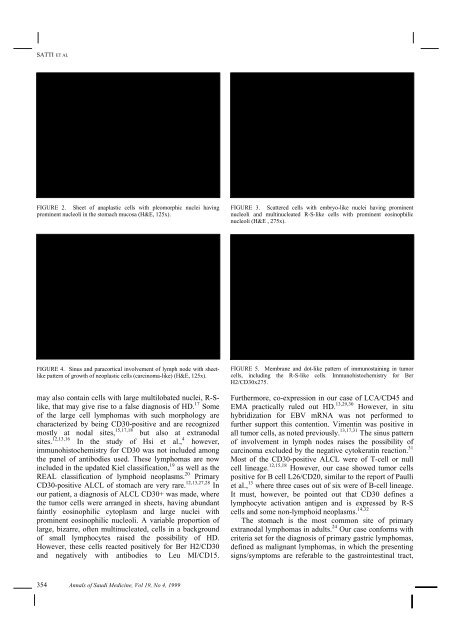
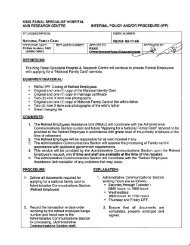
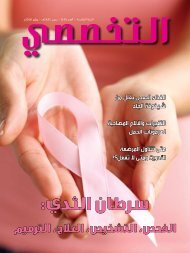
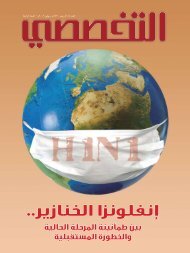
CASE REPORT: <strong>ANAPLASTIC</strong> <strong>LARGE</strong> <strong>CELL</strong> <strong>LYMPHOMA</strong>E29/EMA (Dako), CD3 (Dako), Vimentin (Dako), andAEI-AE3 Cytokeratin (Boehringer Mannheim) wasperformed.ResultsGross examination of the partially resected 12x7x4 cmstomach revealed an exophytic 5x4 cm gastric tumor,which was infiltrating up to the serosa and had a fish-fleshgray-white cut surface. The resection margins were free ofthe tumor. Several perigastric lymph nodes submitted alsoshowed fish-flesh homogenous appearance.In 1994, based on the anaplastic morphology of thegastric neoplasm, the presence of Reed-Sternberg-like (R-S-like) cells and a negative cytokeratin on immunohistochemistry,a diagnosis of Hodgkin’s disease of thestomach was given. Based on this diagnosis, therapy wasstarted.Review of the case in 1998 in a retrospective study ofgastric malignancies revealed a gastric tumor with surfaceulceration of a mucosal neoplasm that extended deep intothe wall and serosa. The tumor was formed of sheets ofpleomorphic cells, with small and large embryo-likemultilobated nuclei having prominent nucleoli andabundant cytoplasm (Figure 2). A variable proportion ofsmall lymphocytic cells were seen, but eosinophils andneutrophils were very scanty. A few binucleate R-S-likecells were seen (Figure 3), in addition to rare cells withbizarre wreath-like multilobated nuclei. A transitionbetween the relatively small-size tumor cells and the largermultinucleated cells was always observed. The lymphnodes showed the same histology with a sinus, carcinomalikepattern of involvement being very apparent (Figure 4).The majority of the neoplastic cells, including the giantR-S-like forms, reacted positively for <strong>CD30</strong> in amembrane- and dot-like pattern and negatively for CD15antibodies (Figure 5). They were also positive for CD45,vimentin and focally positive for EMA. Reaction for T-cellCD45RO and CD3 was negative, while a few tumor cellsreacted positively for B-cells CD20 antibodies. Thepancytokeratin marker AE1-AE3 was negative in thetumor cells. The pleomorphic morphology of this lymphoidneoplasm, the sheet-like and sinus pattern of involvementof lymph nodes, combined with the immunohistochemicalreaction of the tumor cells, reclassifies this neoplasm asprimary gastric <strong>CD30</strong> (Ki-1)-positive ALCL stage II (IE),due to perigastric lymph node involvement. In situhybridization for EBV mRNA was not performed.The postoperative course was uneventful. Subsequentbone marrow aspiration did not show evidence oflymphomatous infiltration. Chemotherapy was started andthe patient received 6 cycles of COPP and ABVD monthlyon an alternate basis over six months. Uppergastrointestinal endoscopy done eight months after surgerywas normal. Biopsies obtained through endoscopy showedfocal collections of plasma cells and eosinophils with areasof intestinal metaplasia, but no evidence of recurrent orresidual malignancy. Repeat CT scan of the abdomenshortly after the endoscopy showed normal stomach. Therewas no evidence of para-aortic lymph node enlargement.At the latest follow-up in February 1998, almost four yearsafter the diagnosis, the patient was alive and well with noevidence of residual tumor, clinically or at endoscopy.DiscussionPresentation of Hodgkin’s disease (HD) as a localizedextranodal process unassociated with lymphatic tissueinvolvement is quite rare, occurring in less than 1% ofpatients with HD. 5 In the NCI study, 6 only six patientswith a histologically reconfirmed diagnosis of HD wereidentified during the period 1953-1990. Of all six cases,however, four involved the stomach. Such a rare diagnosisshould, therefore, be confirmed by combined classichistopathologic and immunophenotypic features. 7,8,10,11This is supported by the fact that in several retrospectivestudies the cases that were originally diagnosed as HDwere all re-classified as NHL of a large cell type after reexamination.9,22 Therefore, the predominant gastriclymphoid malignancy is NHL, 1,4 which has increased infrequency, in contrast to gastric carcinoma, which hasshown a decline in both incidence and mortality rates overthe past few decades. 23,24 These lymphomas were originallyclassified according to criteria developed for nodallymphomas. 25,26 However, with the recent adoption of theconcept of MALT, 2,3 most of these lymphomas have beenclassified as low- and high-grade MALT-lymphomas, 4characterized by the presence of lymphoepithelial lesions(LEL). Only 12 of the 60 cases reported by Hsi et al. 4lacked LEL and were thus classified as diffuse large celllymphomas (DLCL). Some of these gastric DLCL mayassume a pleomorphic anaplastic morphology, with sheetlikegrowth pattern that may simulate carcinoma 12 andFIGURE 1. CT scan of the abdomen, showing thickened gastric pyloricregion with polypoidal projections from its wall.Annals of Saudi Medicine, Vol 19, No 4, 1999 353
SATTI ET ALFIGURE 2. Sheet of anaplastic cells with pleomorphic nuclei havingprominent nucleoli in the stomach mucosa (H&E, 125x).FIGURE 3. Scattered cells with embryo-like nuclei having prominentnucleoli and multinucleated R-S-like cells with prominent eosinophilicnucleoli (H&E , 275x).FIGURE 4. Sinus and paracortical involvement of lymph node with sheetlikepattern of growth of neoplastic cells (carcinoma-like) (H&E, 125x).may also contain cells with large multilobated nuclei, R-Slike,that may give rise to a false diagnosis of HD. 17 Someof the large cell lymphomas with such morphology arecharacterized by being <strong>CD30</strong>-positive and are recognizedmostly at nodal sites, 15,17,18 but also at extranodalsites. 12,13,16 In the study of Hsi et al., 4 however,immunohistochemistry for <strong>CD30</strong> was not included amongthe panel of antibodies used. These lymphomas are nowincluded in the updated Kiel classification, 19 as well as theREAL classification of lymphoid neoplasms. 20 Primary<strong>CD30</strong>-positive ALCL of stomach are very rare. 12,13,27,28 Inour patient, a diagnosis of ALCL <strong>CD30</strong>+ was made, wherethe tumor cells were arranged in sheets, having abundantfaintly eosinophilic cytoplasm and large nuclei withprominent eosinophilic nucleoli. A variable proportion oflarge, bizarre, often multinucleated, cells in a backgroundof small lymphocytes raised the possibility of HD.However, these cells reacted positively for Ber H2/<strong>CD30</strong>and negatively with antibodies to Leu MI/CD15.FIGURE 5. Membrane and dot-like pattern of immunostaining in tumorcells, including the R-S-like cells. Immunohistochemistry for BerH2/<strong>CD30</strong>x275.Furthermore, co-expression in our case of LCA/CD45 andEMA practically ruled out HD. 13,29,30 However, in situhybridization for EBV mRNA was not performed tofurther support this contention. Vimentin was positive inall tumor cells, as noted previously. 13,17,31 The sinus patternof involvement in lymph nodes raises the possibility ofcarcinoma excluded by the negative cytokeratin reaction. 31Most of the <strong>CD30</strong>-positive ALCL were of T-cell or nullcell lineage. 12,15,18 However, our case showed tumor cellspositive for B cell L26/CD20, similar to the report of Paulliet al., 13 where three cases out of six were of B-cell lineage.It must, however, be pointed out that <strong>CD30</strong> defines alymphocyte activation antigen and is expressed by R-Scells and some non-lymphoid neoplasms. 14,32The stomach is the most common site of primaryextranodal lymphomas in adults. 24 Our case conforms withcriteria set for the diagnosis of primary gastric lymphomas,defined as malignant lymphomas, in which the presentingsigns/symptoms are referable to the gastrointestinal tract,354 Annals of Saudi Medicine, Vol 19, No 4, 1999