

SRPS PS - Plastic Surgery Internal
SRPS PS - Plastic Surgery Internal
SRPS PS - Plastic Surgery Internal

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
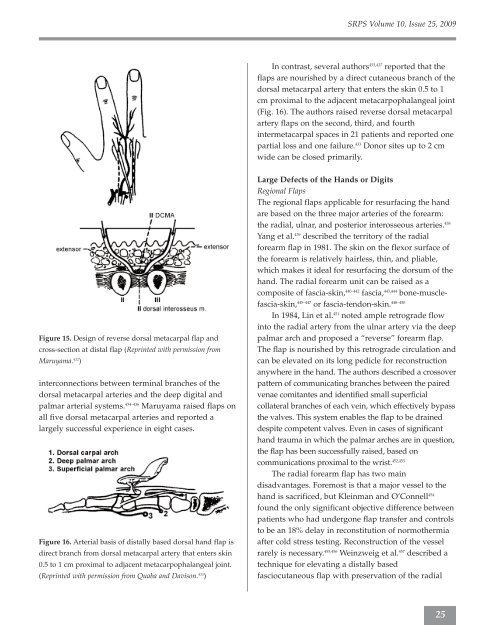
Figure 15. Design of reverse dorsal metacarpal flap and<br />
cross-section at distal flap (Reprinted with permission from<br />
Maruyama. 432 )<br />
interconnections between terminal branches of the<br />
dorsal metacarpal arteries and the deep digital and<br />
palmar arterial systems. 434–436 Maruyama raised flaps on<br />
all five dorsal metacarpal arteries and reported a<br />
largely successful experience in eight cases.<br />
Figure 16. Arterial basis of distally based dorsal hand flap is<br />
direct branch from dorsal metacarpal artery that enters skin<br />
0.5 to 1 cm proximal to adjacent metacarpophalangeal joint.<br />
(Reprinted with permission from Quaba and Davison. 433 )<br />
<strong>SR<strong>PS</strong></strong> Volume 10, Issue 25, 2009<br />
In contrast, several authors 433,437 reported that the<br />
flaps are nourished by a direct cutaneous branch of the<br />
dorsal metacarpal artery that enters the skin 0.5 to 1<br />
cm proximal to the adjacent metacarpophalangeal joint<br />
(Fig. 16). The authors raised reverse dorsal metacarpal<br />
artery flaps on the second, third, and fourth<br />
intermetacarpal spaces in 21 patients and reported one<br />
partial loss and one failure. 433 Donor sites up to 2 cm<br />
wide can be closed primarily.<br />
Large Defects of the Hands or Digits<br />
Regional Flaps<br />
The regional flaps applicable for resurfacing the hand<br />
are based on the three major arteries of the forearm:<br />
the radial, ulnar, and posterior interosseous arteries. 438<br />
Yang et al. 439 described the territory of the radial<br />
forearm flap in 1981. The skin on the flexor surface of<br />
the forearm is relatively hairless, thin, and pliable,<br />
which makes it ideal for resurfacing the dorsum of the<br />
hand. The radial forearm unit can be raised as a<br />
composite of fascia-skin, 440–442 fascia, 443,444 bone-musclefascia-skin,<br />
445–447 or fascia-tendon-skin. 448–450<br />
In 1984, Lin et al. 451 noted ample retrograde flow<br />
into the radial artery from the ulnar artery via the deep<br />
palmar arch and proposed a “reverse” forearm flap.<br />
The flap is nourished by this retrograde circulation and<br />
can be elevated on its long pedicle for reconstruction<br />
anywhere in the hand. The authors described a crossover<br />
pattern of communicating branches between the paired<br />
venae comitantes and identified small superficial<br />
collateral branches of each vein, which effectively bypass<br />
the valves. This system enables the flap to be drained<br />
despite competent valves. Even in cases of significant<br />
hand trauma in which the palmar arches are in question,<br />
the flap has been successfully raised, based on<br />
communications proximal to the wrist. 452,453<br />
The radial forearm flap has two main<br />
disadvantages. Foremost is that a major vessel to the<br />
hand is sacrificed, but Kleinman and O’Connell 454<br />
found the only significant objective difference between<br />
patients who had undergone flap transfer and controls<br />
to be an 18% delay in reconstitution of normothermia<br />
after cold stress testing. Reconstruction of the vessel<br />
rarely is necessary. 455,456 Weinzweig et al. 457 described a<br />
technique for elevating a distally based<br />
fasciocutaneous flap with preservation of the radial<br />
25



