FRCEM FINAL SBA eBook 1(Preview)
FRCEM FINAL SBA book is designed to present concise, easy-to-read, practical information on the diagnosis and treatment of a wide spectrum of conditions that present to the emergency department. The chapters emphasize the immediate management of life-threatening problems & then present the evaluation and treatment of specific disorders. In keeping with the curriculum spanning ST 1- ST 6 I have strived to provide the reader with a broad-based text written in a clear and point form manner. My goal was to not only provide practising emergency physicians quick access to accurate and useful information that will aid in their everyday practice of emergency medicine but also mainly to help trainees throughout their 6-year training in Emergency Medicine. Because this text focuses on the practical aspects of emergency care, there is little discussion of disease processes' basic science or pathophysiology. This is the only book of its kind available which covers the entire curriculum and helps prepare for the FINAL Clinical SAQ. The book will be useful to all practitioners of Emergency Medicine, including Physicians, Residents, Medical Students as well as Physician Extenders.
FRCEM FINAL SBA book is designed to present concise, easy-to-read, practical information on the diagnosis and treatment of a wide spectrum of conditions that present to the emergency department.
The chapters emphasize the immediate management of life-threatening problems & then present the evaluation and treatment of specific disorders.
In keeping with the curriculum spanning ST 1- ST 6 I have strived to provide the reader with a broad-based text written in a clear and point form manner.
My goal was to not only provide practising emergency physicians quick access to accurate and useful information that will aid in their everyday practice of emergency medicine but also mainly to help trainees throughout their 6-year training in Emergency Medicine.
Because this text focuses on the practical aspects of emergency care, there is little discussion of disease processes' basic science or pathophysiology.
This is the only book of its kind available which covers the entire curriculum and helps prepare for the FINAL Clinical SAQ.
The book will be useful to all practitioners of Emergency Medicine, including Physicians, Residents, Medical Students as well as Physician Extenders.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
4 <strong>FRCEM</strong> Final<br />
• Common examples of referred pain are scapular pain<br />
due to biliary colic, groin pain due to renal colic, and<br />
shoulder pain due to blood or infection irritating the<br />
diaphragm.<br />
5. CLINICAL ASSESSMENT<br />
HISTORY<br />
• When possible, the history should be obtained from a<br />
nonsedated patient. The initial differential diagnosis can<br />
be determined by a delineation of the pain's location,<br />
radiation, and movement (e.g., appendicitis-associated<br />
pain usually moves from the periumbilical area to the<br />
right lower quadrant of the abdomen). After the location<br />
is identified, the physician should obtain general<br />
information about onset, duration, severity, and quality<br />
of pain and about exacerbating and remitting factors.<br />
• Associated symptoms often allow the physician to<br />
further focus the differential diagnosis.<br />
• For bowel obstruction, constipation is the symptom<br />
with the highest positive predictive value.<br />
• For appendicitis, right lower quadrant pain has the<br />
highest positive predictive value, although migration<br />
from periumbilical to right lower quadrant pain and fever<br />
also suggest appendicitis. Some conditions that were<br />
historically considered useful in diagnosing abdominal<br />
pain (e.g., anorexia in patients with appendicitis) have<br />
been found to have little predictive value.<br />
• Colic (i.e., sharp, localized abdominal pain that increases,<br />
peaks, and subsides) is associated with numerous<br />
diseases of hollow viscera. The mechanism of pain is<br />
thought to be smooth muscle contraction proximal to a<br />
partial or complete obstruction (e.g., gallstone, kidney<br />
stone, small bowel obstruction). Although colic is<br />
associated with several diseases, the location of colic<br />
may help diagnose the cause. The absence of colic is<br />
useful for ruling out diseases such as acute cholecystitis;<br />
less than 25 percent of patients with acute cholecystitis<br />
present without right upper quadrant pain or colic.<br />
• Peptic ulcer disease is often associated with Helicobacter<br />
pylori infection (75 to 95 percent of duodenal ulcers and<br />
65 to 95 percent of gastric ulcers), 3 although most<br />
patients do not know their H. pylori status. In addition,<br />
many patients with ulcer disease and serology findings<br />
negative for H. pylori report recent use of nonsteroidal<br />
anti-inflammatory drugs.<br />
• Other symptoms of peptic ulcer disease include<br />
concurrent, episodic gnawing or burning pain; pain<br />
relieved by food; and nighttime awakening with pain.<br />
3 Srinivasan R, Greenbaum DS. Chronic abdominal wall pain: a frequently<br />
overlooked problem. Practical approach to diagnosis and management. Am<br />
J Gastroenterol. 2002;97(4):824–830.<br />
• Symptoms in patients with abdominal pain that are<br />
suggestive of surgical or emergent conditions include<br />
fever, protracted vomiting, syncope or presyncope, and<br />
evidence of gastrointestinal blood loss.<br />
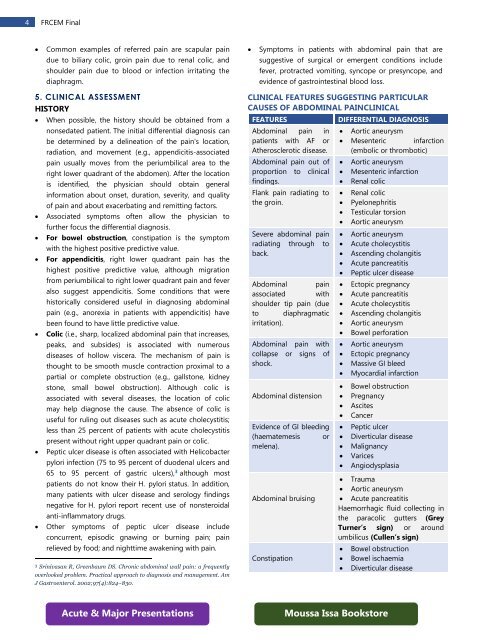
CLINICAL FEATURES SUGGESTING PARTICULAR<br />
CAUSES OF ABDOMINAL PAINCLINICAL<br />
FEATURES<br />
Abdominal pain in<br />
patients with AF or<br />
Atherosclerotic disease.<br />
Abdominal pain out of<br />
proportion to clinical<br />
findings.<br />
Flank pain radiating to<br />
the groin.<br />
Severe abdominal pain<br />
radiating through to<br />
back.<br />
Abdominal pain<br />
associated with<br />
shoulder tip pain (due<br />
to diaphragmatic<br />
irritation).<br />
Abdominal pain with<br />
collapse or signs of<br />
shock.<br />
Abdominal distension<br />
Evidence of GI bleeding<br />
(haematemesis or<br />
melena).<br />
Abdominal bruising<br />
Constipation<br />
DIFFERENTIAL DIAGNOSIS<br />
• Aortic aneurysm<br />
• Mesenteric infarction<br />
(embolic or thrombotic)<br />
• Aortic aneurysm<br />
• Mesenteric infarction<br />
• Renal colic<br />
• Renal colic<br />
• Pyelonephritis<br />
• Testicular torsion<br />
• Aortic aneurysm<br />
• Aortic aneurysm<br />
• Acute cholecystitis<br />
• Ascending cholangitis<br />
• Acute pancreatitis<br />
• Peptic ulcer disease<br />
• Ectopic pregnancy<br />
• Acute pancreatitis<br />
• Acute cholecystitis<br />
• Ascending cholangitis<br />
• Aortic aneurysm<br />
• Bowel perforation<br />
• Aortic aneurysm<br />
• Ectopic pregnancy<br />
• Massive GI bleed<br />
• Myocardial infarction<br />
• Bowel obstruction<br />
• Pregnancy<br />
• Ascites<br />
• Cancer<br />
• Peptic ulcer<br />
• Diverticular disease<br />
• Malignancy<br />
• Varices<br />
• Angiodysplasia<br />
• Trauma<br />
• Aortic aneurysm<br />
• Acute pancreatitis<br />
Haemorrhagic fluid collecting in<br />
the paracolic gutters (Grey<br />
Turner’s sign) or around<br />
umbilicus (Cullen’s sign)<br />
• Bowel obstruction<br />
• Bowel ischaemia<br />
• Diverticular disease<br />
Acute & Major Presentations<br />
Moussa Issa Bookstore