

Front Matter (PDF) - Investigative Ophthalmology & Visual Science
Front Matter (PDF) - Investigative Ophthalmology & Visual Science
Front Matter (PDF) - Investigative Ophthalmology & Visual Science

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
FME<br />
PredFbrte<br />
(fluorometholone) (prednisolone acetate) 1%<br />
FML vs Pred Forte: A choice. Both FML and Pred Forte work. FML has been shown to have<br />
less propensity than dexamethasone to raise IOR And recent animal data 3 indicate that Pred Forte<br />
exhibits maximal corneal penetration, through intact epithelium, compared to commonly used<br />
steroid phosphate and alcohol derivatives. So when potent anti-inflammatory activity is required<br />
and your clinical judgement anticipates something beyond short-term therapy, FML appears to be<br />
the drug of choice. But for severe disorders where safety is less of a concern, Pred Forte<br />
provides a potent alternative to FML.<br />
Potency you can see<br />
y<br />
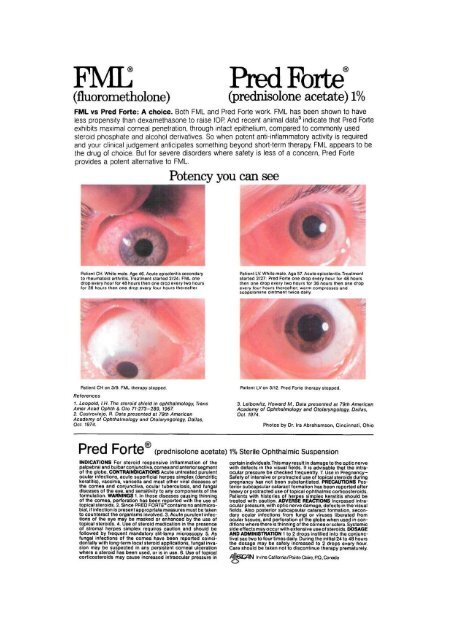
Patient CH. White male. Age 46. Acute episcleritis secondary<br />
to rheumatoid arthritis. Treatment started 2/24: FML one<br />
drop every hour for 48 hours then one drop every two hours<br />
for 36 hours then one drop every four hours thereafter<br />
r<br />
Patient CH on 3/9. FML therapy stopped.<br />
References<br />
1. Leopold, I.H. The steroid shield in ophthalmology, Trans<br />
Amer Acad Ophth & Oto 71:273-289, 1967,<br />
2. Castroviejo, R. Data presented at 79th American<br />
Academy of <strong>Ophthalmology</strong> and Ototaryngology, Dallas,<br />
Oct. 1974.<br />
Patient LV. White male. Age 57. Acute episcleritis. Treatment<br />
started 2/27: Pred Forte one drop every hour for 48 hours<br />
then one drop every two hours for 36 hours then one drop<br />
every four hours thereafter; warm compresses and<br />
scopolamine ointment twice daily.<br />
Patient LV on 3/12. Pred Forte therapy stopped.<br />
3. Leibowitz, Howard M., Data presented at 79th American<br />
Academy of <strong>Ophthalmology</strong> and Ototaryngology, Dallas,<br />
Oct. 1974.<br />
Photos by Dr. Ira Abrahamson, Cincinnati, Ohio<br />
Pred Forte' (prednisolone acetate) 1% Sterile Ophthalmic Suspension<br />
INDICATIONS For steroid responsive inflammation of the<br />
palpebral and bulbar conjunctiva, cornea and anterior segment<br />
of the globe. CONTRAINDICATIONS Acute untreated purulent<br />
ocular infections, acute superficial herpes simplex (dendritic<br />
keratitis), vaccinia, varicella and most other viral diseases of<br />
the cornea and conjunctiva, ocular tuberculosis, and fungal<br />
diseases of the eye, and sensitivity to any components of the<br />
formulation. WARNINGS 1. In those diseases causing thinning<br />
of the cornea, perforation has been reported with the use of<br />
topical steroids. 2. Since PRED FORTE® contains no antimicrobial,<br />
if infection is present appropriate measures must be taken<br />
to counteract the organisms involved. 3. Acute purulent infections<br />
of the eye may be masked or enhanced by the use of<br />
topical steroids. 4. Use of steroid medication in the presence<br />
of stromal herpes simplex requires caution and should be<br />
followed by frequent mandatory slit-lamp microscopy. 5. As<br />
fungal infections of the cornea have been reported coincidentally<br />
with long-term local steroid applications, fungal invasion<br />
may be suspected in any persistent corneal ulceration<br />
where a steroid has been used, or is in use. 6. Use of topical<br />
corticosteroids may cause increased intraocular pressure in<br />
certain individuals.This may result in damage to the optic nerve<br />
with defects in the visual fields. It is advisable that the intraocular<br />
pressure be checked frequently. 7. Use in Pregnancy-<br />
Safety of intensive or protracted use of topical steroids during<br />
pregnancy has not been substantiated. PRECAUTIONS Posterior<br />
subcapsular cataract formation has been reported after<br />
heavy or protracted use of topical ophthalmic corticosteroids.<br />
Patients with histories of herpes simplex keratitis should be<br />
treated with caution. ADVERSE REACTIONS Increased intraocular<br />
pressure, with optic nerve damage, defects in the visual<br />
fields. Also posterior subcapsular cataract formation, secondary<br />
ocular infections from fungi or viruses liberated from<br />
ocular tissues, and perforation of the globe when used in conditions<br />
where there is thinning of the cornea o r sclera. Systemic<br />
side effects may occur with extensive use of steroids. DOSAGE<br />
AND ADMINISTRATION 1 to 2 drops instilled into the conjunctival<br />
sac two to four times daily. During the initial 24 to 48 hours<br />
the dosage may be safely increased to 2 drops every hour.<br />
Care should be taken not to discontinue therapy prematurely.<br />
Irvine Califaria/PohteClaire,P.Q.,Canada














