FRCEM FINAL SBA eBook 1(Preview)
FRCEM FINAL SBA book is designed to present concise, easy-to-read, practical information on the diagnosis and treatment of a wide spectrum of conditions that present to the emergency department. The chapters emphasize the immediate management of life-threatening problems & then present the evaluation and treatment of specific disorders. In keeping with the curriculum spanning ST 1- ST 6 I have strived to provide the reader with a broad-based text written in a clear and point form manner. My goal was to not only provide practising emergency physicians quick access to accurate and useful information that will aid in their everyday practice of emergency medicine but also mainly to help trainees throughout their 6-year training in Emergency Medicine. Because this text focuses on the practical aspects of emergency care, there is little discussion of disease processes' basic science or pathophysiology. This is the only book of its kind available which covers the entire curriculum and helps prepare for the FINAL Clinical SAQ. The book will be useful to all practitioners of Emergency Medicine, including Physicians, Residents, Medical Students as well as Physician Extenders.
FRCEM FINAL SBA book is designed to present concise, easy-to-read, practical information on the diagnosis and treatment of a wide spectrum of conditions that present to the emergency department.
The chapters emphasize the immediate management of life-threatening problems & then present the evaluation and treatment of specific disorders.
In keeping with the curriculum spanning ST 1- ST 6 I have strived to provide the reader with a broad-based text written in a clear and point form manner.
My goal was to not only provide practising emergency physicians quick access to accurate and useful information that will aid in their everyday practice of emergency medicine but also mainly to help trainees throughout their 6-year training in Emergency Medicine.
Because this text focuses on the practical aspects of emergency care, there is little discussion of disease processes' basic science or pathophysiology.
This is the only book of its kind available which covers the entire curriculum and helps prepare for the FINAL Clinical SAQ.
The book will be useful to all practitioners of Emergency Medicine, including Physicians, Residents, Medical Students as well as Physician Extenders.

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
26 <strong>FRCEM</strong> Final<br />
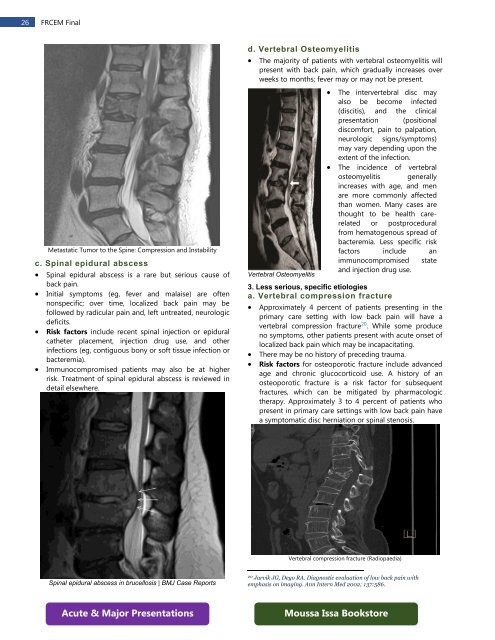
Metastatic Tumor to the Spine: Compression and Instability<br />
c. Spinal epidural abscess<br />
• Spinal epidural abscess is a rare but serious cause of<br />
back pain.<br />
• Initial symptoms (eg, fever and malaise) are often<br />
nonspecific; over time, localized back pain may be<br />
followed by radicular pain and, left untreated, neurologic<br />
deficits.<br />
• Risk factors include recent spinal injection or epidural<br />
catheter placement, injection drug use, and other<br />
infections (eg, contiguous bony or soft tissue infection or<br />
bacteremia).<br />
• Immunocompromised patients may also be at higher<br />
risk. Treatment of spinal epidural abscess is reviewed in<br />
detail elsewhere.<br />
d. Vertebral Osteomyelitis<br />
• The majority of patients with vertebral osteomyelitis will<br />
present with back pain, which gradually increases over<br />
weeks to months; fever may or may not be present.<br />
Vertebral Osteomyelitis<br />
• The intervertebral disc may<br />
also be become infected<br />
(discitis), and the clinical<br />
presentation (positional<br />
discomfort, pain to palpation,<br />
neurologic signs/symptoms)<br />
may vary depending upon the<br />
extent of the infection.<br />
• The incidence of vertebral<br />
osteomyelitis generally<br />
increases with age, and men<br />
are more commonly affected<br />
than women. Many cases are<br />
thought to be health carerelated<br />
or postprocedural<br />
from hematogenous spread of<br />
bacteremia. Less specific risk<br />
factors include an<br />
immunocompromised state<br />
and injection drug use.<br />
3. Less serious, specific etiologies<br />
a. Vertebral compression fracture<br />
• Approximately 4 percent of patients presenting in the<br />
primary care setting with low back pain will have a<br />
vertebral compression fracture 20 . While some produce<br />
no symptoms, other patients present with acute onset of<br />
localized back pain which may be incapacitating.<br />
• There may be no history of preceding trauma.<br />
• Risk factors for osteoporotic fracture include advanced<br />
age and chronic glucocorticoid use. A history of an<br />
osteoporotic fracture is a risk factor for subsequent<br />
fractures, which can be mitigated by pharmacologic<br />
therapy. Approximately 3 to 4 percent of patients who<br />
present in primary care settings with low back pain have<br />
a symptomatic disc herniation or spinal stenosis.<br />
Vertebral compression fracture (Radiopaedia)<br />
Spinal epidural abscess in brucellosis | BMJ Case Reports<br />
20 Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with<br />
emphasis on imaging. Ann Intern Med 2002; 137:586.<br />
Acute & Major Presentations<br />
Moussa Issa Bookstore