

SRPS PS - Plastic Surgery Internal
SRPS PS - Plastic Surgery Internal
SRPS PS - Plastic Surgery Internal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
The dorsal middle phalangeal finger flap 393–395 can be<br />
raised on a short or long antegrade or retrograde<br />
pedicle and can be used as a free flap, an arterial and/or<br />
venous flow-through flap, or a neurovascular flap.<br />
Heterodigital Flaps<br />
In 1951, Cronin first described the cross-finger flap for<br />
fingertip reconstruction. 396 The cross-finger flap brings<br />
durable cover to exposed bone, joint, or flexor tendons<br />
when homodigital flaps do not suffice. 396–400 Blood<br />
supply of the cross-finger flap is random and based on<br />
the subdermal plexus of an adjacent digit. The flap can<br />
be based laterally, proximally, or distally, depending on<br />
the most comfortable approximation of donor digit to<br />
defect. The dorsum of the middle phalanges of the<br />
index, middle, and ring fingers is the most appropriate<br />
donor site in terms of joint immobilization. Use of a<br />
cross-finger flap from the volar aspect of the middle<br />
finger, rather than from the thinner dorsal finger skin,<br />
provides better tissue quality for resurfacing the pulp<br />
of the thumb. 365,401<br />
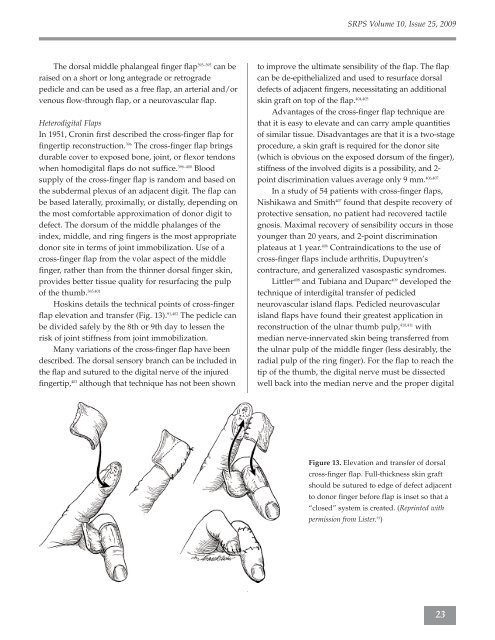
Hoskins details the technical points of cross-finger<br />
flap elevation and transfer (Fig. 13). 91,402 The pedicle can<br />
be divided safely by the 8th or 9th day to lessen the<br />
risk of joint stiffness from joint immobilization.<br />
Many variations of the cross-finger flap have been<br />
described. The dorsal sensory branch can be included in<br />
the flap and sutured to the digital nerve of the injured<br />
fingertip, 403 although that technique has not been shown<br />
<strong>SR<strong>PS</strong></strong> Volume 10, Issue 25, 2009<br />
to improve the ultimate sensibility of the flap. The flap<br />
can be de-epithelialized and used to resurface dorsal<br />
defects of adjacent fingers, necessitating an additional<br />
skin graft on top of the flap. 404,405<br />
Advantages of the cross-finger flap technique are<br />
that it is easy to elevate and can carry ample quantities<br />
of similar tissue. Disadvantages are that it is a two-stage<br />
procedure, a skin graft is required for the donor site<br />
(which is obvious on the exposed dorsum of the finger),<br />
stiffness of the involved digits is a possibility, and 2point<br />
discrimination values average only 9 mm. 406,407<br />
In a study of 54 patients with cross-finger flaps,<br />
Nishikawa and Smith 407 found that despite recovery of<br />
protective sensation, no patient had recovered tactile<br />
gnosis. Maximal recovery of sensibility occurs in those<br />
younger than 20 years, and 2-point discrimination<br />
plateaus at 1 year. 406 Contraindications to the use of<br />
cross-finger flaps include arthritis, Dupuytren’s<br />
contracture, and generalized vasospastic syndromes.<br />
Littler 408 and Tubiana and Duparc 409 developed the<br />
technique of interdigital transfer of pedicled<br />
neurovascular island flaps. Pedicled neurovascular<br />
island flaps have found their greatest application in<br />
reconstruction of the ulnar thumb pulp, 410,411 with<br />
median nerve-innervated skin being transferred from<br />
the ulnar pulp of the middle finger (less desirably, the<br />
radial pulp of the ring finger). For the flap to reach the<br />
tip of the thumb, the digital nerve must be dissected<br />
well back into the median nerve and the proper digital<br />
Figure 13. Elevation and transfer of dorsal<br />
cross-finger flap. Full-thickness skin graft<br />
should be sutured to edge of defect adjacent<br />
to donor finger before flap is inset so that a<br />
“closed” system is created. (Reprinted with<br />
permission from Lister. 91 )<br />
23



