunologicallymediated mult<strong>in</strong>odular goiter is rarely associatedwith destruction of function<strong>in</strong>g tissue andprogression to hypothyroidism (29), it is important to identifythose patients with the nodular variant of autoimmune thyroiditis<strong>in</strong> whom these risks are significant. In some cases,particularly <strong>in</strong> those with thyroid nodules, f<strong>in</strong>e-needle aspiration(FNA) biopsy helps confirm the diagnosis and to excludemalignancy. Also, <strong>in</strong> patients with documentedhypothyroidism, measurement of TPOAb identifies the cause.In the presence of other autoimmune disease such astype 1 diabetes (20,21) or Addison’s disease (17,18), chromosomaldisorders such as Down’s (30) or Turner’s syndrome(31), and therapy with drugs such as lithium (32–34), <strong>in</strong>terferonalpha (35,36), and amiodarone (37) or excess iod<strong>in</strong>e <strong>in</strong>gestion(e.g., kelp) (38–40), TPOAb measurement may provide prognostic<strong>in</strong><strong>for</strong>mation on the risk of develop<strong>in</strong>g hypothyroidism.TSHRAb may act as a TSH agonist or antagonist (41).Thyroid stimulat<strong>in</strong>g immunoglobul<strong>in</strong> (TSI) and/or thyrotrop<strong>in</strong>b<strong>in</strong>d<strong>in</strong>g <strong>in</strong>hibitory immunoglobul<strong>in</strong> (TBII) levels,employ<strong>in</strong>g sensitive assays, should be measured <strong>in</strong> euthyroidor L-thyrox<strong>in</strong>e–treated hypothyroid pregnant womenwith a history of Graves’ disease because they are predictorsof fetal and neonatal thyrotoxicosis (42). S<strong>in</strong>ce the risk <strong>for</strong>thyrotoxicosis correlates with the magnitude of elevation ofTSI, and s<strong>in</strong>ce TSI levels tend to fall dur<strong>in</strong>g the second trimester,TSI measurements are most <strong>in</strong><strong>for</strong>mative when done<strong>in</strong> the early third trimester. The argument <strong>for</strong> measurementearlier <strong>in</strong> pregnancy is also based, <strong>in</strong> part, on determ<strong>in</strong><strong>in</strong>gwhether establish<strong>in</strong>g a surveillance program <strong>for</strong> ongo<strong>in</strong>gfetal and subsequent neonatal thyroid dysfunction isnecessary (43).<strong>Hypothyroidism</strong> may occur as a result of radioiod<strong>in</strong>e orsurgical treatment <strong>for</strong> hyperthyroidism, thyroid cancer, orbenign nodular thyroid disease and after external beam radiation<strong>for</strong> non–thyroid-related head and neck malignancies,<strong>in</strong>clud<strong>in</strong>g lymphoma. A relatively new pharmacologic causeof iatrogenic hypothyroidism is the tyros<strong>in</strong>e k<strong>in</strong>ase <strong>in</strong>hibitors,most notably sunit<strong>in</strong>ib (44,45), which may <strong>in</strong>duce hypothyroidismthrough reduction of glandular vascularity and <strong>in</strong>ductionof type 3 deiod<strong>in</strong>ase activity.Central hypothyroidism occurs when there is <strong>in</strong>sufficientproduction of bioactive TSH (46,47) due to pituitary or hypothalamictumors (<strong>in</strong>clud<strong>in</strong>g craniopharyngiomas), <strong>in</strong>flammatory(lymphocytic or granulomatous hypophysitis) or<strong>in</strong>filtrative diseases, hemorrhagic necrosis (Sheehan’s syndrome),or surgical and radiation treatment <strong>for</strong> pituitary orhypothalamic disease. In central hypothyroidism, serum TSHmay be mildly elevated, but assessment of serum free T 4 isusually low, differentiat<strong>in</strong>g it from subcl<strong>in</strong>ical primary hypothyroidism.Consumptive hypothyroidism is a rare condition that mayoccur <strong>in</strong> patients with hemangiomata and other tumors <strong>in</strong>which type 3 iodothyron<strong>in</strong>e deiod<strong>in</strong>ase is expressed, result<strong>in</strong>g<strong>in</strong> accelerated degradation of T 4 and triiodothyron<strong>in</strong>e (T 3 )(48,49).