Paediatric diabetes operational 1745.pdf - East Cheshire NHS Trust
Paediatric diabetes operational 1745.pdf - East Cheshire NHS Trust
Paediatric diabetes operational 1745.pdf - East Cheshire NHS Trust

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Paediatric</strong> and Adolescent Diabetes Operational PolicyChildren’s Diabetes MDT Operational Policy May 23, 2012 1
Policy Title:<strong>Paediatric</strong> and Adolescent Diabetes Operational PolicyExecutive Summary:Supersedes:Description ofAmendment(s):The Children’s Diabetes Multidisciplinary Team (MDT) is asmall multi-professional team serving the population of <strong>East</strong><strong>Cheshire</strong> and the surrounding area. The team offers care inline with NICE and NSF guidance. This policy sets out howcare is deliveredNew Policy.This policy will impact on: <strong>Paediatric</strong> <strong>diabetes</strong> services, Adult <strong>diabetes</strong> servicesFinancial Implications: Non KnownPolicy Area: Children’s Services Document Reference:Version Number: 1 Effective Date: August 2012Issued By: Family and Well being Review Date: July 2015Authors:Surendran Chandrasekaranand Nicola BirtwistleImpact AssessmentDate:August 2012APPROVAL RECORDConsultation Phase:Committees / Group<strong>Paediatric</strong>ians, Children’sNurses, Mel BarkerDateJuly-August 2012Clinical Director Familiesand Well Being BUDr A Ho………………..Children’s Service’sManager DBaillie……………….Received for information:Children’s Diabetes MDT Operational Policy May 23, 2012 2
Table of contentsIntroduction……………………………………………………………………Referral Flow chart…………………………………………………………..Purpose of the MDT…………………………………………………………Leadership Arrangements and Responsibilities…………………………The Lead Clinician………………………………………………………The Core Nurse Member……………………………………………Responsibilities of Core Dietician…………………………………….Nursing Qualifications…………………………………………………Membership Arrangements……………………………………………………Out Patient Services……………………………………………………………..In Patient Services………………………………………………………………..MDT Meetings……………………………………………………………………Key Worker Policy…………………………………………………………………Data Collection………………………………………………………………………Provision of Patient‐Centered Care……………………………………………Patient Information………………………………………………………………Patient Feedback…………………………………………………………………Treatments……………………………………………………………………….High HbA1C Policy..................................................................DNA Policy…………………………………………………………………………..Adherence to Guidelines………………………………………………………NICE Guidelines………………………………………………………ISPAD Guidelines…………………………………………………Local Guidelines……………………………………………………Education……………………………………………………………………….Facilities…………………………………………………………………………P4P5P6P7P7P7P8P9P10P10P11P12P12P13P13P13P13P14P15P15P16P16P16P16P16P17This Operation Policy was based on work done by BRADFORD TEACHING HOSPITALS FOUNDATION TRUSTChildren’s Diabetes MDT Operational Policy May 23, 2012 3
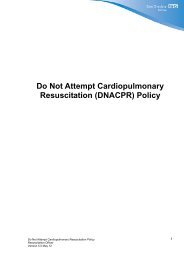
Flow chart for management of new referrals where <strong>diabetes</strong> is suspectedDiagnosis of Diabetes suspectedeither from Primary Care or A+EUrgent referral to Paed Dept via On‐callteam or MDTDiagnosis confirmedInitial treatment plan discussed with Dr Chandrasekaranor Nicola Birtwistle (on‐ call consultant if out of hours)Admission to children’s wardfor initiation of treatmentIf child well without signs of DKA, followtreatment of well child with newlydiagnosed <strong>diabetes</strong> protocol. Commencetreatment with MDI insulin regimeIf child unwell with signs of DKA,follow BSPED DKA guidelinesChild reviewed within 24 hours by Consultant and PDSNfrom MDT. Further treatment decision made by MDT andeducation commenced at appropriate time for family.Dietetic review on the ward prior to discharge.Decisions on timing of discharge made by MDT inconjunction with family. Follow‐up arrangements madeprior to dischargeChildren’s Diabetes MDT Operational Policy May 23, 2012 5
Purpose of the MDTThe aim of the MDT is to help ensure a coordinated approach to the diagnosis, treatmentand on‐going care for all children and young people diagnosed with <strong>diabetes</strong> in <strong>East</strong><strong>Cheshire</strong>.The MDT is committed to achieving the highest standard of care and patientoutcomes through:1. A consistent approach2. Incorporating new research and best practice into patients’ care.3. Providing comprehensive information to patients, carers and their relatives.4. Involving patients in assessment and redesigning of the service.5. Following National and CYPDN guidelines6. The collection of high quality audit data.7. The analysis of such data in audit cycles allied to the CYPDN.8. The involvement in local, national and international research studies.The Operational Policy for the MDT will be reviewed every 2 years at theDiabetes MDT meetings or more frequently according to service needs/changes.Service SpecificationIt is the intention of the <strong>East</strong> <strong>Cheshire</strong> CYPD MDT to work within the framework of Local,National and International <strong>diabetes</strong> guidelines, including NICE, Every Young Person withDiabetes Matters, Diabetes NSF and ISPAD consensus Guidelines.(http://www.ispad.org/FileCenter.html?CategoryID=5)(http://www.nice.org.uk/nicemedia/live/10944/29390/29390.pdf(http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digital asset/dh_073675.pdf)Telephone advice serviceThere is direct telephone access to a member of the <strong>diabetes</strong> team from 9.00am to 5.00pmfive days a week. During this time young people and their families have direct access to theCYPD MDT via the PDSN office number or mobile. Calls will be answered as soon aspossible. The numbers are given to new patients at the time of diagnosis and are includedin the written information given out to families. The consultant will be contactable throughhis secretary at all times during office hours or can be bleeped through switch board if offsite. In the evenings and at weekends families have access to advice via children’s wardand the on call paediatric registrar and consultant. The ward has access to all diabeticguidelines/policies which are kept in a folder in the children’s ward. Policies are alsoaccessible through the stre@mline database and the shared drive.Parents of newly diagnosed children are informed of the access arrangements at diagnosisand existing parents are reminded at outpatient visits and via the twice yearly newsletter.Contact numbers are included in written information given to families at diagnosis. All staffare encouraged to seek assistance from the CYPD team if there is any doubt as to theadvice to be given.The PDSN contacts the ward after the weekend to see if any patients have been admittedover the weekend and will inform the consultant if further advice is required.Children’s Diabetes MDT Operational Policy May 23, 2012 6
Leadership Arrangements and ResponsibilitiesThe Lead ClinicianThe Lead Clinician for the Children’s Diabetes MDT is Dr Surendran Chandrasekaran.Responsibilities of the Lead clinician:• Lead the clinical activity of the multidisciplinary team, workingto agreed guidelines, ensuring a high quality integrated servicewhich meets local, regional and national targets.• Attend and contribute to the North West <strong>Paediatric</strong> Diabetes regionalnetwork meetings or send a representative.• Ensure that the clinical management guidelines are produced andrevised regularly.• Organise “management meetings” of the MDT and ensuredeliberations are recorded.• Establish an audit program and review of outcomes• Ensure an annual report for the CYPDN is produced• Lead on or nominate lead for service improvement.• Overall responsibility for ensuring that MDT work towards meetingpeer review quality measures.• Ensure that the outcomes of the meeting are clearly recorded andclinically validated and that appropriate data collection is supported.• To ensure that guidelines and the Diabetes Networkrecommendations are reviewed and implemented locally.• Take overall responsibility for the function of the MDTCYPDN MembershipThe Lead paediatric <strong>diabetes</strong> clinician will attend the North West <strong>Paediatric</strong> Diabetes regionalNetwork meetings or facilitate the attendance of a nominated representative. The MDT willparticipate in the activities and endeavor to implement developments suggested by theCYPDN.Core Nurse MembersThe Lead and only Nurse for the Children’s Diabetes MDT is Nicola Birtwistle, Band 6. Coverfor her post is by the Children’s Community nursing team.Responsibilities of the PDSN• Working closely with and supporting the lead Physician in their role• Contributing to the multidisciplinary discussion and patientassessment/care planning decisions of the team at their regular meetings• Providing expert nursing advice and support to other health professionals inthe nurses’ specialist area of practice.• Involvement in clinical audit.• Leading on patients’, carers’ and relatives’ communication issues andCo‐ordination of the patients’ pathway for patients referred to the team.• Facilitating access to members of the MDT where requested by patientsChildren’s Diabetes MDT Operational Policy May 23, 2012 7
and their carers.• Contributing to the management of the service.• Utilising research in the nurses’ specialist area of practice.• Act as a role model and expert nurse providing in‐depth highly specialistclinical knowledge to colleagues through MDT meetings, for patients andcarers/relatives.• Lead on audit, identifying areas that require auditing to develop andimprove services.• Promote and support the holistic needs assessment in the managementof <strong>diabetes</strong> care within the Children’s MDT.• Act as a resource for health care professionals by being visible, available, andaccessible for support, counseling and advice in relation to the managementof young people with <strong>diabetes</strong>.• To act as link between Primary and Secondary Care in the implementation ofLocal and national guidance or service initiatives.• Develop links with other specialist areas of care to ensure on‐goingimprovements in the service provision for children with <strong>diabetes</strong> in linewith national guidance.• Provide education and support to schools, nurseries and colleges.• Support the Peer Review process and ensure that service development issupported by specialist nursing.Responsibilities of the Core Dietician• Contributing to the multidisciplinary discussion and patient assessment/careplanning decisions of the team at their regular meetings.• Providing expert dietetic advice to young people and their families fromdiagnosis• Providing expert dietetic advice and support to other health professionals in thedietician’s specialist area of practice.• Leading on the implementation of carbohydrate counting and dose adjustment• Providing advice and training for staff on the ward, and school staff on issuesrelating to dose adjustment and carbohydrate assessment• Involvement in clinical audit.• Contributing to the management of the service.• Utilising research in the dietician’s specialist area of practice.Children’s Diabetes MDT Operational Policy May 23, 2012 8
TrainingDiabetes NurseWithin the <strong>diabetes</strong> service Specialist Nurse Nicola Birtwistle has 18 years of experiencelooking after children with <strong>diabetes</strong>. As well as being a registered general and paediatricnurse she has undertaken a diploma module in <strong>diabetes</strong> and recently completed her degreein Child and family nursing in 2011 and she holds a non medical prescribing qualification.Nicola keeps up to date with pump training courses; she attends relevant symposiums andconferences and is part of the North West <strong>Paediatric</strong> Diabetes NetworkMedicalDr Chandrasekaran completed his training as a General pediatrician with special interest in<strong>diabetes</strong> in 2009. He started as a Consultant in November 2009 and took over Pediatric<strong>diabetes</strong> services at Macclesfield DGH. His training is in line with BSPED recommendations.He has undertaken specific <strong>diabetes</strong> education during pre‐consultant training, including apostgraduate certificate course from the University of Liverpool. He has attended pumptraining course organised by Royal Liverpool University Hospital. He regularly attendsISPAD, BSPED, RCPCH meeting, Nottingham Diabetes Symposium, AND ACDC meetings. Heis part of the North West <strong>Paediatric</strong> Diabetes Network and his team regularly contributes toNPDA.DieticianPost grad diploma in dieteticsPump training courseBritish dietetic association modules in paediatrics which include <strong>diabetes</strong>Training for ward nurses/doctorsTeaching is provided for the ward staff as part of their on‐going professional training and aspart of the new doctor’s induction programme.Children’s Diabetes MDT Operational Policy May 23, 2012 9
Membership Arrangements Members of the MDTCOREMEMBERTeam Member Role CoverSurendranChandrasekaranNicola BirtwistleGeorgina TimsonLead clinicianLead PDSN<strong>Paediatric</strong> DiabetesDieticianS Melanie Hodskinson Admin/secretarial supportall consultantsChildren’sCommunity TeamEXTENDEDDenise Baillie <strong>Paediatric</strong> ManagerDr WaiKaren Bliss/SteveDavisAdult DiabetologistLead Adult DSNsAdrianneSally ChartresDieticianPharmacistOutpatient ServicesThere is a weekly <strong>diabetes</strong> clinic on Monday afternoons between 14:00 – 18:00 in theChildren’s outpatient department at Macclesfield DGH for all young people with <strong>diabetes</strong> upto the age of 16 and for pump patients up to the age of 18. Appointments in the clinic arefor 20 minutes with all team members. If additional time is required with the PDSN ordietician a home visit or nurse led clinic appointment can be arranged outside normal clinictime.Transition clinics (Please see Transition policy)There is a monthly transition clinic, on the 4 th Wednesday of the month for patients fromages 16 to 18, attended by an adult diabetologist and PDSN. The young adult is seen eitherby the adult consultant/PDSN or both.Patients are referred to the transition clinic in school year 11 after their GCSE’s (age 16). Itis hoped that these appointments allow young people the opportunity of meeting the adultteam while still feeling supported by the paediatric team. At the discretion of the MDT itmay be decided that young people will remain with the paediatric service beyond year 12or that they will remain in the transition service for longer than 1 year. This is particularlyrelevant to young people who are attending the CDC and are still attending a special school.Insulin pump patients are referred at the age of 18 to Manchester Royal Infirmary withwhom theCYPD team has developed links. The PDSN aims to attend the first clinic appointment withChildren’s Diabetes MDT Operational Policy May 23, 2012 10
the patient.All ClinicsPatients are all invited by letter to the next outpatient appointment; this is arranged by theMDT at their previous appointment. It is the hospitals responsibility to ensure letters aresent confirming follow up appointment dates and times.At all clinics patients have near patient testing of their HbA1c, so that results are availableat the time of their consultation.The MDT ensures that patients are offered appointments at least every 3 months in linewith national guidelines. New patients are seen on a more regular basis initially dependenton need. We would also arrange earlier review for specific patients if required. This mayinclude patients who have recently changed insulin regime, are running high HbA1c or if acrisis has arisen as highlighted by the family themselves or a member of the MDT.Core members of the MDT will be present at all outpatient clinics and patients will haveaccess to a member of the MDT at all times.Should patients consistently not attend their appointments the DSN will contact thefamilies directly and letters will be sent to both the family and GP highlighting the nonattendanceand further planned course of action.At the beginning of each clinic all patients from clinic are discussed within the MDT. TheMDT will also discuss any other patients where issues have arisen and decisions arerequired.Inpatient careChildren and young people will be admitted to the paediatric ward if they require inpatientcare. Any child admitted with <strong>diabetes</strong> will be discussed with a member of the MDT andadvice will be given on management of their <strong>diabetes</strong> while in hospital. Any in patients willbe reviewed by a member of the MDT within 24 hours of admission to hospital unless theadmission is over a weekend. Out of hours the care of children with <strong>diabetes</strong> will bemanaged by the on call paediatric registrar and consultant. A member of the MDT will oftenbe available for advice if required.Advice on the management of new patients on those admitted with DKA as well as advicefor any children admitted as an emergency with a surgical problem can be found onstre@mline, the intranet and shared drive.Children who are admitted for routine surgery will have already been discussed with theMDT after the child has been seen in the surgical pre admission clinic. Any plans for achange in treatment prior to admission to hospital will have been discussed with the familyby the PDSN. A treatment plan for the admission will have been discussed by the MDT andthis will have been discussed with the nursing staff and documented in the patient’s’ notes.Guidelines for the management of <strong>diabetes</strong> during surgery are available on the intranet andshared drive.Children’s Diabetes MDT Operational Policy May 23, 2012 11
The MDT MeetingsWeekly MeetingsWeekly meetings are held before the Monday clinic to discuss all the patients on the cliniclist. This includes patients who did not attend their appointment the week before. Thesemeetings also give the opportunity for discussion of other patients who are having <strong>diabetes</strong>related problems or are requiring extra input. These meetings are attended by the MDT,PDSN and dieticians. A similar meeting takes place after the transition clinics and includesthe adult <strong>diabetes</strong> team. At the weekly meetings we have the opportunity to discuss othernon‐patient related issues relevant to the MDT.Core members AttendanceCore members of the MDT, are expected to attend at least two‐thirds of the MDT meetings.Attendance will be recorded in the minutes of each meeting. At least two members of theMDT should be present at all meetings.Key worker PolicyThe Key Worker is defined as the main contact and responsible person for the child andfamily throughout their pathway of care, with the overall aim of ensuring the child andfamily are provided with holistic care and support to meet their individual needs.The main elements of the Key Worker role include:• The provision of practical and emotional support to the child/youngperson and family. The co‐ordination and the provision of informationthat is timely and tailored to the age of the child or young person andthe needs of the family, and understood.• Liaison with educational institutions and support reintegration forthe child or young person as well as teaching practical aspects of<strong>diabetes</strong> care.• The teaching and acquisition of skills for the child, youngperson and family as needed.• The contact point for the family or young person for advice orsupport when required. The child or young person’s key worker willbe Nicola Birtwistle and she will be the families’ first port of call. Shewill be supported in her role by the other core members of the MDTat all times. She will also on occasions seek help and advice fromextended members of the team or from outside the MDT should theneed arise.Children’s Diabetes MDT Operational Policy May 23, 2012 12
Data CollectionAuditThe Diabetes MDT takes part annually in the National Diabetes Audit. We will seekassistance in the submission of data from the <strong>Trust</strong>. At the present time no assistance isprovided for the collection of this data. The MDT also submits data to other national<strong>diabetes</strong> audits and surveys.The MDT currently collects local data on an annual basis for audit purposes. Audit data isthen discussed at our MDT service meetings.Admissions InformationData can easily be accessed through streamline database on new patient admissions, DKAadmissions, admission relating to poor diabetic control, and admissions unrelated to<strong>diabetes</strong> such as routine or acute surgical problems. Currently this data is collected verballybut in future we hope to collect this data as part of an annual report. Additionally we recordany admissions during the previous 12 months at the time of patients’ yearly reviews.Clinical Trials/researchWe are involved with studies through the MCRN for example ADDRESS 1 &2. We areinterested in getting involved in SKIPI trial following discussion with our PCT. We have aresearch nurse who actively looks for studies that we can contribute to.Provision of Patient‐Centered CareThe Children’s Diabetes MDT acknowledges the importance of sensitive and appropriatecommunications with patients and their carers. The team continues to develop a servicethat regards patients as partners in achieving the best possible outcomes for them asindividuals. Young people and their families are taught the skills and knowledge about<strong>diabetes</strong> and are encouraged to manage themselves with the support of the team.Provision of patient written informationNewly diagnosed children and young people are provided with verbal and practicalteaching and are given information leaflets and a copy of the newly diagnosed carepathway. This written information includes advice on contacting the team, managingillness, sick day rules and managing hypoglycaemia.Patient and Carer Feedback and InvolvementPatient Feedback/Experience ExerciseA patient satisfaction survey was completed in August 2010 and subsequent changes weremade to the service. This will be repeated again this year.We are currently in the process of seeking the views of pump service users.Children’s Diabetes MDT Operational Policy May 23, 2012 13
Patient InvolvementThere is an active Diabetes UK local support group. The PDSN attends the committeemeetings and most of the organised events.Treatment, Follow up and ScreeningNICE have developed guidelines for the management of a number of different aspects ofpaediatric <strong>diabetes</strong> care. The MDT has tried to implement these recommendations into ourworking practices. We endeavor to provide a service as detailed in the guidelines whereresources allow. The MDT work towards target HbA1c of 58 mmols/mol (7.5 %) whilerecognising that this target is often difficult to achieve.At diagnosis all new patients will be managed by the MDT at the earliest opportunity. Thiswill normally be on the day of admission or within the next 24 hours. It may not be possibleto meet this target at weekends or over Bank Holidays. Ward staff are encouraged tocontact Dr Chandrasekaran or Nicola Birtwistle about all new admissions and they will oftenbe able to provide advice even when not on call. Children will be seen by the consultant orPDSN within 24 hours of admission where possible or the next working day, and will begiven an appointment to see the dieticians within a week post diagnosis. At the time ofadmission young people will be investigated according to recommendations in the NICEguideline as incorporated into our local guidelines. Children who are well will be starteddirectly onto sub‐cutaneous insulin therapy. This will be multiple injection therapy fromdiagnosis. If patients are unwell at the time of admission they will be stabilised onintravenous treatment following the BSPED DKA protocol.During the initial admission the PDSN will commence a structured teaching programme andthis will be continued and completed following discharge. Our specialist dietician willdiscuss dietary issues with the family and young person including provisional advice oncarbohydrate counting and dose adjustment. Further discussions will take place at homefollowing discharge. Families will receive a lot of support at home following diagnosis withregular visits and phone contacts from the PDSN. These visits will continue until the PDSNand the families are happy with the initial management.Patients will be offered follow up appointments at least every 3 months in the clinic. Wherethe need arises patients will be offered earlier reviews either in the consultant or nurselead clinic. At each appointment we will review the young person’s progress and addressany issues that have arisen. Families will also be offered the opportunity of seeing a PDSNand a dietician at all clinics. Currently appointment times are every 20 minutes withadditional time available for nursing and dietetic review.At all outpatient clinics near patient testing will take place so HbA1C will be available for allpatients at the time of their appointments.Each clinic room is equipped with a computer that could enable the downloading of datafrom blood glucose machines and insulin pumps.The MDT follows guidance from NICE on screening. At least annually patients have an MOT.Bloods are obtained for coeliac antibodies at diagnosis. Thyroid functions will be monitoredin all patients annually. In addition, children over the age of 12 years will have their lipidlevels checked, a urine sample is collected for ACR measurements and a blood pressure isobtained. We also collect data on the young person’s HbA1c results and record anyadmissions over the last 12 months. Children over the age of 12 are referred to the districtscreening programme for annual retinal screening.We have the facilities to conduct continuous blood glucose monitoring if this is requiredwith access to our own monitor.For young people who are experiencing problems with their <strong>diabetes</strong> we will endeavor toChildren’s Diabetes MDT Operational Policy May 23, 2012 14
increase the frequency of their appointments and provide increased support with a view toimproving control. This will include home visits, visits to school and telephone support.The MDT offers a pump service to young people where it is felt that pump therapy isindicated. Currently we use the NICE guidelines to aid our decision making on when we canoffer pump therapy. The PDSN and the lead clinician have both attended a pump trainingcourse. We currently have 42 patients on insulin pumps.The service looks after a small number of young people who do not have classical type 1<strong>diabetes</strong>. We have patients with type 2 <strong>diabetes</strong> and <strong>diabetes</strong> associated with othersyndromes. We endeavor to make accurate diagnoses for all our patients and often liaisewith national or international experts for advice on the management of these moreuncommon types of <strong>diabetes</strong>.High HbA1c PolicyChildren that have HbA1c’s above 80mmol/mol (9.5%) are offered extra support andinterventions to help improve control. This is done in collaboration with the family andyoung person and an individual plan is negotiated. These plans may incorporate, troubleshooting, further <strong>diabetes</strong> education, insulin regimen change, more frequent contact viaphone, email, home visits etc, Continuous Glucose Monitoring,Teenagers with persistent high HbA1c’s who are not engaging with their <strong>diabetes</strong> treatmentare assessed to see if CAMHS referral is required.Currently in May 2012 the number of children and young people with an HbA1c above orequal to 9.5% is 23 which is 27% of the case load. The team recognises that this is a higherproportion than they would want. Increased resource to the team should help reduce thisnumber. The team will audit this number on a regular basis.DNA PolicyThe Diabetes team follows the trust paediatric DNA policy which incorporates safeguarding. A child with <strong>diabetes</strong> will never be discharged from follow up and every effort willbe made to engage the family and young person with services. If a child or young persondoes not attend or cancels a pre arranged clinic appointment, another time is given for thenext available clinic slot. If this is more than a month the PDSN will arrange to see the childsooner if this is required.The PDSN will aim to contact the child or young person to see if there are any specificproblems that may be preventing them from attending the clinics especially in the case ofregular non attendees. If the team has safe guarding concerns these will be discussed withthe named nurse for child protection.Escalation policyThe DKA and Safeguarding children policies give guidance on the how to escalate concerns,there is no specific escalation policy relating specifically to <strong>diabetes</strong>.Children’s Diabetes MDT Operational Policy May 23, 2012 15
Adherence to GuidelinesThe MDT looks to work within the framework of Local, National and International <strong>diabetes</strong>guidelines, including NICE, Every Young Person with Diabetes Matters, Diabetes NSF andISPAD consensus Guidelines.(http://www.ispad.org/FileCenter.html?CategoryID=5)(http://www.nice.org.uk/nicemedia/live/10944/29390/29390.pdf)These have been used to inform our local guidelines for the management of DKA, newpatients, hypoglycaemia and the care of young people undergoing surgery amongst others.Our local guidelines are used by the team for management of all aspects of <strong>diabetes</strong> care.The guidelines are currently available on the <strong>Trust</strong> intranet, stre@mline database andshared drive.The guidelines are widely available on trust computers in all areas of the hospital wherechildren and young people with <strong>diabetes</strong> may be seen. The guidelines are presented in aformat that allows printed copies to be made and kept in patient records during anyhospital admissions. The <strong>diabetes</strong> guidelines also provide advice to non‐members of theteam who may be contacted out of hours by children or their families. They include adviceon the management of illness and our sick day rules. This is to help on call teams giveappropriate advice at time when the MDT is unavailable such a weekends and at night.At junior doctor induction sessions access to these local guidelines are discussed so that allmedical staff is aware of their existence and how they can be accessed when required.Psychosocial AssessmentThe Service has recently adopted the Yorkshire and Humber <strong>Paediatric</strong> Diabetes NetworkWellbeing in Diabetes Questionnaire Tool to help the assessment of psychological need inchildren and young people with <strong>diabetes</strong>. Children identified as requiring psychologicalsupport are referred to the local CAMHS team. It is recognized that this is not an adequateservice. We hope with the introduction of the new tariff, psychology services will beimproved.EducationAt the time of diagnosis all new patients and their families will be seen by the coremembers of the MDT within 24 hours of admission unless this occurs at a weekend. It willbe the consultant’s responsibility to discuss the diagnosis with the young person and theirfamily, and to decide on an initial treatment plan. A structured education programme willbe started by the PDSN’s including the administration of insulin injections blood glucosetesting and blood glucose monitoring and the recognition and treatment of hypoglycaemia.The families will also be seen by our specialist dietician and the family will be given adviceabout basic dietary issues. The basis of carbohydrate counting will be discussed. Once theteam and the family are happy that these initial self‐management skills have been learntwe will aim to discharge the young person home.The PDSN’s and dietician will arrange follow up home visits over the next few weeks tosupport the family and to complete the structured education programme. Documentationof progress will be kept in the nursing record. These home visits will continue for as long asis judged necessary by the PDSN’s and the family.Written education material will be given to all families at the time of diagnosis and will bereferred to at future home and hospital visits. Families will also be given contact details forthe team at the time of discharge.Children’s Diabetes MDT Operational Policy May 23, 2012 16
Education will continue throughout the follow up process. This will often be patient led.The form of education offered will be tailored to the needs of each patient and couldinclude topics around specific issues such as travel or the management of illness.Educational opportunities may arise at outpatient attendances or during future home visits.It is important to the MDT that we try to update our advice from time to time as often asaspects of care are forgotten over time.The PDSN has an increasing role in providing support and education within schools. This isparticularly since widespread introduction of multiple daily injection regimes and pumptherapy.The dietician and PDSN run group carbohydrate counting courses for families.‘The goals for <strong>diabetes</strong> education’ are being introduced as a way of documenting youngpeople’s progress with education.FacilitiesChildren requiring admission to hospital will be admitted to children’s ward. The ward hasthe facilities to monitor patients fully and to provide an appropriate level of nursing care forchildren admitted in DKA. This could include 1:1 nursing if required. Resuscitationequipment is provided on both wards and there is a fully equipped stabilization unit on theWard for the management of critically ill children. There are currently no dedicated HDUbeds.Young people over the age of 16 years who have started the transition process will beadmitted to the adult unit via MAU. Responsibility for the care of the young person wouldbe by the adult <strong>diabetes</strong> team.There are ICU facilities at MDGH and young people over the age of 16 would be admitted tothe local ICU for the management of their <strong>diabetes</strong> if the clinical need arose. Youngerchildren who require intensive care would need to be discussed with NWTS who willfacilitate the transfer of critically ill children with <strong>diabetes</strong> should this be required as for allother children in need of specialist intensive care.Children’s Diabetes MDT Operational Policy May 23, 2012 17
Equality Analysis (Impact assessment)What is being assessed? Name of the policy, procedure, proposal, strategy or service:<strong>Paediatric</strong> Diabetes Specialist Team Operational PolicyDetails of person responsible for completing the assessment: Name: Nicola Birtwistle Job title: <strong>Paediatric</strong> Diabetes Specialist Nurse Team: <strong>Paediatric</strong>sState main purpose or aim of the policy, procedure, proposal, strategy or service:(usually the first paragraph of what you are writing. Also include details of legislation,guidance, regulations etc which have shaped or informed the document)The purpose of the Operational Policy is to outline the level of service that is delivered children, young people andtheir families with <strong>diabetes</strong>2. CONSIDERATION OF DATA AND RESEARCHTo carry out the equality analysis you will need to consider information about the people whouse the service and the staff that provide it.2.1 Give details of RELEVANT information available that gives you an understanding of whowill be affected by this documentAll paediatric patients with <strong>diabetes</strong> and their families under the care of Dr Chandrasekaran2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints eitherfrom patients or staff (grievance) relating to the policy, procedure, proposal, strategy orservice or its effects on different groups?)none2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result ofthis document?Children’s Diabetes MDT Operational Policy May 23, 2012 18
no3. ASSESSMENT OF IMPACTNow that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy orservice (part 1) and looked at the data and research you have (part 2), this section asks you toassess the impact of the policy, procedure, proposal, strategy or service on each of the strandslisted below.Children’s Diabetes MDT Operational Policy May 23, 2012 19
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialRACE:to affect, racial groups differently? Yes No xExplain your response: Where there is a patient and/or carers whose first language is not English, staff shouldfollow the trust interpretation and translation policy to arrange telephone & face to face interpretation to ensurethat parents and young people understand information given to them and to gain consent.From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialGENDER (INCLUDING TRANSGENDER):to affect, different gender groups differently? Yes No xExplain your response: No differential impact identified, treatment is the same for all irrespective of gender.DISABILITYFrom the evidence available does the policy, procedure, proposal, strategy or service affect, or havethe potential to affect, disabled people differently? Yes No xExplain your response: If the patient or carers are deaf, then a British sign language interpreter may be needed andwill be accessed in accordance with the trust interpreting policy (in the future staff will have access to signtranslate– an online translation tool used with a webcam). If the patient or carer is blind, then information can be recordedin audio format. If the patient or carer has learning disabilities, staff should ensure information is understood andappropriate methods of communication are used. There is a picture communications book in the CommunicationBox on the ward/dept and staff should be aware of how to access the health facilitator for children with learningdisabilities from <strong>Cheshire</strong> & Wirral Partnership <strong>Trust</strong>. Staff should ensure they have accessed trust learningdisability awareness training.Guidance on helping/approaching patients with disabilities can be found in the trust’s ‘Welcoming people withdisabilities’ booklet (also in the communications box).AGE:From the evidence available does the policy, procedure, proposal, strategy or service, affect, or have the potentiato affect, age groups differently? Yes No Explain your response: The policy only relates to children and young people and their carers who are the users ofthis service.From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialLESBIAN, GAY, BISEXUAL:to affect, lesbian, gay or bisexual groups differently? Yes No xExplain your response: Care and treatment would be the same regardless of sexual orientation. Same sex coupleswould be involved in their child’s care in the same way as heterosexual couples. All staff receive equality andhuman rights training as part of the trust statutory/mandatory training.From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialRELIGION/BELIEF:to affect, religious belief groups differently? Yes No xExplain your response: All different faith groups will have access to the same level of care which can be adapted atime of fasting. For example if a patient was unable to come to clinic, alternative arrangements would be madeand a home visit done if requiredChildren’s Diabetes MDT Operational Policy May 23, 2012 20
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialCARERS:to affect, carers differently? Yes No xExplain your response: See details in above sections.OTHER: EG Pregnant women, people in civil partnerships, human rights issues.From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potentialto affect any other groups differently? Yes No xExplain your response: No other issues identified.4. Safeguarding Assessment ‐ CHILDRENa. Is there a direct or indirect impact upon children? Yes x No b. If yes please describe the nature and level of the impact (consideration to be given to all children; children in aspecific group or area, or individual children. As well as consideration of impact now or in the future; competing/ conflicting impact between different groups of children and young people:Policy only relates to Children and their families so will directly impact children who have <strong>diabetes</strong>. Anyinformation given to children/young people should be age appropriate. There is a picture communications book inthe ward communications box.c. If no please describe why there is considered to be no impact / significant impact on children5. Relevant consultationHaving identified key groups, how have you consulted with them to find out their views andmade sure that the policy, procedure, proposal, strategy or service will affect them in the waythat you intend? Have you spoken to staff groups, charities, national organisations etc?All relevant staff groups have had the opportunity to read and comment on this policy. Policy has been amendedto reflect their opinions.6. APPROVAL – At this point, you should forward the template to:The <strong>Trust</strong>’s Equality and Diversity Lead lynbailey@nhs.netThe Named Nurse for Safeguarding Children melaniebarker@nhs.netEquality and Diversity response:APPROVEDSafeguarding Children response:APPROVEDChildren’s Diabetes MDT Operational Policy May 23, 2012 21
7. Any actions identified: Have you identified any work which you will need to do in thefuture to ensure that the document has no adverse impact?Action Lead Date to be Achieved1. Ensure all staff have been on learning disabilityawareness training2. Ensure all staff aware of communications box andcontentsThis iscovered by<strong>Paediatric</strong>sTheEssentialswhich allstaff attendannuallyAll staff attend annually8. Review Date: July 2015Date completed: August 2012The <strong>Trust</strong>’s Equality and Diversity Lead:The Named Nurse for Safeguarding Children:… Melanie BarkerChildren’s Diabetes MDT Operational Policy May 23, 2012 22