Australian Mesothelioma Register Report 2002 - Safe Work Australia
Australian Mesothelioma Register Report 2002 - Safe Work Australia
Australian Mesothelioma Register Report 2002 - Safe Work Australia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
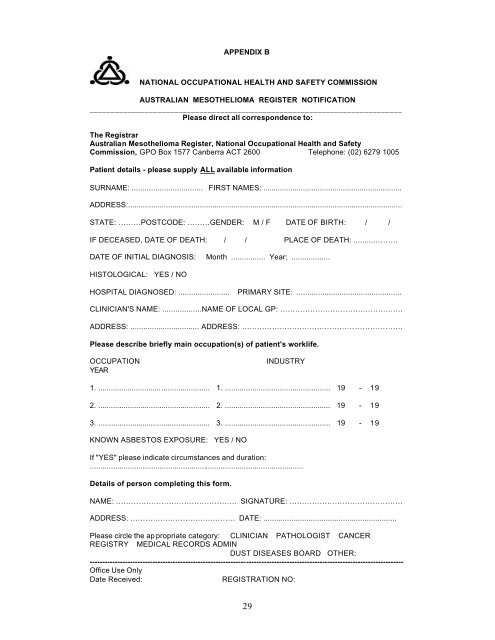
APPENDIX BNATIONAL OCCUPATIONAL HEALTH AND SAFETY COMMISSIONAUSTRALIAN MESOTHELIOMA REGISTER NOTIFICATION__________________________________________________________________________Please direct all correspondence to:The Registrar<strong><strong>Australia</strong>n</strong> <strong>Mesothelioma</strong> <strong>Register</strong>, National Occupational Health and <strong>Safe</strong>tyCommission, GPO Box 1577 Canberra ACT 2600 Telephone: (02) 6279 1005Patient details - please supply ALL available informationSURNAME: ................................. FIRST NAMES: ..................................................................ADDRESS:..................................................................................................................................STATE: ………POSTCODE: ………GENDER: M / F DATE OF BIRTH: / /IF DECEASED, DATE OF DEATH: / / PLACE OF DEATH: ..........………DATE OF INITIAL DIAGNOSIS: Month ................ Year: ..................HISTOLOGICAL: YES / NOHOSPITAL DIAGNOSED: ........................ PRIMARY SITE: .................................................CLINICIAN'S NAME: ..................NAME OF LOCAL GP: ………………………………………….ADDRESS: ................................ ADDRESS: ……………………………………………………….Please describe briefly main occupation(s) of patient's worklife.OCCUPATIONYEARINDUSTRY1. ..................................................... 1. .................................................. 19 - 192. ..................................................... 2. .................................................. 19 - 193. ..................................................... 3. .................................................. 19 - 19KNOWN ASBESTOS EXPOSURE: YES / NOIf "YES" please indicate circumstances and duration:.....................................................................................................Details of person completing this form.NAME: ………………………………………… SIGNATURE: ………………………………………ADDRESS: …………………………………… DATE: ..............................................................Please circle the ap propriate category: CLINICIAN PATHOLOGIST CANCERREGISTRY MEDICAL RECORDS ADMINDUST DISEASES BOARD OTHER:----------------------------------------------------------------------------------------------------------------------------Office Use OnlyDate Received:REGISTRATION NO:29