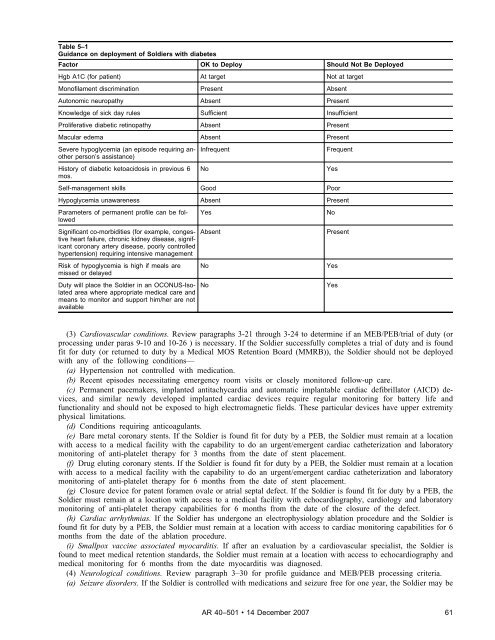
Table 5–1Guidance on deployment of Soldiers with diabetesFactor OK to Deploy Should Not Be DeployedHgb A1C (for patient) At target Not at targetMonofilament discrimination Present AbsentAutonomic neuropathy Absent PresentKnowledge of sick day rules Sufficient InsufficientProliferative diabetic retinopathy Absent PresentMacular edema Absent PresentSevere hypoglycemia (an episode requiring anotherperson’s assistance)History of diabetic ketoacidosis in previous 6mos.InfrequentSelf-management skills Good PoorNoFrequentHypoglycemia unawareness Absent PresentParameters of permanent profile can be followedSignificant co-morbidities (for example, congestiveheart failure, chronic kidney disease, significantcoronary artery disease, poorly controlledhypertension) requiring intensive managementRisk of hypoglycemia is high if meals aremissed or delayedDuty will place the Soldier in an OCONUS-Isolatedarea where appropriate medical care andmeans to monitor and support him/her are notavailableYesAbsentNoNoYesNoPresentYesYes(3) Cardiovascular conditions. Review paragraphs 3-21 through 3-24 to determine if an MEB/PEB/trial of duty (orprocessing under paras 9-10 and 10-26 ) is necessary. If the Soldier successfully completes a trial of duty and is foundfit for duty (or returned to duty by a Medical MOS Retention Board (MMRB)), the Soldier should not be deployedwith any of the following conditions—(a) Hypertension not controlled with medication.(b) Recent episodes necessitating emergency room visits or closely monitored follow-up care.(c) Permanent pacemakers, implanted antitachycardia and automatic implantable cardiac defibrillator (AICD) devi c e s , a n d s i m i l a r n e w l y d e v e l o p e d i m p l a n t e d c a r d i a c d e v i c e s r e q u i r e r e g u l a r m o n i t o r i n g f o r b a t t e r y l i f e a n dfunctionality and should not be exposed to high electromagnetic fields. These particular devices have upper extremityphysical limitations.(d) Conditions requiring anticoagulants.(e) Bare metal coronary stents. If the Soldier is found fit for duty by a PEB, the Soldier must remain at a locationwith access to a medical facility with the capability to do an urgent/emergent cardiac catheterization and laboratorymonitoring of anti-platelet therapy for 3 months from the date of stent placement.(f) Drug eluting coronary stents. If the Soldier is found fit for duty by a PEB, the Soldier must remain at a locationwith access to a medical facility with the capability to do an urgent/emergent cardiac catheterization and laboratorymonitoring of anti-platelet therapy for 6 months from the date of stent placement.(g) Closure device for patent foramen ovale or atrial septal defect. If the Soldier is found fit for duty by a PEB, theSoldier must remain at a location with access to a medical facility with echocardiography, cardiology and laboratorymonitoring of anti-platelet therapy capabilities for 6 months from the date of the closure of the defect.(h) Cardiac arrhythmias. If the Soldier has undergone an electrophysiology ablation procedure and the Soldier isfound fit for duty by a PEB, the Soldier must remain at a location with access to cardiac monitoring capabilities for 6months from the date of the ablation procedure.(i) Smallpox vaccine associated myocarditis. If after an evaluation by a cardiovascular specialist, the Soldier isfound to meet medical retention standards, the Soldier must remain at a location with access to echocardiography andmedical monitoring for 6 months from the date myocarditis was diagnosed.(4) Neurological conditions. Review paragraph 3–30 for profile guidance and MEB/PEB processing criteria.(a) Seizure disorders. If the Soldier is controlled with medications and seizure free for one year, the Soldier may be<strong>AR</strong> <strong>40</strong>–<strong>501</strong> • 14 December 200761
assigned overseas but should not be assigned to areas where access to medications or where the ability to monitoranticonvulsant drug levels are not available.(b) Demyelinating conditions. If a Soldier has been found fit for duty by a PEB (see paragraph 3–30e) for stablenon-disqualifying demyelinating disease, the Soldier should not be subjected to austere environments or where there isno readily available access to environments of equal to or less than 80 degrees Fahrenheit.(5) Asthma. See paragraph 3–27a for profile guidance and for MEB/PEB processing criteria. If it is determined thatthe Soldier can be returned to duty, the Soldier should not deploy if he/she cannot wear protective gear, hasexperienced recent emergency room visits, or requires repetitive use of oral corticosteroids.(6) Sleep apnea. See paragraph 3-41c for profile guidance and for MEB processing criteria. The Soldier can bedeployed if nasal continuous positive airway pressure (CPAP) is required and can be supported in the area ofdeployment. Criteria for the ability to use nasal CPAP in the area of deployment include the following: availability of areliable power source; absence of environmental factors that would render electrical equipment inoperable or unreliable,and the availability of a reliable source of replacement supplies such as masks, harnesses, and filters. A Soldierthat requires nasal CPAP should not be deployed if these factors cannot be assured and the absence of nasal CPAPwould hinder the Soldier from performing his/her military duties.(7) Musculoskeletal. Soldiers with any recent musculoskeletal injury or surgery that prevents necessary mobility orfiring a weapon should not deploy. Any chronic condition that restricts performance in the Soldier’s MOS (forexample, low back pain that prevents lifting) should be referred to an MEB/PEB (or processed under paras 9–10 and10–26). If found fit for duty, the Soldier may be deployed unless he/she cannot function in the specific environment inwhich he/she is being assigned. Soldiers who meet medical retention standards but have a 3 in the profile cannot bedeployed unless cleared by an MMRB.(8) Psychiatric. (See ASD (HA) Policy Guidance for Deployment-Limiting Psychiatric Conditions and Medicationsfor further information.)(a) A psychiatric condition controlled by medication should not automatically lead to non-deployment. Soldiers witha psychiatric disorder in remission or whose residual symptoms do not impair duty performance may be considered fordeployment duties. The commander makes the ultimate decision to deploy after consulting with the treating physicianor other privileged provider. The availability, accessibility, and practicality of a course of treatment or continuation oftreatment in theater or austere environment should be consistent with clinical practice standards. If there are anyquestions on the safety of psychiatric medication, a psychiatrist must be consulted.(b) Psychotic and bipolar disorders are considered disqualifying for deployment.(c) Psychiatric disorders that meet medical retention standards must demonstrate a pattern of stability withoutsignificant symptoms for at least 3 months prior to deployment.(d) Soldiers must demonstrate behavioral stability and minimal potential for deterioration or recurrence of symptomsin a deployed, austere environment, to the extent this can be predicted. The potential for deterioration must beevaluated considering potential environmental demands and individual vulnerabilities.(e) Medication disqualifying for deployment include—1. Antipsychotics used to control psychotic, bipolar, and chronic insomnia symptoms; lithium and anticonvulsants tocontrol bipolar symptoms;2. Medications that require special storage considerations, for example, refrigeration;3. Medications that require laboratory monitoring or special assessments, including lithium, anticonvulsants, andantipsychotics;4. Medication prescribed within 3 months prior to deployment that has yet to demonstrate efficacy or be free ofsignificant impairing side effects.(f) Psychotropics clinically and operationally problematic during deployments include short half-life benzodiazepinesand stimulants. Decisions to deploy personnel on such medications should be balanced with necessity for suchmedication in order to effectively function in a deployed setting, susceptibility to withdrawal symptoms, ability tosecure and procure controlled medications, and potential for medication abuse.(9) History of exertional heat illnesses. See paragraph 3–45 for profile guidance and MEB/PEB criteria. If there isany evidence of significant heat intolerance, the Soldier should not deploy to warm austere climates.(10) Pregnancy. Pregnant Soldiers will not deploy.(11) History of cancer. Soldiers with a history of cancer who have been returned to duty but have a requirement forperiodic monitoring every 6 months or less should not deploy.(12) Chronic infectious diseases (HIV, Hepatitis B or C). Soldiers will not deploy into the combat theater ofoperations. If found fit by a PEB, Soldiers may deploy to Europe or Korea (Host Nation permitting).(13) Abnormal cervical cytology. Soldiers with recently treated moderate or severe dysplasia may only be deployedto austere environments if coordination is arranged via the unit commander and theater surgeon to ensure follow-upevaluation 7 to 9 months after initial evaluation and treatment.(14) Malignant hyperthermia. Soldiers with history of malignant hyperthermia should not be assigned to areas wherecomplete anesthesia services are unavailable or to austere environments.62 <strong>AR</strong> <strong>40</strong>–<strong>501</strong> • 14 December 2007/R<strong>AR</strong> 23 August 2010
- Page 1 and 2:
Army Regulation 40-501Medical Servi
- Page 3 and 4:
HeadquartersDepartment of the ArmyW
- Page 5 and 6:
Contents—ContinuedVascular system
- Page 7 and 8:
Contents—ContinuedChapter 7Physic
- Page 9 and 10:
Contents—ContinuedTable ListTable
- Page 11 and 12:
(See AR 40-29/NAVMEDCOMINST 6120.2/
- Page 13 and 14:
listed in paragraphs 2-3 through 2-
- Page 15 and 16:
d. Current or history of hearing ai
- Page 17 and 18:
82), hip (718.85), ankle and foot (
- Page 19 and 20: . However, for entrance into USMA o
- Page 21 and 22: anch block (426.2), Mobitz type II
- Page 23 and 24: 81) that interfere with normal func
- Page 25 and 26: j. Current or history of congenital
- Page 27 and 28: uniform or protective equipment, or
- Page 29 and 30: Table 2-2Military acceptable weight
- Page 31 and 32: d. Cirrhosis of the liver with recu
- Page 33 and 34: q. Salt-wasting congenital adrenal
- Page 35 and 36: a. Active eye disease or any progre
- Page 37 and 38: (3) Angina pectoris in association
- Page 39 and 40: c. The following profile guidelines
- Page 41 and 42: . All primary muscle disorders incl
- Page 43 and 44: v. Pemphigus. Not responsive to tre
- Page 45 and 46: (2) Asthma. (See para 3-27a.)(3) Al
- Page 47 and 48: (4) Soldiers will be referred to an
- Page 49 and 50: Chapter 4Medical Fitness Standards
- Page 51 and 52: 4-7. EarsThe causes of medical unfi
- Page 53 and 54: (2) Manifest refractive error. Refr
- Page 55 and 56: d. Acute, recurrent sinusitis or ch
- Page 57 and 58: 4-24. Skin and cellular tissuesThe
- Page 59 and 60: . The attending FS/APA/AMNP/AME mak
- Page 61 and 62: Reconnaissance and Surveillance Lea
- Page 63 and 64: n. Lungs and chest wall. Paragraph
- Page 65 and 66: c. Determination of whether of any
- Page 67 and 68: a. Abdomen and gastrointestinal sys
- Page 69: . Asplenic Soldiers are disqualifie
- Page 73 and 74: aggravate the condition and result
- Page 75 and 76: l o c a l F S / A P A / A M N P / A
- Page 77 and 78: Allied documents designed for the s
- Page 79 and 80: (1) Administratively restricted fro
- Page 81 and 82: and will not be aggravated by aviat
- Page 83 and 84: 6-20. Waiver and suspension authori
- Page 85 and 86: as “no field duty,” or “no ov
- Page 87 and 88: this regulation. The approving auth
- Page 89 and 90: organic solvent vapors above permis
- Page 91 and 92: authority for permanent “3” or
- Page 93 and 94: Table 7-2Profile codes*Code Descrip
- Page 95 and 96: their unit commanders. This reporti
- Page 97 and 98: 8-12. Medical examination requireme
- Page 99 and 100: equired. The requirements in paragr
- Page 101 and 102: Army, regardless of component. All
- Page 103 and 104: assessments because resources are b
- Page 105 and 106: (3) If the test is positive, you wi
- Page 107 and 108: (6) Soldiers who fail a Level II ev
- Page 109 and 110: Table 8-1Recording of medical exami
- Page 111 and 112: Table 8-1Recording of medical exami
- Page 113 and 114: Table 8-3Results of Speech Recognit
- Page 115 and 116: Chapter 9Army Reserve Medical Exami
- Page 117 and 118: medical evaluation that provides a
- Page 119 and 120: 10-9. Immunizationsa. Immunization
- Page 121 and 122:
chapter 7 and table 7-1, that the D
- Page 123 and 124:
and the examination information. Ev
- Page 125 and 126:
equired dental examinations and Sol
- Page 127 and 128:
. Medical Readiness Class 2 (MR2)(1
- Page 129 and 130:
AR 600-8-24Officer Transfers and Di
- Page 131 and 132:
AR 350-1Army Training and Leader De
- Page 133 and 134:
5 USC 552a(b)7Public information; a
- Page 135 and 136:
DD Form 2795Pre-Deployment Health A
- Page 137 and 138:
GlossarySection IAbbreviationsAAaer
- Page 139 and 140:
CGcommanding generalCHAMPConsortium
- Page 141 and 142:
FEDS_HEALFederal Strategic Health A
- Page 143 and 144:
JFTRJoint Federal Travel Regulation
- Page 145 and 146:
OCONUSoutside continental United St
- Page 147 and 148:
SEREsurvival, evasion, resistance,
- Page 149 and 150:
WTUWarrior Transition UnitSection I
- Page 151 and 152:
UNCLASSIFIED PIN 015562-000