Food Allergy Care Plan - Louisburg USD 416
Food Allergy Care Plan - Louisburg USD 416
Food Allergy Care Plan - Louisburg USD 416

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
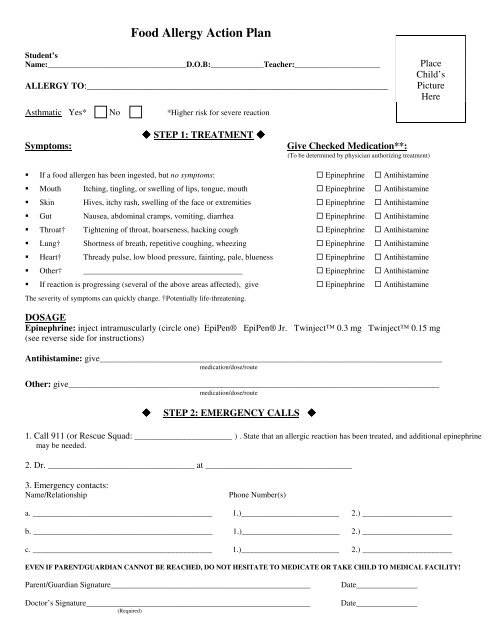
<strong>Food</strong> <strong>Allergy</strong> Action <strong>Plan</strong>Student’sName:__________________________________D.O.B:_____________Teacher:_____________________ALLERGY TO:______________________________________________________________Asthmatic Yes* No *Higher risk for severe reactionPlaceChild’sPictureHere STEP 1: TREATMENT Symptoms: Give Checked Medication**: If a food allergen has been ingested, but no symptoms: Epinephrine Antihistamine Mouth Itching, tingling, or swelling of lips, tongue, mouth Epinephrine Antihistamine Skin Hives, itchy rash, swelling of the face or extremities Epinephrine Antihistamine Gut Nausea, abdominal cramps, vomiting, diarrhea Epinephrine Antihistamine Throat† Tightening of throat, hoarseness, hacking cough Epinephrine Antihistamine Lung† Shortness of breath, repetitive coughing, wheezing Epinephrine Antihistamine Heart† Thready pulse, low blood pressure, fainting, pale, blueness Epinephrine Antihistamine Other† _______________________________________ Epinephrine Antihistamine If reaction is progressing (several of the above areas affected), give Epinephrine AntihistamineThe severity of symptoms can quickly change. †Potentially life-threatening.DOSAGEEpinephrine: inject intramuscularly (circle one) EpiPen® EpiPen® Jr. Twinject 0.3 mg Twinject 0.15 mg(see reverse side for instructions)Antihistamine: give____________________________________________________________________________________medication/dose/routeOther: give___________________________________________________________________________________________medication/dose/route STEP 2: EMERGENCY CALLS 1. Call 911 (or Rescue Squad: ________________________ ) . State that an allergic reaction has been treated, and additional epinephrinemay be needed.2. Dr. ____________________________________ at ____________________________________(To be determined by physician authorizing treatment)3. Emergency contacts:Name/RelationshipPhone Number(s)a. ____________________________________________ 1.)________________________ 2.) ______________________b. ____________________________________________ 1.)________________________ 2.) ______________________c. ____________________________________________ 1.)________________________ 2.) ______________________EVEN IF PARENT/GUARDIAN CANNOT BE REACHED, DO NOT HESITATE TO MEDICATE OR TAKE CHILD TO MEDICAL FACILITY!Parent/Guardian Signature_________________________________________________Doctor’s Signature_______________________________________________________(Required)Date_______________Date_______________
TRAINED STAFF MEMBERS1. ____________________________________________________ Room ________2. ____________________________________________________ Room ________3. ____________________________________________________ Room ________EpiPen® and EpiPen® Jr. Directions Pull off gray activation cap.Twinject 0.3 mg and Twinject 0.15 mgDirections Hold black tip near outer thigh(always apply to thigh). Pull off green end cap, then red end cap. Put gray cap against outerthigh, press down firmlyuntil needle penetrates. Holdfor 10 seconds, then remove. Swing and jab firmly into outer thighuntil Auto-Injector mechanismfunctions. Hold in place and countto 10. Remove the EpiPen® unit andmassage the injection area for 10seconds.SECOND DOSE ADMINISTRATION:If symptoms don’t improve after10 minutes, administer second dose: Unscrew gray cap and pullsyringe from barrel by holdingblue collar at needle base. Slide yellow or orangecollar off plunger. Put needle into thigh throughskin, push plunger downall the way, and remove.Once EpiPen® or Twinject is used, call the Rescue Squad. Take the used unit with you to theEmergency Room. <strong>Plan</strong> to stay for observation at the Emergency Room for at least 4 hours.For children with multiple food allergies, consider providing separate Action<strong>Plan</strong>s for different foods.**Medication checklist adapted from the Authorization of Emergency Treatment formdeveloped by the Mount Sinai School of Medicine. Used with permission.
PERMISSION TO CARRY ASTHMA INHALERS/EPIPENSTO BE COMPLETED BY THE PHYSICIAN: The above‐named student has been instructed in the proper use of their asthmainhaler/emergency medication. The child’s well‐being is in jeopardy unless this medication is carried on his/her person. Therefore, Irequest that he/she be permitted to carry the asthma inhaler/emergency medication at school. He/she understands the purpose,appropriate method, and frequency of use of the asthma inhaler/emergency medication.NAME OF MEDICATION: ______________________ PHYSICIAN’S SIGNATURE: _____________________ DATE: _________TO BE COMPLETED BY THE PARENT/GUARDIAN: I permit my child to carry the above‐listed asthma inhaler/emergency medicationas ordered by his/her physician.PARENT/GUARDIAN SIGNATURE: __________________________________________ DATE: ________________TO BE COMPLETED BY SCHOOL NURSE: Kansas law now permits students to carry and use inhaled medications after demonstratingappropriate use to school nurse. This student demonstrates knowledge / skill to carry and use the above listed asthma inhaler.SCHOOL NURSE SIGNATURE: ______________________________________________ DATE: ________________TO BE COMPLETED BY STUDENT: I have been instructed in the proper use of my medication and will take it as prescribed to me bymy physician.STUDENT’S SIGNATURE: _________________________________________________ DATE: _________________KS approval 07/15/09