

CHANGE
baghc_f
baghc_f

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ARTICLE OF<br />
INTEREST<br />
ARTICLE OF<br />
INTEREST<br />
THE POLITICS OF OBESITY<br />
Obesity is a complex illness and social issue and is increasingly prevalent<br />
GEORGE HOPKINS<br />
Obesity Surgery Society of Australia<br />
& New Zealand, President<br />
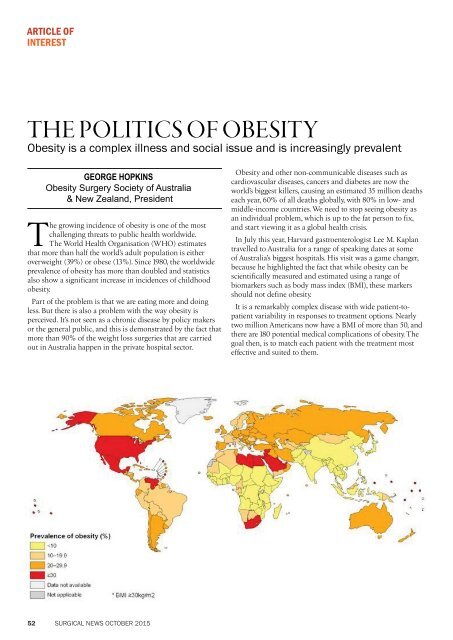
The growing incidence of obesity is one of the most<br />
challenging threats to public health worldwide.<br />
The World Health Organisation (WHO) estimates<br />
that more than half the world’s adult population is either<br />
overweight (39%) or obese (13%). Since 1980, the worldwide<br />
prevalence of obesity has more than doubled and statistics<br />
also show a significant increase in incidences of childhood<br />
obesity.<br />
Part of the problem is that we are eating more and doing<br />
less. But there is also a problem with the way obesity is<br />
perceived. It’s not seen as a chronic disease by policy makers<br />
or the general public, and this is demonstrated by the fact that<br />
more than 90% of the weight loss surgeries that are carried<br />
out in Australia happen in the private hospital sector.<br />
Obesity and other non-communicable diseases such as<br />
cardiovascular diseases, cancers and diabetes are now the<br />
world’s biggest killers, causing an estimated 35 million deaths<br />
each year, 60% of all deaths globally, with 80% in low- and<br />
middle-income countries. We need to stop seeing obesity as<br />
an individual problem, which is up to the fat person to fix,<br />
and start viewing it as a global health crisis.<br />
In July this year, Harvard gastroenterologist Lee M. Kaplan<br />
travelled to Australia for a range of speaking dates at some<br />
of Australia’s biggest hospitals. His visit was a game changer,<br />
because he highlighted the fact that while obesity can be<br />
scientifically measured and estimated using a range of<br />
biomarkers such as body mass index (BMI), these markers<br />
should not define obesity.<br />
It is a remarkably complex disease with wide patient-topatient<br />
variability in responses to treatment options. Nearly<br />
two million Americans now have a BMI of more than 50, and<br />
there are 180 potential medical complications of obesity. The<br />
goal then, is to match each patient with the treatment most<br />
effective and suited to them.<br />
The complexity of obesity<br />
Obese patients who require surgery that is not weight loss<br />
related should still be encouraged to reduce their weight<br />
before surgery, especially if they have features of metabolic<br />
syndrome. Prescribed low calorie diets can help achieve<br />
preoperative weight loss.<br />
A combination of preventative measures and an increase in<br />
the availability of treatment options for those who are already<br />
obese will help curb this disease. Examples of preventative<br />
measures include better labelling on food packaging and<br />
public education programs. There is evidence to suggest that<br />
education programs can have a positive impact on physical<br />
activity levels.<br />
Where preventative measures have failed, there is strong<br />
evidence to suggest that surgery is an effective intervention for<br />
weight loss in the morbidly obese (BMI > 40), and that this<br />
may reduce the long-term costs and health impacts of obesity.<br />
Dr Kaplan points out that gastric bypass has the opposite<br />
effect to restrictive dieting, with energy expenditure and<br />
satiety going up, and appetite and stress response decreasing.<br />
Providing access for weight loss surgery in public hospitals<br />
seems a difficult commitment for policy makers. In the face of<br />
overwhelming science this can be interpreted as a bias against<br />
the obese, as it is so often viewed rightly or wrongly as selfinflicted.<br />
The other consideration is the overwhelming numbers<br />
that could and would stand ready for surgical treatment<br />
whenever and wherever this service is offered. Our<br />
experience at the Royal Brisbane & Women’s Hospital<br />
certainly suggests that to manage the workloads and wait<br />
times, very strict parameters need to be applied to eligibility<br />
for surgical intervention. That said our clinics remain<br />
saturated and intermittently closed to new case referrals.<br />
Access Economics estimates that the number of obese<br />
people in Australia is set to double by 2028 to almost 8<br />
million. The medical, psychological and financial burden of<br />
obesity, coupled with the failure of conservative measures<br />
and the success of surgical interventions, is why weight<br />
loss surgery must be considered part of the package in<br />
addressing the obesity epidemic.<br />
With Amy Kimber<br />
52 SURGICAL NEWS OCTOBER 2015 SURGICAL NEWS OCTOBER 2015 53