South African Psychiatry - February 2019
South African Psychiatry - February 2019
South African Psychiatry - February 2019

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
FEATURE<br />
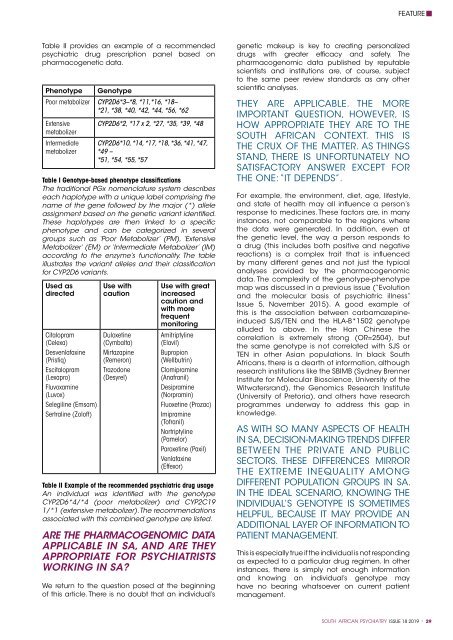
Table II provides an example of a recommended<br />
psychiatric drug prescription panel based on<br />
pharmacogenetic data.<br />
Phenotype<br />
Genotype<br />
Poor metabolizer CYP2D6*3–*8, *11,*16, *18–<br />
*21, *38, *40, *42, *44, *56, *62<br />
Extensive<br />
metabolizer<br />
Intermediate<br />
metabolizer<br />
CYP2D6*2, *17 x 2, *27, *35, *39, *48<br />
CYP2D6*10, *14, *17, *18, *36, *41, *47,<br />
*49 –<br />
*51, *54, *55, *57<br />
Table I Genotype-based phenotype classifications<br />
The traditional PGx nomenclature system describes<br />
each haplotype with a unique label comprising the<br />
name of the gene followed by the major (*) allele<br />
assignment based on the genetic variant identified.<br />
These haplotypes are then linked to a specific<br />
phenotype and can be categorized in several<br />
groups such as ‘Poor Metabolizer’ (PM), ‘Extensive<br />
Metabolizer’ (EM) or ‘Intermediate Metabolizer’ (IM)<br />
according to the enzyme’s functionality. The table<br />
illustrates the variant alleles and their classification<br />
for CYP2D6 variants.<br />
Used as<br />
directed<br />
Citalopram<br />
(Celexa)<br />
Desvenlafaxine<br />
(Pristiq)<br />
Escitalopram<br />
(Lexapro)<br />
Fluvoxamine<br />
(Luvox)<br />
Selegiline (Emsam)<br />
Sertraline (Zoloft)<br />
Use with<br />
caution<br />
Duloxetine<br />
(Cymbalta)<br />
Mirtazapine<br />
(Remeron)<br />
Trazodone<br />
(Desyrel)<br />
Use with great<br />
increased<br />
caution and<br />
with more<br />
frequent<br />
monitoring<br />
Amitriptyline<br />
(Elavil)<br />
Bupropion<br />
(Wellbutrin)<br />
Clomipramine<br />
(Anafranil)<br />
Desipramine<br />
(Norpramin)<br />
Fluoxetine (Prozac)<br />
Imipramine<br />
(Tofranil)<br />
Nortriptyline<br />
(Pamelor)<br />
Paroxetine (Paxil)<br />
Venlafaxine<br />
(Effexor)<br />
Table II Example of the recommended psychiatric drug usage<br />
An individual was identified with the genotype<br />
CYP2D6*4/*4 (poor metabolizer) and CYP2C19<br />
1/*1 (extensive metabolizer). The recommendations<br />
associated with this combined genotype are listed.<br />
ARE THE PHARMACOGENOMIC DATA<br />
APPLICABLE IN SA, AND ARE THEY<br />
APPROPRIATE FOR PSYCHIATRISTS<br />
WORKING IN SA?<br />
We return to the question posed at the beginning<br />
of this article. There is no doubt that an individual’s<br />
genetic makeup is key to creating personalized<br />
drugs with greater efficacy and safety. The<br />
pharmacogenomic data published by reputable<br />
scientists and institutions are, of course, subject<br />
to the same peer review standards as any other<br />
scientific analyses.<br />
THEY ARE APPLICABLE. THE MORE<br />
IMPORTANT QUESTION, HOWEVER, IS<br />
HOW APPROPRIATE THEY ARE TO THE<br />
SOUTH AFRICAN CONTEXT. THIS IS<br />
THE CRUX OF THE MATTER. AS THINGS<br />
STAND, THERE IS UNFORTUNATELY NO<br />
SATISFACTORY ANSWER EXCEPT FOR<br />
THE ONE: “IT DEPENDS”.<br />
For example, the environment, diet, age, lifestyle,<br />
and state of health may all influence a person’s<br />
response to medicines. These factors are, in many<br />
instances, not comparable to the regions where<br />
the data were generated. In addition, even at<br />
the genetic level, the way a person responds to<br />
a drug (this includes both positive and negative<br />
reactions) is a complex trait that is influenced<br />
by many different genes and not just the typical<br />
analyses provided by the pharmacogenomic<br />
data. The complexity of the genotype-phenotype<br />
map was discussed in a previous issue (“Evolution<br />
and the molecular basis of psychiatric illness”<br />
Issue 5, November 2015). A good example of<br />
this is the association between carbamazepineinduced<br />
SJS/TEN and the HLA-B*1502 genotype<br />
alluded to above. In the Han Chinese the<br />
correlation is extremely strong (OR=2504), but<br />
the same genotype is not correlated with SJS or<br />
TEN in other Asian populations. In black <strong>South</strong><br />
<strong>African</strong>s, there is a dearth of information, although<br />
research institutions like the SBIMB (Sydney Brenner<br />
Institute for Molecular Bioscience, University of the<br />
Witwatersrand), the Genomics Research Institute<br />
(University of Pretoria), and others have research<br />
programmes underway to address this gap in<br />
knowledge.<br />
AS WITH SO MANY ASPECTS OF HEALTH<br />
IN SA, DECISION-MAKING TRENDS DIFFER<br />
BETWEEN THE PRIVATE AND PUBLIC<br />
SECTORS. THESE DIFFERENCES MIRROR<br />
THE EXTREME INEQUALITY AMONG<br />
DIFFERENT POPULATION GROUPS IN SA.<br />
IN THE IDEAL SCENARIO, KNOWING THE<br />
INDIVIDUAL’S GENOTYPE IS SOMETIMES<br />
HELPFUL, BECAUSE IT MAY PROVIDE AN<br />
ADDITIONAL LAYER OF INFORMATION TO<br />
PATIENT MANAGEMENT.<br />
This is especially true if the individual is not responding<br />
as expected to a particular drug regimen. In other<br />
instances, there is simply not enough information<br />
and knowing an individual’s genotype may<br />
have no bearing whatsoever on current patient<br />
management.<br />
SOUTH AFRICAN PSYCHIATRY ISSUE 18 <strong>2019</strong> * 29