Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester
Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester
Diagnostic Criteria for Nonviable Pregnancy Early in the First Trimester

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
T h e n e w e ngl a nd j o u r na l o f m e dic i n eTable 1. Term<strong>in</strong>ology and <strong>Diagnostic</strong> Tests Used <strong>Early</strong> <strong>in</strong> <strong>the</strong> <strong>First</strong> <strong>Trimester</strong> of <strong>Pregnancy</strong>.Term<strong>in</strong>ologyViable<strong>Nonviable</strong>Intrauter<strong>in</strong>e pregnancyof uncerta<strong>in</strong> viability<strong>Pregnancy</strong> of unknown location<strong>Diagnostic</strong> testsHuman chorionic gonadotrop<strong>in</strong>(hCG)Pelvic ultrasonography†CommentsA pregnancy is viable if it can potentially result <strong>in</strong> a liveborn baby.A pregnancy is nonviable if it cannot possibly result <strong>in</strong> a liveborn baby. Ectopicpregnancies and failed <strong>in</strong>trauter<strong>in</strong>e pregnancies are nonviable.A woman is considered to have an <strong>in</strong>trauter<strong>in</strong>e pregnancy of uncerta<strong>in</strong> viabilityif transvag<strong>in</strong>al ultrasonography shows an <strong>in</strong>trauter<strong>in</strong>e gestational sac withno embryonic heartbeat (and no f<strong>in</strong>d<strong>in</strong>gs of def<strong>in</strong>ite pregnancy failure).*A woman is considered to have a pregnancy of unknown location if she has apositive ur<strong>in</strong>e or serum pregnancy test and no <strong>in</strong>trauter<strong>in</strong>e or ectopic pregnancyis seen on transvag<strong>in</strong>al ultrasonography.Serum hCG concentration is measured with <strong>the</strong> use of <strong>the</strong> World HealthOrganization 3rd or 4th International Standard.A positive serum pregnancy test is def<strong>in</strong>ed by a serum hCG concentration abovea positivity threshold (5 mIU/ml).M<strong>in</strong>imum quality criteria <strong>in</strong>clude transvag<strong>in</strong>al assessment of <strong>the</strong> uterus andadnexa and transabdom<strong>in</strong>al evaluation <strong>for</strong> free <strong>in</strong>traperitoneal fluid and amass high <strong>in</strong> <strong>the</strong> pelvis; oversight provided by an appropriately tra<strong>in</strong>ed physician;scans per<strong>for</strong>med by providers and <strong>in</strong>terpreted by physicians, all ofwhom meet at least m<strong>in</strong>imum tra<strong>in</strong><strong>in</strong>g or certification standards <strong>for</strong> ultrasonography,<strong>in</strong>clud<strong>in</strong>g transvag<strong>in</strong>al ultrasonography; and scann<strong>in</strong>g equipmentpermitt<strong>in</strong>g adequate visualization of structures early <strong>in</strong> <strong>the</strong> first trimester.* In a woman with a positive ur<strong>in</strong>e or serum pregnancy test, an <strong>in</strong>trauter<strong>in</strong>e fluid collection with rounded edges conta<strong>in</strong><strong>in</strong>gno yolk sac or embryo is most likely a gestational sac; it is certa<strong>in</strong> to be a gestational sac if it conta<strong>in</strong>s a yolk sac orembryo.† Transabdom<strong>in</strong>al imag<strong>in</strong>g without transvag<strong>in</strong>al scann<strong>in</strong>g may be sufficient <strong>for</strong> diagnos<strong>in</strong>g early pregnancy failure whenan embryo whose crown–rump length is 15 mm or more has no visible cardiac activity.negative diagnosis — fail<strong>in</strong>g to diagnose a pregnancyas nonviable. For ei<strong>the</strong>r an <strong>in</strong>trauter<strong>in</strong>epregnancy of uncerta<strong>in</strong> viability or a pregnancyof unknown location, <strong>the</strong> consequence of a falsepositive diagnosis of nonviability may be dire:medical or surgical <strong>in</strong>tervention that elim<strong>in</strong>atesor severely damages a viable pregnancy. This ismuch worse than <strong>the</strong> consequence of a falsenegative diagnosis <strong>in</strong> women with an <strong>in</strong>trauter<strong>in</strong>epregnancy of uncerta<strong>in</strong> viability: a delay (usuallyby a few days) <strong>in</strong> <strong>in</strong>tervention <strong>for</strong> a failed pregnancy.Likewise, <strong>for</strong> a pregnancy of unknownlocation, harm<strong>in</strong>g a potentially normal <strong>in</strong>trauter<strong>in</strong>epregnancy is considerably worse than <strong>the</strong>possible consequence of a false negative diagnosis:a short delay <strong>in</strong> treatment of an ectopic pregnancy<strong>in</strong> a woman who is be<strong>in</strong>g followed medicallyand has no ultrasonographically identifiableadnexal mass.Thus, <strong>the</strong> criteria <strong>for</strong> diagnos<strong>in</strong>g nonviability<strong>in</strong> early pregnancy should virtually elim<strong>in</strong>atefalse positive results. That is, <strong>the</strong> goal is a specificityof 100%, which yields a positive predictivevalue of 100% <strong>for</strong> nonviability, regardless of <strong>the</strong>prior probability of that diagnosis. We recognizethat this goal cannot always be achieved <strong>in</strong>cl<strong>in</strong>ical practice because of <strong>the</strong> dependence ofultra sonography on <strong>the</strong> expertise of <strong>the</strong> operatorand because of statistical limitations <strong>in</strong>rul<strong>in</strong>g out very rare events. However, we areconfident that current data allow us to achievea specificity extremely close to 100%. Althoughit would be ideal to have both high sensitivityand high specificity, diagnosis of early pregnancyfailure requires a focus on <strong>the</strong> latter at<strong>the</strong> expense of <strong>the</strong> <strong>for</strong>mer. 4,9Research <strong>in</strong> <strong>the</strong> past 2 to 3 years 10-12 has shownthat previously accepted criteria <strong>for</strong> rul<strong>in</strong>g out aviable pregnancy, which were based on smallnumbers of patients, 9 are not str<strong>in</strong>gent enoughto avoid false positive test results. Dissem<strong>in</strong>ationof this new <strong>in</strong><strong>for</strong>mation to practitioners and <strong>the</strong>achievement of standardized practice protocolsare challeng<strong>in</strong>g, because <strong>the</strong> diagnosis and managementof early-pregnancy complications <strong>in</strong>volvephysicians from multiple specialties, <strong>in</strong>clud<strong>in</strong>gradiology, obstetrics and gynecology, emergencymedic<strong>in</strong>e, and family medic<strong>in</strong>e. As a result, <strong>the</strong>re1444n engl j med 369;15 nejm.org october 10, 2013The New England Journal of Medic<strong>in</strong>eDownloaded from nejm.org on October 10, 2013. For personal use only. No o<strong>the</strong>r uses without permission.Copyright © 2013 Massachusetts Medical Society. All rights reserved.
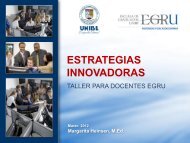
current conceptsAB19.1 mm+ +Figure 1. <strong>Early</strong> Intrauter<strong>in</strong>e Gestational Sac.A transvag<strong>in</strong>al ultrasonogram obta<strong>in</strong>ed at 5 weeks of gestation (Panel A) shows a small, round, fluidfilled structure(arrow), which was confirmed to be an early <strong>in</strong>trauter<strong>in</strong>e pregnancy 4 weeks later (Panel B) on a followup scan show<strong>in</strong>ga fetus measur<strong>in</strong>g 19.1 mm, correspond<strong>in</strong>g to approximately 9 weeks of gestational age. Plus signs <strong>in</strong>dicate calipers.is a patchwork of sometimes conflict<strong>in</strong>g, oftenoutdated published recommendations and guidel<strong>in</strong>esfrom professional societies. 13In this review, we exam<strong>in</strong>e <strong>the</strong> diagnosis ofnonviability <strong>in</strong> early <strong>in</strong>trauter<strong>in</strong>e pregnancy ofuncerta<strong>in</strong> viability and <strong>in</strong> early pregnancy of unknownlocation separately, focus<strong>in</strong>g ma<strong>in</strong>ly on<strong>the</strong> <strong>in</strong>itial (or only) ultrasonographic study per<strong>for</strong>meddur<strong>in</strong>g <strong>the</strong> pregnancy. Our recommendationsare meant to apply to any practice, subspecialtyor community-based, that meets at least<strong>the</strong> m<strong>in</strong>imum quality criteria <strong>for</strong> pelvic ultrasonographylisted <strong>in</strong> Table 1.Di agnos<strong>in</strong>g Pr egna nc y Fa ilur e<strong>in</strong> a n In tr au ter <strong>in</strong>e Pr egna nc yof Uncerta <strong>in</strong> V i a bilit yThe sequence of events <strong>in</strong> early pregnancy, as seenon transvag<strong>in</strong>al ultrasonography, follows a fairlypredictable pattern. The gestational sac is first seenat approximately 5 weeks of gestational age, 14,15appear<strong>in</strong>g as a small cystic-fluid collection withrounded edges and no visible contents, located <strong>in</strong><strong>the</strong> central echogenic portion of <strong>the</strong> uter us (i.e.,with<strong>in</strong> <strong>the</strong> decidua). Previously described ultrasonographicsigns of early pregnancy — <strong>the</strong>“double sac sign” 16 and “<strong>in</strong>tradecidual sign” 17— were def<strong>in</strong>ed with <strong>the</strong> use of transabdom<strong>in</strong>alultrasonography, but with current transvag<strong>in</strong>alultrasono graphic technology, <strong>the</strong>se signs are absent<strong>in</strong> at least 35% of gestational sacs. 18 There<strong>for</strong>e,any round or oval fluid collection <strong>in</strong> awoman with a positive pregnancy test mostlikely represents an <strong>in</strong>trauter<strong>in</strong>e gestational sac(Fig. 1) 19,20 and should be reported as such; it ismuch less likely to be a pseudogestational sacor decidual cyst, f<strong>in</strong>d<strong>in</strong>gs that can be present <strong>in</strong>a woman with an ectopic pregnancy. 21,22The yolk sac, a circular structure about 3 to5 mm <strong>in</strong> diameter, makes its appearance atabout 5 1 ∕2 weeks of gestation. The embryo is firstseen adjacent to <strong>the</strong> yolk sac at about 6 weeks, atwhich time <strong>the</strong> heartbeat is present as a flicker<strong>in</strong>gmotion. 14,15Variations from <strong>the</strong> expected pattern of developmentare worrisome or, if major, def<strong>in</strong>itive <strong>for</strong>early pregnancy failure. The criteria most oftenused to diagnose pregnancy failure are <strong>the</strong> absenceof cardiac activity by <strong>the</strong> time <strong>the</strong> embryohas reached a certa<strong>in</strong> length (crown–rump length),<strong>the</strong> absence of a visible embryo by <strong>the</strong> time <strong>the</strong>gestational sac has grown to a certa<strong>in</strong> size (meansac diameter), and <strong>the</strong> absence of a visible embryoby a certa<strong>in</strong> po<strong>in</strong>t <strong>in</strong> time.Crown–Rump Length as a Criterion<strong>for</strong> Failed <strong>Pregnancy</strong>Shortly after transvag<strong>in</strong>al ultrasonography becamewidely available <strong>in</strong> <strong>the</strong> mid-to-late 1980s,n engl j med 369;15 nejm.org october 10, 2013 1445The New England Journal of Medic<strong>in</strong>eDownloaded from nejm.org on October 10, 2013. For personal use only. No o<strong>the</strong>r uses without permission.Copyright © 2013 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n eTable 2. Guidel<strong>in</strong>es <strong>for</strong> Transvag<strong>in</strong>al Ultrasonographic Diagnosis of <strong>Pregnancy</strong> Failure <strong>in</strong> a Woman with an Intrauter<strong>in</strong>e<strong>Pregnancy</strong> of Uncerta<strong>in</strong> Viability.*F<strong>in</strong>d<strong>in</strong>gs <strong>Diagnostic</strong> of <strong>Pregnancy</strong> FailureCrown–rump length of ≥7 mm and no heartbeatMean sac diameter of ≥25 mm and no embryoAbsence of embryo with heartbeat ≥2 wk after a scanthat showed a gestational sac without a yolk sacAbsence of embryo with heartbeat ≥11 days after ascan that showed a gestational sac with a yolk sacF<strong>in</strong>d<strong>in</strong>gs Suspicious <strong>for</strong>, but Not <strong>Diagnostic</strong> of, <strong>Pregnancy</strong> Failure†Crown–rump length of 7 mm)Small gestational sac <strong>in</strong> relation to <strong>the</strong> size of <strong>the</strong> embryo (
T h e n e w e ngl a nd j o u r na l o f m e dic i n epregnancies. 10,35 In addition, <strong>the</strong> <strong>in</strong>ter observervariation <strong>in</strong> <strong>the</strong> measurement of <strong>the</strong> mean sacdiameter is ±19%, 32 so a diameter of 21 mm (<strong>the</strong>upper limit above) as measured by one observermay be 19% greater, or 25 mm, when measuredby ano<strong>the</strong>r observer.These studies, <strong>in</strong> comb<strong>in</strong>ation, suggest that itis prudent to use a cutoff of 25 mm (ra<strong>the</strong>r than16 mm) <strong>for</strong> <strong>the</strong> mean sac diameter with no visibleembryo (Table 2) <strong>in</strong> diagnos<strong>in</strong>g failed pregnancy(Fig. 2B and 2C). This would yield a specificityand positive predictive value of 100% (or as closeto 100% as can be determ<strong>in</strong>ed). When <strong>the</strong> meansac diameter is 16 to 24 mm, <strong>the</strong> lack of an embryois suspicious <strong>for</strong>, though not diagnostic of,failed pregnancy (Fig. S2 <strong>in</strong> <strong>the</strong> SupplementaryAppendix).Time-based <strong>Criteria</strong> <strong>for</strong> Failed <strong>Pregnancy</strong>Not all failed pregnancies ever develop a 7-mmembryo or a 25-mm gestational sac, so it is importantto have o<strong>the</strong>r criteria <strong>for</strong> diagnos<strong>in</strong>gpregnancy failure. The most useful of such criteria<strong>in</strong>volve nonvisualization of an embryo by acerta<strong>in</strong> po<strong>in</strong>t <strong>in</strong> time. An alternative approach topredict<strong>in</strong>g pregnancy failure, based on subnormalgrowth of <strong>the</strong> gestational sac and embryo,has been shown to be unreliable. 36Nonvisualization of an embryo with a heartbeatby 6 weeks after <strong>the</strong> last menstrual periodis suspicious <strong>for</strong> failed pregnancy, but dat<strong>in</strong>g of<strong>the</strong> last menstrual period (<strong>in</strong> a pregnancy conceivedwithout medical assistance) is too unreliable<strong>for</strong> def<strong>in</strong>itive diagnosis of pregnancy failure.37 The tim<strong>in</strong>g of events <strong>in</strong> early pregnancy— gestational sac at 5 weeks, yolk sac at 5 1 ∕2weeks, and embryo with heartbeat at 6 weeks— is accurate and reproducible, with a variationof about ± 1 ∕2 week 14,15 ; this consistency expla<strong>in</strong>s<strong>the</strong> time-related criteria <strong>for</strong> pregnancy failurelisted <strong>in</strong> Table 2. For example, if <strong>the</strong> <strong>in</strong>itial ultrasonogramshows a gestational sac with a yolk sacand a follow-up scan obta<strong>in</strong>ed at least 11 dayslater does not show an embryo with cardiac activity,<strong>the</strong> diagnosis of failed pregnancy is established(Fig. 2D and 2E; also see Fig. S3 <strong>in</strong> <strong>the</strong>Supplementary Appendix).O<strong>the</strong>r Suspicious F<strong>in</strong>d<strong>in</strong>gsSeveral ultrasonographic f<strong>in</strong>d<strong>in</strong>gs early <strong>in</strong> <strong>the</strong>first trimester have been reported as abnormal.These <strong>in</strong>clude an “empty” amnion, 38 an enlargedyolk sac, 39 and a small gestational sac. 40 <strong>Criteria</strong><strong>for</strong> <strong>the</strong>se abnormal f<strong>in</strong>d<strong>in</strong>gs are presented <strong>in</strong>Table 2. Because none of <strong>the</strong>se signs have beenextensively studied, <strong>the</strong>y are considered to besuspicious <strong>for</strong>, though not diagnostic of, failedpregnancy.Di agnos<strong>in</strong>g a nd Rul<strong>in</strong>g Ou ta V iable Intr auter <strong>in</strong>e Pr egnancy<strong>in</strong> a Woman with a <strong>Pregnancy</strong>of Unknown LocationThe evaluation and management of a pregnancyof unknown location have received considerableattention, with various flow charts and ma<strong>the</strong>maticalmodels proposed <strong>for</strong> use <strong>in</strong> this context.41,42 Our <strong>in</strong>tent here is not to review <strong>the</strong>broad topic of pregnancy of unknown location,but <strong>in</strong>stead to focus on one important element:<strong>the</strong> role of an hCG level at a s<strong>in</strong>gle po<strong>in</strong>t <strong>in</strong> time<strong>in</strong> diagnos<strong>in</strong>g or rul<strong>in</strong>g out a viable <strong>in</strong>trauter<strong>in</strong>epregnancy and <strong>in</strong> guid<strong>in</strong>g patient-care decisions.The hCG levels <strong>in</strong> viable <strong>in</strong>trauter<strong>in</strong>e pregnancies,nonviable <strong>in</strong>trauter<strong>in</strong>e pregnancies, andectopic pregnancies have considerable overlap,so a s<strong>in</strong>gle hCG measurement does not dist<strong>in</strong>guishreliably among <strong>the</strong>m. 2,4,43 Considerableresearch dur<strong>in</strong>g <strong>the</strong> past 30 years has sought todeterm<strong>in</strong>e <strong>the</strong> discrim<strong>in</strong>atory hCG level: <strong>the</strong>value above which an <strong>in</strong>trauter<strong>in</strong>e gestationalsac is consistently seen on ultra sonography <strong>in</strong>normal pregnancies. An early study, based ontransabdom<strong>in</strong>al ultrasonography, put <strong>the</strong> level at6500 mIU per milliliter. 44 With improvements <strong>in</strong>ultrasonographic technology, <strong>in</strong>clud<strong>in</strong>g <strong>the</strong> <strong>in</strong>troductionof transvag<strong>in</strong>al ultrasonography, gestationalsacs became detectable earlier <strong>in</strong> pregnancy,and <strong>the</strong> reported discrim<strong>in</strong>atory hCGlevel was brought down to 1000 to 2000 mIU permilliliter. 45-47 As with <strong>the</strong> crown–rump lengthand mean sac diameter, however, more recentresearch has shown that previously acceptedvalues <strong>for</strong> <strong>the</strong> discrim<strong>in</strong>atory hCG level are notas reliable <strong>for</strong> rul<strong>in</strong>g out a viable pregnancy asorig<strong>in</strong>ally thought.One reason <strong>for</strong> <strong>the</strong> lower reliability of <strong>the</strong>discrim<strong>in</strong>atory hCG level today than was reported<strong>in</strong> <strong>the</strong> past may be <strong>the</strong> fact that multiplegestations, which are associated with higherhCG levels at a given stage of pregnancy thanare s<strong>in</strong>gleton gestations, are more commonnow than <strong>the</strong>y were 20 to 30 years ago. Failureof <strong>the</strong> discrim<strong>in</strong>atory hCG level to rule out aviable <strong>in</strong>trauter<strong>in</strong>e pregnancy, however, has1448n engl j med 369;15 nejm.org october 10, 2013The New England Journal of Medic<strong>in</strong>eDownloaded from nejm.org on October 10, 2013. For personal use only. No o<strong>the</strong>r uses without permission.Copyright © 2013 Massachusetts Medical Society. All rights reserved.
current conceptsbeen seen <strong>in</strong> s<strong>in</strong>gleton as well as multiple gestations.Several studies have documented cases<strong>in</strong> which an embryo with cardiac activity wasseen on follow-up ultrasonography after <strong>in</strong>itialultrasonography showed no gestational sac withan hCG level above 2000 mIU per milliliter 12,48,49and even above 3000 mIU per milliliter. 12,48In a woman with a pregnancy of unknownlocation whose hCG level is more than 2000 mIUper milliliter, <strong>the</strong> most likely diagnosis is a nonviable<strong>in</strong>trauter<strong>in</strong>e pregnancy, occurr<strong>in</strong>g approximatelytwice as often as ectopic pregnancy. 50Ectopic pregnancy, <strong>in</strong> turn, occurs approximately19 times as often as a viable <strong>in</strong>trauter<strong>in</strong>e pregnancywhen <strong>the</strong> hCG level is 2000 to 3000 mIUper milliliter and <strong>the</strong> uterus is empty, and 70 timesas often as a viable <strong>in</strong>trauter<strong>in</strong>e pregnancy when<strong>the</strong> hCG level is more than 3000 mIU per milliliterwith an empty uterus. (These latter estimatesare based on data from one <strong>in</strong>stitution assess<strong>in</strong>gectopic pregnancies 19 and viable <strong>in</strong>trauter<strong>in</strong>epreg nancies 12 <strong>in</strong> relation to hCG levels <strong>in</strong> womenwith an empty uterus.)On <strong>the</strong> basis of <strong>the</strong>se values, among womenwith a pregnancy of unknown location and hCGlevels of 2000 to 3000 mIU per milli liter, <strong>the</strong>rewill be 19 ectopic pregnancies and 38 nonviable<strong>in</strong>trauter<strong>in</strong>e pregnancies <strong>for</strong> each viable <strong>in</strong>trauter<strong>in</strong>epregnancy. Thus, <strong>the</strong> like lihood of a viable<strong>in</strong>trauter<strong>in</strong>e pregnancy <strong>for</strong> such women is[1 ÷ (1 + 19 + 38)], or approximately 2%. If we use<strong>the</strong> same reason<strong>in</strong>g <strong>for</strong> women with a pregnancyof unknown location and hCG levels ofmore than 3000 mIU per milliliter, <strong>the</strong> likelihoodof a viable <strong>in</strong>trauter<strong>in</strong>e pregnancy is[1 ÷ (1 + 70 + 140)], or approximately 0.5%.We recognize that <strong>the</strong>se estimates of <strong>the</strong> likelihoodof a viable <strong>in</strong>trauter<strong>in</strong>e pregnancy <strong>in</strong> awoman with a pregnancy of unknown locationwhose hCG level is 2000 mIU per milliliter orhigher are not highly precise, given <strong>the</strong> limitationsof <strong>the</strong> available data, but <strong>the</strong>re are a numberof reasons why presumptive treatment <strong>for</strong> ectopicpregnancy with <strong>the</strong> use of methotrexate or o<strong>the</strong>rpharmacologic or surgical means is <strong>in</strong>appropriateif <strong>the</strong> woman is hemodynamically stable.<strong>First</strong>, as noted above, <strong>the</strong>re is a chance of harm<strong>in</strong>ga viable <strong>in</strong>trauter<strong>in</strong>e pregnancy, especially if<strong>the</strong> hCG level is 2000 to 3000 mIU per milliliter.Second, <strong>the</strong> most likely diagnosis is nonviable<strong>in</strong>trauter<strong>in</strong>e pregnancy (i.e., failed pregnancy), 50and methotrexate is not an appropriate treatment<strong>for</strong> a woman with this diagnosis. Third, <strong>the</strong>re islimited risk <strong>in</strong> tak<strong>in</strong>g a few extra days to make adef<strong>in</strong>itive diagnosis <strong>in</strong> a woman with a pregnancyof unknown location who has no signs orsymptoms of rupture and no ultrasonographicevidence of ectopic pregnancy. Fourth, <strong>the</strong> progressionof hCG values over a period of 48 hoursprovides valuable <strong>in</strong><strong>for</strong>mation <strong>for</strong> diagnostic and<strong>the</strong>rapeutic decision mak<strong>in</strong>g. 4,51 Thus, it is generallyappropriate to do additional test<strong>in</strong>g be<strong>for</strong>eundertak<strong>in</strong>g treatment <strong>for</strong> ectopic pregnancy <strong>in</strong> ahemodynamically stable patient (Table 3). 2,43,52Table 3. <strong>Diagnostic</strong> and Management Guidel<strong>in</strong>es Related to <strong>the</strong> Possibility of a Viable Intrauter<strong>in</strong>e <strong>Pregnancy</strong><strong>in</strong> a Woman with a <strong>Pregnancy</strong> of Unknown Location.*F<strong>in</strong>d<strong>in</strong>gNo <strong>in</strong>trauter<strong>in</strong>e fluid collectionand normal (or near-normal)adnexa on ultrasonography†Ultrasonography not yetper<strong>for</strong>medKey Po<strong>in</strong>tsA s<strong>in</strong>gle measurement of hCG, regardless of its value, does not reliably dist<strong>in</strong>guishbetween ectopic and <strong>in</strong>trauter<strong>in</strong>e pregnancy (viable or nonviable).If a s<strong>in</strong>gle hCG measurement is
T h e n e w e ngl a nd j o u r na l o f m e dic i n eWomen with ectopic pregnancies have highlyvariable hCG levels, often less than 1000 mIUper milliliter, 43,53,54 and <strong>the</strong> hCG level does notpredict <strong>the</strong> likelihood of ectopic pregnancy rupture.55 That is, a s<strong>in</strong>gle hCG value, even if low,does not rule out a potentially life-threaten<strong>in</strong>gruptured ectopic pregnancy. Hence, ultrasonographyis <strong>in</strong>dicated <strong>in</strong> any woman with a positivepregnancy test who is cl<strong>in</strong>ically suspected ofhav<strong>in</strong>g an ectopic pregnancy.ConclusionsA false positive diagnosis of nonviable pregnancyearly <strong>in</strong> <strong>the</strong> first trimester — <strong>in</strong>correctly diagnos<strong>in</strong>gpregnancy failure <strong>in</strong> a woman with an <strong>in</strong>trauter<strong>in</strong>egestational sac or rul<strong>in</strong>g out viable <strong>in</strong>trauter<strong>in</strong>egestation <strong>in</strong> a woman with a pregnancy of unknownlocation — can prompt <strong>in</strong>terventions thatdamage a pregnancy that might have had a normaloutcome. Recent research has shown <strong>the</strong> needto adopt more str<strong>in</strong>gent criteria <strong>for</strong> <strong>the</strong> diagnosisof nonviability <strong>in</strong> order to m<strong>in</strong>imize or avoid falsepositive test results. The guidel<strong>in</strong>es presented here,if promulgated widely to practitioners <strong>in</strong> <strong>the</strong> variousspecialties <strong>in</strong>volved <strong>in</strong> <strong>the</strong> diagnosis and managementof problems <strong>in</strong> early pregnancy, wouldimprove patient care and reduce <strong>the</strong> risk of <strong>in</strong>advertentharm to potentially normal pregnancies.Supported by fund<strong>in</strong>g from <strong>the</strong> National Institute <strong>for</strong> HealthResearch Biomedical Research Centre based at Imperial CollegeHealthcare National Health Service Trust and Imperial CollegeLondon (to Dr. Bourne).Dr. Benacerraf reports receiv<strong>in</strong>g lecture fees from World ClassCME and <strong>the</strong> International Institute <strong>for</strong> Cont<strong>in</strong>u<strong>in</strong>g Medical Educationand travel reimbursement from GE Healthcare. Dr. Bensonreports receiv<strong>in</strong>g fees <strong>for</strong> expert testimony <strong>in</strong> medical malpracticecases regard<strong>in</strong>g standard of care <strong>for</strong> <strong>in</strong>terpretation of ultrasonographicexam<strong>in</strong>ations and lecture fees from <strong>the</strong> International Institute<strong>for</strong> Cont<strong>in</strong>u<strong>in</strong>g Medical Education and <strong>the</strong> Institute <strong>for</strong>Advanced Medical Education. Dr. Doubilet reports receiv<strong>in</strong>g fees<strong>for</strong> expert testimony <strong>in</strong> medical malpractice cases regard<strong>in</strong>g standardof care <strong>for</strong> <strong>in</strong>terpretation of ultrasonographic exam<strong>in</strong>ationsand lecture fees from <strong>the</strong> International Institute <strong>for</strong> Cont<strong>in</strong>u<strong>in</strong>gMedical Education. Dr. Filly reports receiv<strong>in</strong>g fees <strong>for</strong> expert testimony<strong>in</strong> medical malpractice cases as an expert <strong>in</strong> diagnostic sonographyand lecture fees from World Class CME. He also reportsbe<strong>in</strong>g co-holder of a patent <strong>for</strong> a needle-guide device used <strong>for</strong>venous access under ultrasonographic guidance. Dr. Goldste<strong>in</strong>reports receiv<strong>in</strong>g consult<strong>in</strong>g fees from Cook OB/GYN, Pfizer,Shionogi, and Bayer and lecture fees from Merck and WarnerChilcott. Dr. Lyons reports receiv<strong>in</strong>g lecture fees from GE MedicalSystems and hold<strong>in</strong>g stock <strong>in</strong> Zonare Medical Systems. No o<strong>the</strong>rpotential conflict of <strong>in</strong>terest relevant to this article was reported.Disclosure <strong>for</strong>ms provided by <strong>the</strong> authors are available with<strong>the</strong> full text of this article at NEJM.org.References1. Creanga AA, Shapiro-Mendoza CK,Bish CL, Zane S, Berg CJ, Callaghan WM.Trends <strong>in</strong> ectopic pregnancy mortality <strong>in</strong><strong>the</strong> United States, 1980-2007. Obstet Gynecol2011;117:837-43.2. Barnhart KT. Ectopic pregnancy.N Engl J Med 2009;361:379-87.3. Doubilet PM, Benson CB. <strong>First</strong>, do noharm . . . to early pregnancies. J UltrasoundMed 2010;29:685-9.4. Barnhart KT. <strong>Early</strong> pregnancy failure:beware of <strong>the</strong> pitfalls of modern management.Fertil Steril 2012;98:1061-5.5. Nurmohamed L, Moretti ME, SchechterT, et al. Outcome follow<strong>in</strong>g high-dosemethotrexate <strong>in</strong> pregnancies misdiagnosedas ectopic. Am J Obstet Gynecol 2011;205(6):533.e1-533.e3.6. Shwayder JM. Wait<strong>in</strong>g <strong>for</strong> <strong>the</strong> tide tochange: reduc<strong>in</strong>g risk <strong>in</strong> <strong>the</strong> turbulent seaof liability. Obstet Gynecol 2010;116:8-15.7. Misdiagnosed ectopic, given methotrexate.Facebook website (http://www.facebook.com/groups/misduagnosedectopic/).8. Doubilet P. A ma<strong>the</strong>matical approachto <strong>in</strong>terpretation and selection of diagnostictests. Med Decis Mak<strong>in</strong>g 1983;3:177-95.9. Jeve Y, Rana R, Bhide A, Thangarat<strong>in</strong>amS. Accuracy of first trimester ultrasound<strong>in</strong> <strong>the</strong> diagnosis of early embryonicdemise: a systematic review. UltrasoundObstet Gynecol 2011;38:489-96.10. Abdallah Y, Daemen A, Kirk E, et al.Limitations of current def<strong>in</strong>itions of miscarriageus<strong>in</strong>g mean gestational sac diameterand crown–rump length measurements:a multicenter observational study. UltrasoundObstet Gynecol 2011;38:497-502.11. Hamilton J, Hamilton J. The 6 mmcrown–rump length threshold <strong>for</strong> detect<strong>in</strong>gfetal heart movements — what is <strong>the</strong>evidence? Ultrasound Obstet Gynecol 2011;38:Suppl 1:7. abstract.12. Doubilet PM, Benson CB. Fur<strong>the</strong>r evidenceaga<strong>in</strong>st <strong>the</strong> reliability of <strong>the</strong> humanchorionic gonadotrop<strong>in</strong> discrim<strong>in</strong>atorylevel. J Ultrasound Med 2011;30:1637-42.13. Thilaganathan B. The evidence base<strong>for</strong> miscarriage diagnosis: better late thannever. Ultrasound Obstet Gynecol 2011;38:487-8.14. Bree RL, Edwards M, Böhm-Velez M,Beyler S, Roberts J, Mendelson EB. Transvag<strong>in</strong>alsonography <strong>in</strong> <strong>the</strong> evaluation ofnormal early pregnancy: correlation withhCG level. AJR Am J Roentgenol 1989;153:75-9.15. Goldste<strong>in</strong> I, Zimmer EA, Tamir A,Peretz BA, Paldi E. Evaluation of normalgestational sac growth: appearance ofembryonic heartbeat and embryo bodymovements us<strong>in</strong>g <strong>the</strong> transvag<strong>in</strong>al technique.Obstet Gynecol 1991;77:885-8.16. Bradley WG, Fiske CE, Filly RA. Thedouble sac sign of early <strong>in</strong>trauter<strong>in</strong>e pregnancy:use <strong>in</strong> exclusion of ectopic pregnancy.Radiology 1982;143:223-6.17. Yeh H-C, Goodman JD, Carr L, Rab<strong>in</strong>owitzJG. Intradecidual sign: a US criterionof early <strong>in</strong>trauter<strong>in</strong>e pregnancy. Radiology1986;161:463-7.18. Doubilet PM, Benson CB. Double sacsign and <strong>in</strong>tradecidual sign <strong>in</strong> early pregnancy:<strong>in</strong>terobserver reliability and frequencyof occurrence. J Ultrasound Med2013;32:1207-14.19. Benson CB, Doubilet PM, Peters HE,Frates MC. Intrauter<strong>in</strong>e fluid with ectopicpregnancy: a reappraisal. J Ultrasound Med2013;32:389-93.20. Barnhart K, van Mello NM, Bourne T,et al. <strong>Pregnancy</strong> of unknown location: aconsensus statement of nomenclature,def<strong>in</strong>itions, and outcome. Fertil Steril 2011;95:857-66.21. Mueller CE. Intrauter<strong>in</strong>e pseudogestationalsac <strong>in</strong> ectopic pregnancy. J Cl<strong>in</strong>Ultra sound 1979;7:133-6.22. Ackerman TE, Levi CS, Lyons EA,Dashefsky SM, L<strong>in</strong>dsay DJ, Holt SC. Decidualcyst: endovag<strong>in</strong>al sonographic signof ectopic pregnancy. Radiology 1993;189:727-31.23. Levi CS, Lyons EA, Zheng XH, L<strong>in</strong>dsayDJ, Holt SC. Endovag<strong>in</strong>al ultrasound: demonstrationof cardiac activity <strong>in</strong> embryos ofless than 5.0 mm <strong>in</strong> crown-rump length.Radiology 1990;176:71-4.1450n engl j med 369;15 nejm.org october 10, 2013The New England Journal of Medic<strong>in</strong>eDownloaded from nejm.org on October 10, 2013. For personal use only. No o<strong>the</strong>r uses without permission.Copyright © 2013 Massachusetts Medical Society. All rights reserved.