

Official Journal Of The Trinidad & Tobago Medical - the Trinidad and ...
Official Journal Of The Trinidad & Tobago Medical - the Trinidad and ...
Official Journal Of The Trinidad & Tobago Medical - the Trinidad and ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Caribbean <strong>Medical</strong> <strong>Journal</strong><br />
Development of a Nationwide T&T Diabetes Outreach Program<br />
Part 2: Specific Programs<br />
Immediately after a patient has anthropometrics entered <strong>and</strong><br />
POC testing performed, <strong>the</strong> data, collected <strong>and</strong> now stored in<br />
TTDEMS, is printed out onto a “Stoplight Form” by a color<br />
printer; one copy is given to <strong>the</strong> healthcare provider, <strong>and</strong> ano<strong>the</strong>r<br />
copy is given to <strong>the</strong> patient. <strong>The</strong> purpose of this form is twofold-<br />
- to provide POC results for <strong>the</strong> healthcare provider to act upon<br />
during <strong>the</strong> clinic visit that same day, <strong>and</strong> to alert patients to <strong>the</strong>ir<br />
level of control for each parameter. Ten parameters indicated<br />
on each Stoplight Form: body mass index, blood pressure,<br />
HbA1c, glucose, urinary microalbumin:creatinine ratio, total<br />
cholesterol, triglycerides, LDL cholesterol, HDL cholesterol<br />
<strong>and</strong> foot exam. <strong>The</strong> TTDEMS system flags individual patient<br />
results with a red light, yellow light, or green light, based on<br />
ranges consistent with those recommended by CHRC, PAHO,<br />
<strong>and</strong> <strong>the</strong> American Diabetes Association. A red light indicates<br />
“poor; take action”; a yellow light indicates “needs improvement”;<br />
<strong>and</strong> a green light indicates “good”. <strong>The</strong> reverse side of <strong>the</strong><br />
Stoplight Form contains suggestions for providers on diabetes<br />
care pathway guidelines. See attached sample of a Stoplight<br />
Form given to a patient who participated in our Diabetes Outreach<br />
Program (Figure 1 of Stoplight Form).<br />
TTDEMS not only prints out immediate results on <strong>the</strong> individual<br />
patient, but can aggregate data. <strong>The</strong> aggregate group data stored<br />
in <strong>the</strong> TTDEMS database can be used for a variety of purposes:<br />
To assess prevalent risk status (such as HbA1c, dyslipidemia,<br />
<strong>and</strong> hypertension); to assess prevalent complication status (such<br />
as microalbuminuria); <strong>and</strong> to assess <strong>the</strong> prevalence of provider<br />
adherence to CHRC/PAHO guidelines for management of<br />
diabetes.<br />
A number of health care research questions could be evaluated<br />
using aggregate data, such as: What is <strong>the</strong> status of diabetes<br />
care in each clinic? What characteristics affect <strong>the</strong> health status<br />
observed – access to or utilization of services? Medications<br />
prescribed? Medications taken? Does POC testing improve a<br />
clinic’s achievement of guideline adherence (such as regularity<br />
of HbA1c, lipid, or microalbumin testing), <strong>and</strong> does it change<br />
provider adherence to established guidelines? Studies have<br />
suggested that having access to immediate test results through<br />
POC testing is associated with <strong>the</strong> same or better medication<br />
adherence compared with having test results provided by a<br />
pathology laboratory 6 .<br />
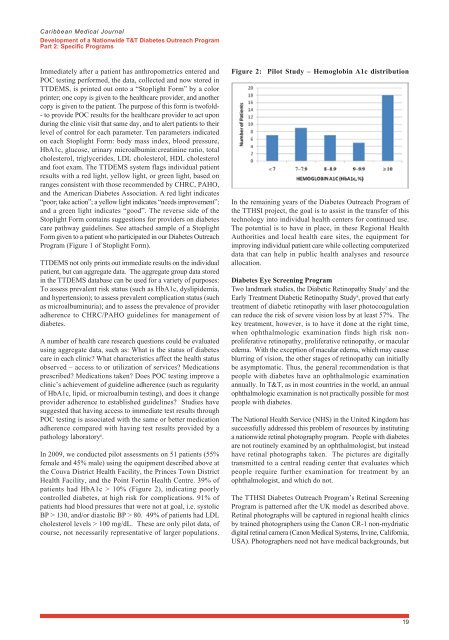
In 2009, we conducted pilot assessments on 51 patients (55%<br />
female <strong>and</strong> 45% male) using <strong>the</strong> equipment described above at<br />
<strong>the</strong> Couva District Health Facility, <strong>the</strong> Princes Town District<br />
Health Facility, <strong>and</strong> <strong>the</strong> Point Fortin Health Centre. 39% of<br />
patients had HbA1c > 10% (Figure 2), indicating poorly<br />
controlled diabetes, at high risk for complications. 91% of<br />
patients had blood pressures that were not at goal, i.e. systolic<br />
BP > 130, <strong>and</strong>/or diastolic BP > 80. 49% of patients had LDL<br />
cholesterol levels > 100 mg/dL. <strong>The</strong>se are only pilot data, of<br />
course, not necessarily representative of larger populations.<br />
Figure 2: Pilot Study – Hemoglobin A1c distribution<br />
In <strong>the</strong> remaining years of <strong>the</strong> Diabetes Outreach Program of<br />
<strong>the</strong> TTHSI project, <strong>the</strong> goal is to assist in <strong>the</strong> transfer of this<br />
technology into individual health centers for continued use.<br />
<strong>The</strong> potential is to have in place, in <strong>the</strong>se Regional Health<br />
Authorities <strong>and</strong> local health care sites, <strong>the</strong> equipment for<br />
improving individual patient care while collecting computerized<br />
data that can help in public health analyses <strong>and</strong> resource<br />
allocation.<br />
Diabetes Eye Screening Program<br />
Two l<strong>and</strong>mark studies, <strong>the</strong> Diabetic Retinopathy Study 7 <strong>and</strong> <strong>the</strong><br />
Early Treatment Diabetic Retinopathy Study 8 , proved that early<br />
treatment of diabetic retinopathy with laser photocoagulation<br />
can reduce <strong>the</strong> risk of severe vision loss by at least 57%. <strong>The</strong><br />
key treatment, however, is to have it done at <strong>the</strong> right time,<br />
when ophthalmologic examination finds high risk nonproliferative<br />
retinopathy, proliferative retinopathy, or macular<br />
edema. With <strong>the</strong> exception of macular edema, which may cause<br />
blurring of vision, <strong>the</strong> o<strong>the</strong>r stages of retinopathy can initially<br />
be asymptomatic. Thus, <strong>the</strong> general recommendation is that<br />
people with diabetes have an ophthalmologic examination<br />
annually. In T&T, as in most countries in <strong>the</strong> world, an annual<br />
ophthalmologic examination is not practically possible for most<br />
people with diabetes.<br />
<strong>The</strong> National Health Service (NHS) in <strong>the</strong> United Kingdom has<br />
successfully addressed this problem of resources by instituting<br />
a nationwide retinal photography program. People with diabetes<br />
are not routinely examined by an ophthalmologist, but instead<br />
have retinal photographs taken. <strong>The</strong> pictures are digitally<br />
transmitted to a central reading center that evaluates which<br />
people require fur<strong>the</strong>r examination for treatment by an<br />
ophthalmologist, <strong>and</strong> which do not.<br />
<strong>The</strong> TTHSI Diabetes Outreach Program’s Retinal Screening<br />
Program is patterned after <strong>the</strong> UK model as described above.<br />
Retinal photographs will be captured in regional health clinics<br />
by trained photographers using <strong>the</strong> Canon CR-1 non-mydriatic<br />
digital retinal camera (Canon <strong>Medical</strong> Systems, Irvine, California,<br />
USA). Photographers need not have medical backgrounds, but<br />
19