Birmingham H ip Resurfacing v ersus C onserv e Plus M etal-on-M ...
Birmingham H ip Resurfacing v ersus C onserv e Plus M etal-on-M ...
Birmingham H ip Resurfacing v ersus C onserv e Plus M etal-on-M ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Copyright Dr. Koen De Smet<br />
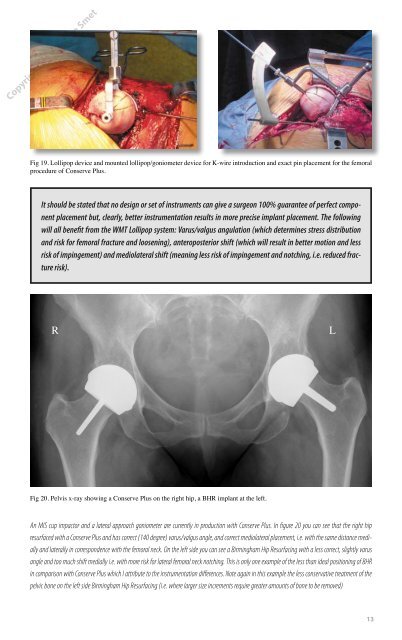
Fig 19. Loll<str<strong>on</strong>g>ip</str<strong>on</strong>g>op device and mounted loll<str<strong>on</strong>g>ip</str<strong>on</strong>g>op/g<strong>on</strong>iometer device for K-wire introducti<strong>on</strong> and exact pin placement for the femoral<br />
procedure of C<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>e <str<strong>on</strong>g>Plus</str<strong>on</strong>g>.<br />
It should be stated that no design or set of instruments can give a surge<strong>on</strong> 100% guarantee of perfect comp<strong>on</strong>ent<br />
placement but, clearly, better instrumentati<strong>on</strong> results in more precise implant placement. The following<br />
will all benefit from the WMT Loll<str<strong>on</strong>g>ip</str<strong>on</strong>g>op system: Varus/valgus angulati<strong>on</strong> (which determines stress distributi<strong>on</strong><br />
and risk for femoral fracture and loosening), anteroposterior shift (which will result in better moti<strong>on</strong> and less<br />
risk of impingement) and mediolateral shift (meaning less risk of impingement and notching, i.e. reduced fracture<br />
risk).<br />
R L<br />
Fig 20. Pelvis x-ray showing a C<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>e <str<strong>on</strong>g>Plus</str<strong>on</strong>g> <strong>on</strong> the right h<str<strong>on</strong>g>ip</str<strong>on</strong>g>, a BHR implant at the left.<br />
An MIS cup impactor and a lateral approach g<strong>on</strong>iometer are currently in producti<strong>on</strong> with C<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>e <str<strong>on</strong>g>Plus</str<strong>on</strong>g>. In figure 20 you can see that the right h<str<strong>on</strong>g>ip</str<strong>on</strong>g><br />
resurfaced with a C<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>e <str<strong>on</strong>g>Plus</str<strong>on</strong>g> and has correct (140 degree) varus/valgus angle, and correct mediolateral placement, i.e. with the same distance medially<br />
and laterally in corresp<strong>on</strong>dence with the femoral neck. On the left side you can see a <str<strong>on</strong>g>Birmingham</str<strong>on</strong>g> H<str<strong>on</strong>g>ip</str<strong>on</strong>g> <str<strong>on</strong>g>Resurfacing</str<strong>on</strong>g> with a less correct, slightly varus<br />
angle and too much shift medially i.e. with more risk for lateral femoral neck notching. This is <strong>on</strong>ly <strong>on</strong>e example of the less than ideal positi<strong>on</strong>ing of BHR<br />
in comparis<strong>on</strong> with C<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>e <str<strong>on</strong>g>Plus</str<strong>on</strong>g> which I attribute to the instrumentati<strong>on</strong> differences. Note again in this example the less c<str<strong>on</strong>g><strong>on</strong>serv</str<strong>on</strong>g>ative treatment of the<br />
pelvic b<strong>on</strong>e <strong>on</strong> the left side <str<strong>on</strong>g>Birmingham</str<strong>on</strong>g> H<str<strong>on</strong>g>ip</str<strong>on</strong>g> <str<strong>on</strong>g>Resurfacing</str<strong>on</strong>g> (i.e. where larger size increments require greater amounts of b<strong>on</strong>e to be removed)<br />
13