PRESENTATION on BEST PRACTICES for VASCULAR ACCESS
VASCULAR ACCESS BEST PRACTICES - Network 6
VASCULAR ACCESS BEST PRACTICES - Network 6

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>PRESENTATION</str<strong>on</strong>g> <strong>on</strong> <strong>BEST</strong> <strong>PRACTICES</strong><strong>for</strong><strong>VASCULAR</strong> <strong>ACCESS</strong>The presentati<strong>on</strong> will start at 10:00 amRoll call will not be takenYour participati<strong>on</strong> will be verified by a post survey atthe end of the presentati<strong>on</strong>All lines MUST be muted throughout the presentati<strong>on</strong>(*6) MutesAt the end of the presentati<strong>on</strong> Questi<strong>on</strong>s will betaken, at that time all lines MUST be un-muted(*6) Un-Mutes1
SPREADING <strong>PRACTICES</strong>INNETWORK6By: Cyndy McCallus RN, BSNNetwork 6 Quality Improvement Nurse SpecialistOctober, 20122
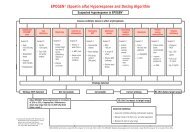
<strong>VASCULAR</strong> <strong>ACCESS</strong> <strong>BEST</strong> <strong>PRACTICES</strong>OBJECTIVESAt the end of this webinar attendees will be ableto:• Understand the “CMS goal” <strong>for</strong> AV Fistulas• Discuss the importance of “AV Fistulas”• Review Best Practices used by your facilities• Verbalize the benefit of sharing/Utilizing “BestPractices”• Initiate a new process or add to a current process toimprove Vascular Access outcomes‐ “Sustain Gain”3
WHY is it IMPORTANTCenters <strong>for</strong> Medicare & Medicaid (CMS)implemented a high priority goal of 66% AV FistulaRate across the nati<strong>on</strong>…WHY?CMS recognizes a well functi<strong>on</strong>ing vascular accessenables the hemo‐dialysis patient to receiveefficient/adequate dialysis treatments, enhancing theirquality of life; V550(5).4
The FFBI c<strong>on</strong>sists of the Centers of Medicare & MedicaidServices (CMS), ESRD Networks, and the entire renalcommunity, work together to ensure that every suitablepatient will receive the most optimal <strong>for</strong>m of vascular access –which, most cases, will be a native AV fistula.Fistulas are the “Gold Standard” <strong>for</strong> establishing access to apatient’s circulatory system in order to provide life sustainingdialysis(CMS Administrator Mark B McClellan, MD, PHD)5
KDOQIKDOQI(Nati<strong>on</strong>al Kidney Foundati<strong>on</strong> Disease Outcomes Quality Initiative)Vascular access c<strong>on</strong>tinues to be a leading cause <strong>for</strong>hospitalizati<strong>on</strong> and morbidity in patients with CKDstage 5. Appropriate care of HD patients with CKDstage 5 requires c<strong>on</strong>stant attenti<strong>on</strong> to the maintenanceof vascular access patency and functi<strong>on</strong>Studies c<strong>on</strong>sistently indicate that the AV Fistulahas the best patency rates and require fewerinterventi<strong>on</strong>s in comparis<strong>on</strong> to other access typesGOALS: Increase the placement of native fistulaeDetect access dysfuncti<strong>on</strong> be<strong>for</strong>e access thrombosis6
GOAL66%7
Many say that 66% is UNREALISTICThat is a MYTH1) Other than the USA and Canada, everycountry in DOPPS (Europe, Japan, Aus, NZ) has aprevalent AVF rate >66%2)The NKF/KDOQI vascular accessworkgroup examined the evidence and supports thisgoal3) There are two Networks that havereached that goal in the USA, so it can be DONE8
AVF Rates by Network80.0%70.0%60.0%% Prevalent AVF by NetworkMarch 2011 compared to March 2012% AVF50.0%40.0%30.0%20.0%10.0%0.0%6 8 9 5 11 3 10 13 7 4 14 US 12 2 17 1 18 15 16March 2011 Rate 52.8 55.3 54.2 55.1 56.1 57.3 57.2 57.0 57.9 57.1 58.0 58.0 58.0 60.2 61.6 61.9 61.6 64.7 66.3March 2012 Rate 56.0 57.8 57.8 58.0 58.9 59.0 59.2 59.3 59.7 59.9 60.1 60.4 60.7 62.5 62.9 63.8 63.9 67.0 68.5Increase 3.2% 2.5% 3.6% 2.9% 2.8% 1.7% 2.0% 2.3% 1.8% 2.8% 2.1% 2.4% 2.7% 2.3% 1.3% 1.9% 2.3% 2.3% 2.2%
Catheters are associated with:Increased infecti<strong>on</strong>sIncreased hospitalizati<strong>on</strong>sIncreased deathsAV Grafts associated with:More complicati<strong>on</strong>s (8x’s > risk) – American Society of NephrologyDecreased survival of accessIncreased interventi<strong>on</strong>sHigher CostsTotal Care Costs:CVC - $79,364AVG - $72,729AVF - $58,588Source: USRDS Data Report ‐ Costs of ESRD
WHAT TO DO?BestPractices11
DEFINE <strong>BEST</strong> <strong>PRACTICES</strong>Methods and techniques that havec<strong>on</strong>sistently shown results superior thanthose achieved with other means, andwhich are used as benchmarks to strive <strong>for</strong>.12
<strong>BEST</strong> <strong>PRACTICES</strong>No practice is best <strong>for</strong> every<strong>on</strong>e or inevery situati<strong>on</strong>, and no best practiceremains best <strong>for</strong> very l<strong>on</strong>g as peoplekeep <strong>on</strong> finding better ways ofdoing things.13
<strong>VASCULAR</strong> <strong>ACCESS</strong> is NOT ONE SIZE FITS ALL14
Best Practices TO FOLLOWVein mapping, timely referral, Access CenterMaintain the access <strong>on</strong>ce established/AVF friendlysurge<strong>on</strong>C<strong>on</strong>tinuous Quality Improvement/Tracking/SleevesupVascular access Coordinator, M<strong>on</strong>itoring andMaintenance15
Preserve future sites <strong>for</strong> vascular access/vesselpreservati<strong>on</strong>/PICC/Epicardial FirstProvide educati<strong>on</strong> to patients, family, and staff,modified hospital systemsShare successes and failures/multi-disciplinarymeetingsCannulati<strong>on</strong> techniques, self management,butt<strong>on</strong>hole16
DIALYSIS AVF FEUD17
22.2% 26.3%Network 6• Increased Medical Director/Nephrologist/CorporateInvolvement•Increased Patient Educati<strong>on</strong>•Vessel Mapping•Change in referral patterns•Dedicated Vascular Access Coordinator19
39.4% 53.6%Network 6•Dedicated Vascular Access Coordinator•Utilizati<strong>on</strong> of Vascular Access Center•Referring to different Surge<strong>on</strong>s•Vascular access tracking/trending20
34.3 %Network 650.6%• Increased Surge<strong>on</strong> Involvement• Reassessment of all AVG patients• Increased Patient Educati<strong>on</strong>• Vessel Mapping• Increased CKD Educati<strong>on</strong>/Early Referral21
46.9 % 59.4%Network 6• Vascular Access Tracking/Trending• Utilizati<strong>on</strong> of Vascular Access Centers• Increased Patient Educati<strong>on</strong>• AVF placement in patients with catheterswhen indicated (regardless of prior access)22
36.8% 44.6%Network 6• Designated Staff Member as Access Coordinator• Increased Medical Director/Nephrologist/CorporateInvolvement• Vascular Access tracking/trending• Increased Cannulati<strong>on</strong> Training23
29.2% 55.7%Network 6•Educati<strong>on</strong>al Learning Sessi<strong>on</strong>s focusing <strong>on</strong>topic with pre and post test to assessknowledge•Celebrati<strong>on</strong>s of access placement•Surge<strong>on</strong> and/or interventi<strong>on</strong>al team presentingto staff <strong>on</strong> cannulati<strong>on</strong>•Butt<strong>on</strong>hole technique educati<strong>on</strong>•Reiterati<strong>on</strong> of the CVC placement24
37.5% 53.0%Network 6•Dedicated Vascular Access Coordinator•Utilizati<strong>on</strong> of Vascular Access Center•Trending Vascular Surge<strong>on</strong> results•Referral to “Fistula Friendly” VascularSurge<strong>on</strong>s <strong>on</strong>ly25
SPREAD SOLUTIONS/OUTCOMESSHARE RESOURCES, STATISTICS, IDEAS, THOUGHTS26
Why Spread Ideas?•Enhancement of effectiveness and efficiency by spreadinggood ideas and practices•Time savings –Learn from others mistakes•B<strong>on</strong>ds c<strong>on</strong>necti<strong>on</strong> – strengthens problem solvingtechniques•More sophisticated ideas, insights, results in bettersoluti<strong>on</strong>s•Provides innovati<strong>on</strong> and discovery, increases engagement,motivati<strong>on</strong>•Satisfacti<strong>on</strong> from sharing knowledge•Benefits the facility, patient and family27
•Follow up with Vascular Surge<strong>on</strong> <strong>for</strong> start date ofcannulati<strong>on</strong>•Medical Director to meet with local surge<strong>on</strong>s. Also,scheduled vein mapping prior to hospital discharge•Frequent Review•Referring New Patients <strong>for</strong> access placement with in thefirst 2 treatments and referring to the “Right Surge<strong>on</strong>” isthe best way to get the patient <strong>on</strong> board and to get AVFinstead of AVG 28
•Butt<strong>on</strong>hole cannulati<strong>on</strong> program•Vascular Coordinator and Nephrology Nurse Practi<strong>on</strong>erfull time at hospital resp<strong>on</strong>sible <strong>for</strong> CKD educati<strong>on</strong>, timelyreferral to Vascular surge<strong>on</strong>•Vessel mapping and access placement prior to admissi<strong>on</strong>to facility•M<strong>on</strong>thly Access reporting and c<strong>on</strong>ference calls withVascular Team29
Road Blocks to Best PracticesSystem• Pt.’s without Medical Insurance• Waiting time <strong>for</strong> Insurancecoverage• N<strong>on</strong> Cooperative Surge<strong>on</strong>s/NotAVF friendly• Communicati<strong>on</strong> betweenSurge<strong>on</strong>/Hospital/Access Center• Lack of Knowledge of AttendingMD• AVF not Maturing, Late referral• Discharged with no AVF plan/veinmappingPatient• Fear of Needles• Exhausted sites• Lack of Knowledge• Refusing• Catheter Culture• N<strong>on</strong>‐compliant• Language Barriers• Transportati<strong>on</strong>• Co‐Morbidities/Age30
POSSIBLE SOLUTIONSSystem• Establish relati<strong>on</strong>ship withInsurance c<strong>on</strong>tacts• Collaborate with Surge<strong>on</strong>soffice• Work with local primary carepractiti<strong>on</strong>ers and hospitals• Training <strong>for</strong> Surge<strong>on</strong>Nephrologist/Medical Director• Early referral <strong>for</strong> AVF, veinmapping, utilize tracking tools,algorithms• Meet with hospital dischargeteamPatient• Patient, family educati<strong>on</strong> beinventive in delivery• Follow up with patients thatrefuse• Terminology with catheters –Permanent vs. Temporarymaybe use Cuffed/n<strong>on</strong>‐Cuffed• AMA <strong>for</strong>ms –document, careplan meetings, involve family• Utilize SW to help withtransportati<strong>on</strong>, languagebarriers31
SUSTAIN your GAINSustainability: Locking in the progress that you havemade already and c<strong>on</strong>tinually building up<strong>on</strong> it:ANDSpread: Actively disseminating <strong>BEST</strong> PRACTICE andknowledge about every interventi<strong>on</strong> andimplementing each interventi<strong>on</strong> in every availablesetting32
Improving AVF Rates• Follow your Comprehensive Acti<strong>on</strong> Plan• Address the Problem• Have Goals• Root Causes/Barriers• Interventi<strong>on</strong>s• Resp<strong>on</strong>sible parties• Regular Updates/QAPI meetings• Documentati<strong>on</strong>• New Ideas/Thoughts/Implement/SHARE/SPREAD33
Network 6Missi<strong>on</strong>Improve the livesof People with orat risk of ESRDby promotingand AdvancingQuality of Care34
RESOURCES• www.myskc.org• http://www.fistulafirst.org/• www.kidney.org35
QUESTIONSIf you have any questi<strong>on</strong>s please c<strong>on</strong>tactCyndy McCallus RN, BSNDebra Evans RN, BSNatinfo@nw6.esrd.netComplete Participati<strong>on</strong> Survey:http://www.surveym<strong>on</strong>key.com/s/BestPract36