Ehrlichia - VetLearn.com
Ehrlichia - VetLearn.com
Ehrlichia - VetLearn.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CE<br />
Vol. 24, No. 4 April 2002 277<br />
Article #1 (1.5 contact hours)<br />
Refereed Peer Review<br />
KEY FACTS<br />
■ <strong>Ehrlichia</strong>l infection can result in<br />
a wide range of manifestations<br />
(from inapparent infection to<br />
fatal illness).<br />
■ Diagnosis can be problematic<br />
because not all species of<br />
<strong>Ehrlichia</strong> produce cross-reactive<br />
antibody titers and positive titers<br />
may reflect either inactive<br />
infection or past exposure.<br />
■ Dogs and other domestic species<br />
have the potential to harbor ticks<br />
that can transmit certain types of<br />
ehrlichiosis to humans.<br />
Comments? Questions?<br />
Email: <strong>com</strong>pendium@medimedia.<strong>com</strong><br />
Web: <strong>VetLearn</strong>.<strong>com</strong> • Fax: 800-556-3288<br />
The Increasingly<br />
Complicated Story<br />
of <strong>Ehrlichia</strong><br />
University of Missouri-Columbia<br />
Diane E. Preziosi, DVM, DABVP*<br />
Leah A. Cohn, DVM, PhD, DACVIM<br />
ABSTRACT: Ehrlichiosis, once viewed as a rare disease in the United States, has be<strong>com</strong>e an<br />
increasingly <strong>com</strong>mon diagnosis in many regions of the country. Although <strong>Ehrlichia</strong> canis was<br />
the first species described and remains the best understood, many other species of <strong>Ehrlichia</strong><br />
are now known to infect dogs. The recognition of new types of ehrlichial infections has added<br />
<strong>com</strong>plexity to the diagnosis of ehrlichiosis. The importance of these pathogens has increased<br />
with the recognition of human ehrlichiosis.<br />
<strong>Ehrlichia</strong>l infection was first recognized as a cause of canine disease in Algeria<br />
circa 1935. 1 Veterinarians in the United States did not be<strong>com</strong>e familiar<br />
with this disease until the Vietnam War era when military working dogs,<br />
including many that had never left the country, developed what was then known<br />
as tropical pancytopenia caused by <strong>Ehrlichia</strong> canis. 2,3 Since then, other species of<br />
<strong>Ehrlichia</strong> that cause disease in dogs have been identified. Classification of these<br />
ehrlichial species has been reorganized, diagnostic testing options have increased,<br />
and additional manifestations of ehrlichiosis have been recognized in a wider<br />
geographic area. In the mid-1980s, an ehrlichial species was recognized as a<br />
cause of disease in humans in the United States; since then, various other species<br />
have been found to infect humans as well. Some ehrlichial species that infect<br />
dogs can also infect humans (through tick bites), leading to concerns about the<br />
role of dogs in harboring a disease that may be transmitted to humans. This article<br />
addresses these developments and their importance in the understanding,<br />
diagnosis, and treatment of ehrlichiosis primarily in dogs.<br />
CLASSIFICATION<br />
<strong>Ehrlichia</strong> are gram-negative obligate intracellular bacteria that lack<br />
lipopolysaccharide endotoxins and rely on arthropod vectors for transmission.<br />
For many years, E. canis was the only ehrlichial species known to cause disease in<br />
dogs, and it is by far the best described veterinary ehrlichial pathogen. Several<br />
additional <strong>Ehrlichia</strong> species that infect dogs as either primary or incidental hosts<br />
are now recognized. Previous classification schemes have made use of the cell<br />
*Dr. Preziosi is currently affiliated with the University of Pennsylvania.
278 Small Animal/Exotics Compendium April 2002<br />
Table 1. <strong>Ehrlichia</strong>l Agents Known to Infect Dogs<br />
Type Target Cells Major Host Known Vector(s)<br />
Genogroup I<br />
<strong>Ehrlichia</strong> canis Mononuclear cells Dogs Rhipicephalus sanguineus<br />
<strong>Ehrlichia</strong> chaffeensis Mononuclear cells Humans Amblyomma americanum, Dermacentor variabilis<br />
<strong>Ehrlichia</strong> ewingii Granulocytes Dogs R. sanguineus, A. americanum, D. variabilis<br />
Genogroup II<br />
<strong>Ehrlichia</strong> phagocytophila Granulocytes Ruminants Ixodes ricinus<br />
<strong>Ehrlichia</strong> equi Granulocytes Equidae I. ricinus, Ixodes pacificus<br />
Agent of human Granulocytes Humans Ixodes scapularis, I. ricinus, I. pacificus<br />
granulocytic ehrlichiosis<br />
<strong>Ehrlichia</strong> platys Platelets Dogs R. sanguineus<br />
Genogroup III<br />
<strong>Ehrlichia</strong> risticii Monocytes, enterocytes Equidae Arthropods<br />
Neorickettsia helminthoeca Monocytes Dogs Flukes<br />
type infected by the ehrlichial organism. Although this<br />
has proven useful, several species, such as <strong>Ehrlichia</strong><br />
ewingii, <strong>Ehrlichia</strong> chaffeensis, <strong>Ehrlichia</strong> risticii, and<br />
<strong>Ehrlichia</strong> phagocytophila, may infect more than one cell<br />
type. 4,5 Current classification schemes are based on<br />
genetic analysis of the organism’s 16S rRNA gene<br />
sequence. This method produces three species<br />
genogroups, with the members of any one genogroup<br />
<strong>com</strong>monly producing cross-reactive antibody titers. 5–8<br />
Despite close genetic relatedness, the individual species<br />
within a genogroup may infect different cells within<br />
different hosts, use different vectors, and have different<br />
geographic distributions (Table 1).<br />
EPIDEMIOLOGY<br />
Most ehrlichial species rely on arthropod vectors for<br />
transmission, although the specific vectors are not well<br />
described for every species of <strong>Ehrlichia</strong>. The geographic<br />
distribution pattern of various ehrlichial species is<br />
related to the distribution of the relevant vector(s). The<br />
predominant vector for E. canis is the brown dog tick<br />
(Rhipicephalus sanguineus), which is found worldwide. 9,10<br />
Accordingly, E. canis has been reported in dogs from<br />
Africa, Europe, Asia, the Middle East, and the United<br />
States. In contrast to E. canis, E. ewingii is known to use<br />
at least three different vectors. In addition to R. sanguineus,<br />
both Dermacentor variabilis (American dog<br />
tick) and Amblyomma americanum (lone star tick) are<br />
capable of transmitting E. ewingii infection. 10 The primary<br />
distribution of the lone star tick in the midwestern<br />
and southeastern United States may account for the<br />
increased incidence of E. ewingii infection in these<br />
regions. 5,6,10 <strong>Ehrlichia</strong> equi infection, which is transmitted<br />
by Ixodes ticks, is most often reported in the upper<br />
midwestern and northeastern United States. 7,11,12<br />
In addition to ticks, other known vectors of ehrlichial<br />
infection include snails and flukes. E. risticii, the<br />
causative agent of Potomac horse fever, is transmitted<br />
through the ingestion of snails and can cause infection<br />
in dogs as well as horses. 13 Although not often thought<br />
of as an ehrlichial species, Neorickettsia helminthoeca,<br />
the causative agent of salmon poisoning disease,<br />
belongs to the same genogroup as E. risticii. During a<br />
<strong>com</strong>plex life cycle, it is transmitted to dogs through the<br />
ingestion of flukes harbored in certain types of fish. 14<br />
The vectors of some ehrlichial species that affect dogs<br />
remain in<strong>com</strong>pletely defined.<br />
Concurrent infection with multiple arthropod-borne<br />
pathogens is possible and may contribute to illnesses<br />
described in some <strong>Ehrlichia</strong>-positive dogs. Dogs that<br />
harbor one tick are likely to harbor several (of either the<br />
same or different species). In addition, the same arthropod<br />
may serve as transmission vector for several genera<br />
and species of infectious agents. For instance, R. sanguineus<br />
is capable of transmitting not only E. canis and<br />
E. ewingii, but Babesia canis and Babesia gibsoni as<br />
well. 2,10,15–17 Ixodes ticks, <strong>com</strong>petent vectors for transmission<br />
of E. equi and the agent of human granulocytic<br />
ehrlichiosis (HGE), can also transmit infection with<br />
Borrelia burgdorferi and Babesia microti. 18–21 In addition<br />
to many case reports in the literature describing such<br />
concurrent infections, serologic surveys have documented<br />
these cases on a larger scale. In one such study, 6<br />
almost 50% of dogs diagnosed with <strong>Ehrlichia</strong> also harbored<br />
Bartonella vinsonii. Concurrent seropositivity has<br />
also been documented for B. burgdorferi and E. canis. 18<br />
Such simultaneous infections may worsen the severity of<br />
observed disease and impact the out<strong>com</strong>e of treatment.
Compendium April 2002 Ehrlichiosis 279<br />
TRANSMISSION AND PATHOGENESIS<br />
The transmission and pathogenesis of canine ehrlichiosis<br />
are best understood for E. canis infection. E.<br />
canis organisms gain entry via salivary secretions during<br />
the bite of an infected tick. 4 Ticks acquire the organism<br />
during their larval or nymph stage when they feed on<br />
an infected canid. Infection is spread when the tick<br />
feeds again on a new host. Because transovarial transmission<br />
does not occur, the tick vector cannot serve as a<br />
reservoir of disease. 4 Ticks can remain infected for long<br />
periods, however, allowing for disease transmission in<br />
early spring after the infected tick has overwintered.<br />
The course of clinical infection with E. canis is traditionally<br />
divided into three stages, which vary in<br />
length. These stages may be difficult to differentiate<br />
in natural infections. 4,22,23<br />
Acute Phase<br />
The acute phase occurs 1 to 3 weeks after the<br />
infected tick bites a dog. 9 During this phase, the organism<br />
invades leukocytes and divides to form morulae,<br />
which are colonies bound by a vacuolar membrane.<br />
Usually a specific ehrlichial species preferentially<br />
invades either mononuclear or granulocytic leukocytes.<br />
E. canis, E. chaffeensis, and E. risticii invade mononuclear<br />
cells, whereas E. ewingii, E. phagocytophila, and E.<br />
equi invade granulocytic neutrophils or eosinophils<br />
(Table 1). During acute infection, the most consistent<br />
hematologic change is the development of thrombocytopenia.<br />
24 This multifactorial change results from vascular<br />
endothelial inflammation with resulting platelet<br />
consumption, immunologically mediated destruction<br />
of platelets, and splenic sequestration of platelets. 9,24,25<br />
Interestingly, thrombocytopenia seems to be a <strong>com</strong>mon<br />
finding during infection with all species of <strong>Ehrlichia</strong><br />
described thus far. In addition to thrombocytopenia,<br />
thrombocytopathia may ac<strong>com</strong>pany E. canis infection.<br />
26 Hyperglobulinemia during acute E. canis infection<br />
is usually the result of a polyclonal gammopathy,<br />
but the gammopathy does not seem to be caused by<br />
ehrlichial-specific antibody production. 9,27 Few dogs<br />
succumb to the acute disease; most either clear the<br />
organism (likely via cell-mediated immunity) or enter<br />
the subclinical stage of infection. 4,9<br />
Subclinical Phase<br />
The subclinical phase of E. canis infection is characterized<br />
by persistence of the organism in the host in the<br />
absence of clinical illness. It appears likely that organisms<br />
are retained at low numbers in splenic mononuclear<br />
cells during subclinical infection. 28 The length of<br />
the subclinical phase may range from weeks to years; in<br />
fact, it is not known what percentage of subclinically<br />
infected dogs will ever develop clinical illness. In a single<br />
study of naturally infected dogs, 53% demonstrated<br />
positive E. canis antibody titers 4 years after the presumed<br />
time of infection but remained clinically asymptomatic.<br />
Many of these dogs did, however, demonstrate<br />
abnormalities suggestive of ehrlichial disease on <strong>com</strong>plete<br />
blood cell counts (e.g., hyperglobulinemia,<br />
thrombocytopenia). 29 Although subclinical infection is<br />
well documented for E. canis, it is less clear whether<br />
other <strong>Ehrlichia</strong> species also induce persistent but subclinical<br />
infections. In at least one case, 12 E. ewingii<br />
morulae were observed in an asymptomatic dog.<br />
Chronic Stage<br />
The pathogenesis of the chronic stage of E. canis infection<br />
is poorly understood because adequate models are<br />
not available. Not all infected animals progress to the<br />
chronic stage, and the factors that influence progression<br />
are still unknown. Persistent E. canis infection results in<br />
persistent antibody formation (both nonspecific and<br />
ehrlichial directed). 9,30,31 Unfortunately, humoral immunity<br />
to E. canis provides no protection. 4,32 In fact, many of<br />
the manifestations of chronic ehrlichial disease may result<br />
from an exuberant but nonprotective humoral immune<br />
response. 4,9 As in the acute stage, hemorrhagic tendencies<br />
may be related to either thrombocytopenia or thrombocytopathia.<br />
In addition to the mechanisms mentioned<br />
previously, hyperglobulinemia associated with chronic<br />
infection is often more pronounced, and hyperviscosity<br />
syndrome with resultant thrombocytopathy may result. 26<br />
Glomerulonephritis may result from the deposit of antigen–antibody<br />
<strong>com</strong>plexes with resultant inflammatory<br />
damage. 23 Bone marrow hypoplasia has been a classic<br />
finding associated with chronic E. canis infection and<br />
may result in pancytopenia. 3,22,23 Nonregenerative anemia<br />
<strong>com</strong>monly associated with chronic E. canis infection may<br />
be caused by either anemia of inflammatory disease or by<br />
pancytopenia due to bone marrow hypoplasia. 22,23,33 Concurrent<br />
infectious diseases documented in dogs with E.<br />
canis have been attributed to immunosuppressive effects<br />
of chronic infection. 23<br />
CLINICAL FINDINGS<br />
<strong>Ehrlichia</strong> canis<br />
Clinical findings associated with E. canis infection<br />
vary tremendously and are likely influenced by the<br />
strain of organism, host immune status, and breed of<br />
animal. 4,34 German shepherds are classically thought to<br />
be more susceptible to infection and to have a more fulminant<br />
course of infection than dogs of other<br />
breeds. 34–36 By definition, no clinical signs are apparent<br />
during the subclinical phase of infection, although<br />
hematologic abnormalities may be identified. 29 Often,
280 Small Animal/Exotics Compendium April 2002<br />
either the acute stage of infection goes unnoticed or<br />
signs are mild enough that owners do not seek veterinary<br />
care for their pets. When dogs are evaluated during<br />
the acute stage of infection, signs are largely nonspecific<br />
and include lethargy, fever, anorexia, weight loss,<br />
splenomegaly, and generalized lymphadenopathy. 4,37<br />
Most diagnoses of E. canis infection occur during the<br />
chronic stage of infection. As occurs with dogs presented<br />
during the acute stage, the owners of dogs with<br />
chronic ehrlichiosis most <strong>com</strong>monly report nonspecific<br />
signs, such as lethargy, anorexia, and weight loss. 23,34<br />
Signs attributable to bleeding tendencies, including<br />
epistaxis, melena, petechial and/or ecchymotic hemorrhages,<br />
hyphema, retinal hemorrhage, and hematuria,<br />
occur in 25% to 60% of cases. 22,23,33,34 Additional physical<br />
examination findings include lymphadenopathy,<br />
fever, pale mucous membranes, and splenomegaly. 22,23,33,34<br />
Anterior uveitis, retinal changes, or neurologic abnormalities<br />
are noted occasionally. 23,38 Ataxia, paraparesis,<br />
conscious proprioceptive deficits, head tilt, nystagmus,<br />
and seizures have all been reported as neurologic manifestations<br />
of infection. 23 The importance of lameness as<br />
a clinical sign of E. canis infection is debatable.<br />
Although lameness is often listed as a clinical sign of<br />
infection in the older literature, many of the animals<br />
displaying lameness were found to have granulocytic<br />
morulae, suggesting that the infection may have been<br />
caused by E. ewingii rather than E. canis. 39–41 Other clinical<br />
signs of chronic E. canis infection relate to <strong>com</strong>plications,<br />
including glomerulonephritis with nephrotic<br />
syndrome, or pancytopenia resulting in secondary infections<br />
and severe anemia.<br />
Clinicopathologic abnormalities are also nonspecific.<br />
Although normal platelet concentrations do not rule out<br />
chronic ehrlichiosis, most cases display some degree of<br />
thrombocytopenia. 22,23,33,34 Nonregenerative anemia<br />
(often mild to moderate) is also identified in most<br />
cases. 22,23 White blood cell counts may fall below, within,<br />
or above reference ranges in dogs with ehrlichiosis. 22,23,33<br />
Although hyperglobulinemia has not been reported consistently,<br />
it is observed in most cases. 22,23,34 Albeit usually<br />
due to polyclonal gammopathy, hyperglobulinemia may<br />
present as a monoclonal gammopathy that can be easily<br />
mistaken for multiple myeloma. 27,42 Other serum biochemistry<br />
abnormalities noted with some regularity<br />
include hypoalbuminemia, elevated alkaline phosphatase,<br />
and elevated alanine transaminase concentrations.<br />
22,23,33 Proteinuria may occur independently or concurrently<br />
with glomerulonephritis. 22,23,33,43,44 Although<br />
early descriptions of E. canis infection were of a tropical<br />
pancytopenia, the pancytopenic manifestations now<br />
appear to account for a small minority of cases in the<br />
United States. Cytologic evaluation of bone marrow<br />
aspirates often displays increased numbers of plasma<br />
cells, with either hypoplasia (suggesting chronic infection)<br />
or hyperplasia (suggesting acute or chronic infection)<br />
of the other marrow elements. 3,22,23,37<br />
<strong>Ehrlichia</strong> ewingii<br />
E. ewingii is one of two ehrlichial agents known to<br />
result in granulocytic infection in dogs, with the other<br />
agent being E. equi. 12 Unfortunately, identification of<br />
granulocytic morulae does not differentiate E. equi infection<br />
from E. ewingii infection, which likely predominates<br />
in the southern and lower midwestern United<br />
States. Because E. ewingii belongs to the same genogroup<br />
as E. canis, E. canis titers should be positive during infection.<br />
12 Many descriptions of granulocytic ehrlichial infection<br />
are of dogs with acute-onset polyarthritis, and these<br />
cases have more often than not been ascribed to E.<br />
ewingii infection. 5,39–41,45 The lameness may involve more<br />
than one leg or appear to shift from limb to limb. Joint<br />
stiffness and occasional joint swelling due to effusion<br />
may be noted, and dogs are often febrile. Splenomegaly<br />
and hepatomegaly have been reported. Bleeding tendencies<br />
may be noted, and many infected dogs have mild to<br />
moderate thrombocytopenia. 12 Central nervous system<br />
involvement, particularly meningitis, has been<br />
reported. 46 Dual infection with both E. canis and E.<br />
ewingii has also been reported in association with profound<br />
ataxia and epistaxis. 47 Polyarthritis resolves quickly<br />
with appropriate therapy. Fatal granulocytic ehrlichial<br />
infections seem to be extremely rare in dogs.<br />
<strong>Ehrlichia</strong> equi<br />
As with E. ewingii, the true incidence of E. equi infections<br />
in dogs is unknown, but E. equi may account for a<br />
significant proportion of granulocytic ehrlichiosis in the<br />
northeastern and upper midwestern United States and<br />
California, where equine infections are endemic. 7,11,12<br />
Experimental infection with E. equi in dogs produced<br />
only mild to inapparent clinical signs, but naturally<br />
infected dogs have presented with nonspecific illness,<br />
including fever, lethargy, and thrombocytopenia. 11,48<br />
There are no unique clinical findings attributed to infection<br />
with E. equi, but polyarthritis is described less frequently<br />
than for E. ewingii. 11 Without an index of suspicion,<br />
veterinarians may not request the specific diagnostic<br />
testing required to differentiate this ehrlichial infection<br />
from others, and E. canis titers may be negative. 11,12<br />
<strong>Ehrlichia</strong> risticii<br />
E. risticii, the causative agent of Potomac horse fever, can<br />
infect dogs and cats as well as horses. This agent is transmitted<br />
not by a tick bite but rather by ingestion of snails,<br />
perhaps explaining why canine infection is not <strong>com</strong>monly
Compendium April 2002 Ehrlichiosis 281<br />
described. When dogs are infected, lethargy, vomiting,<br />
bleeding disorders, and arthralgia have been reported. 13<br />
Because E. risticii belongs to a different genogroup than E.<br />
canis, antibody cross-reactivity may be lacking. Unless<br />
genogroup-specific titers are requested, dogs with E. risticii<br />
infection may display negative ehrlichial titers. 13<br />
<strong>Ehrlichia</strong> chaffeensis<br />
Although E. chaffeensis is primarily notable as a<br />
human pathogen, dogs are also susceptible to infection<br />
with this organism. Experimentally infected dogs seem<br />
to have mild or inapparent disease. 49 However, a report<br />
of three dogs infected naturally with E. chaffeensis documented<br />
more serious signs, including vomiting, epistaxis,<br />
lymphadenopathy, and anterior uveitis. 6 Because<br />
E. chaffeensis shares genogrouping with E. canis, routine<br />
titers should prove positive in infected dogs. 6<br />
<strong>Ehrlichia</strong> platys<br />
E. platys is unique among the <strong>Ehrlichia</strong> species because<br />
of its predisposition for platelets rather than leukocytes.<br />
E. platys does not share serologic cross-reactivity with E.<br />
canis, but co-infections have been documented. 8,15,50,51<br />
Although infection with E. platys results in cyclic thrombocytopenia<br />
in dogs, it is seldom the cause of clinical<br />
bleeding unless trauma or surgery is performed during<br />
the thrombocytopenic cycle. 52,53 The disease manifestations<br />
associated with E. platys may be more severe in<br />
strains found outside the United States. 54–56 Veterinarians<br />
should consider specific testing for E. platys infection in<br />
dogs with recurring evidence of thrombocytopenia for<br />
which another cause (including the more <strong>com</strong>mon<br />
ehrlichial infections) cannot be documented.<br />
Feline Ehrlichiosis<br />
The topic of feline ehrlichiosis deserves separate mention<br />
from canine ehrlichiosis. 57 Cats have been experimentally<br />
infected with both E. risticii and E. equi, producing<br />
either subclinical infection or mild illness. 48,58 To<br />
date, experimental infection with E. canis or E. ewingii<br />
has not been attempted. Naturally occurring feline ehrlichiosis<br />
has been documented in only 31 cats worldwide.<br />
These cats presented with various clinical signs, including<br />
fever, anorexia, arthropathy, gastrointestinal signs,<br />
and general malaise. 57,59–62 Until a clearer picture of the<br />
importance and clinical presentation of feline ehrlichiosis<br />
is developed, ehrlichiosis should remain a consideration<br />
in cats with various unexplained clinical illnesses. Diagnosis<br />
relies on ruling out other causes for the described<br />
clinical illness in <strong>com</strong>bination with either identification
282 Small Animal/Exotics Compendium April 2002<br />
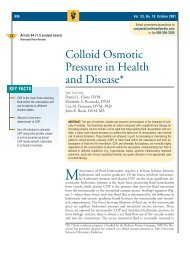
Figure 1—A round, basophilic morula of E. ewingii is seen in<br />
the cytoplasm of the neutrophil. (Courtesy of Steve Stockham,<br />
DVM, MS, Kansas State University.)<br />
of morulae within the peripheral blood cells or serologic<br />
evidence of exposure to an ehrlichial agent as well as resolution<br />
of clinical signs after appropriate antibiotic therapy.<br />
57 Both granulocytic and monocytic infections have<br />
been described, with the expected variations in serologic<br />
reactivity to different ehrlichial agents. 57,60,62<br />
DIAGNOSIS<br />
Ehrlichiosis is usually diagnosed based on clinical<br />
signs, consistent laboratory abnormalities, and<br />
<strong>Ehrlichia</strong>-specific testing. Although observation of<br />
intracellular morulae is diagnostic, the search for morulae<br />
is most often unrewarding. 35 The use of concentration<br />
techniques, such as buffy coat examination with a<br />
Romanovsky-type stain, maximizes the chance of identifying<br />
morulae. 3 Morulae may be observed in white<br />
blood cells from peripheral blood or other fluids,<br />
including cerebrospinal and joint fluids. 39,40,46,47 In general,<br />
morulae are more readily apparent during the<br />
acute phase of monocytic E. canis infection or during<br />
infection with the granulocytic species E. ewingii and<br />
E. equi (Figure 1). 5,11,23,35<br />
The most <strong>com</strong>monly employed diagnostic test for<br />
suspected ehrlichial infection is indirect fluorescent<br />
antibody (IFA) serology. This form of testing does not<br />
detect the actual ehrlichial organism but rather<br />
ehrlichial-reactive antibody in the serum. Veterinarians<br />
employing IFA testing must understand that a positive<br />
titer in a dog from an endemic area does not confirm<br />
that the disease under investigation is caused by<br />
ehrlichial infection. Rather, a positive titer confirms<br />
exposure to the organism but may be observed after<br />
exposure and clearance of the organism, during the<br />
subclinical stage, or after successful treatment, as well as<br />
during active infection. Likewise, a negative titer does<br />
not rule out infection. Moribund animals may cease to<br />
produce antibody, resulting in a diminished or negative<br />
titer, and acutely infected dogs require 7 to 21 days for<br />
seroconversion, potentially resulting in negative titers<br />
in infected dogs. 63 Depending on the particular IFA test<br />
used, serology can be more or less specific for a species<br />
of <strong>Ehrlichia</strong>. Antibody generated to one species of<br />
<strong>Ehrlichia</strong> may cross-react with other species. Species<br />
that fall within the same genogroup are likely to possess<br />
serologic cross-reactivity. Likewise, titers to one<br />
genogroup may be negative during infection with<br />
members of a different genogroup (i.e., E. canis titers<br />
may be negative during infection with E. equi). Currently,<br />
titers are <strong>com</strong>mercially available for members of<br />
each genogroup, including E. canis, E. equi, E. risticii,<br />
and E. platys. a<br />
Polymerase chain reaction (PCR) detects actual DNA<br />
from the ehrlichial organism. Primers are chosen to<br />
amplify a portion of the bacterial DNA, allowing detection<br />
of that genetic material. The use of generic<br />
ehrlichial primers allows detection of any of several<br />
species of <strong>Ehrlichia</strong> using one test. Alternatively, by<br />
using primers directed at a specific, highly variable portion<br />
of the bacterial gene, PCR can identify the specific<br />
species of <strong>Ehrlichia</strong> in an affected animal. Such primers<br />
are currently available for E. canis, E. ewingii, E. equi,<br />
E. chaffeensis, E. risticii, and E. platys. 6 Many <strong>com</strong>mercial<br />
laboratories use generic primers and then may or<br />
may not speciate positive samples. b,c Although PCR can<br />
be a sensitive test, the choice of sample will influence<br />
results. Most <strong>com</strong>mercial laboratories that perform<br />
PCR request whole blood samples, but organisms<br />
might at times be sequestered in low numbers in such<br />
tissues as the spleen or bone marrow. 64 PCR may be<br />
used occasionally in conjunction with IFA to differentiate<br />
between exposure to <strong>Ehrlichia</strong> and true infection<br />
(such as after <strong>com</strong>pletion of treatment and in the presence<br />
of continued clinical signs and persistent ehrlichial<br />
titers). 65 The laboratory’s quality control is crucial for<br />
reliable PCR results.<br />
A <strong>com</strong>mercial in-house screening kit that tests for B.<br />
burgdorferi antibody d has been marketed. Screening<br />
ELISA tests of this kind are designed to produce a positive<br />
response in animals with an antibody titer corresponding<br />
to an IFA titer of greater than 1:500.<br />
Reported sensitivity and specificity of these test kits are<br />
98.9% and greater than 99%, respectively. As with any<br />
test, predictive value is more important than either sensitivity<br />
or specificity, but it depends on both as well as<br />
a ProtaTek International, Inc., Chandler, AZ.<br />
b Antech Diagnostics, Irvine, CA.<br />
c Tick-borne disease testing facility, College of Veterinary Medicine,<br />
North Carolina State University, Raleigh, NC.<br />
d Snap ® 3Dx Test, IDEXX Laboratories, Inc., Westbrook, ME.
Compendium April 2002 Ehrlichiosis 283<br />
on the prevalence of the disease in question. Thus a<br />
positive screening test in an endemic area is more likely<br />
to be a true positive than is the same result in an area<br />
with a lesser disease prevalence. As is true of the IFA<br />
test, a positive titer must be interpreted with caution<br />
because it may represent current or resolved infection<br />
or merely exposure.<br />
TREATMENT<br />
Tetracycline-related antibiotics have been the treatment<br />
of choice for ehrlichial infections for years. 3<br />
Excellent absorption and an infrequent dosing interval<br />
make doxycycline the preferred drug. 32,66 Although a 7to<br />
14-day course of doxycycline at 10 mg/kg/day has<br />
been previously re<strong>com</strong>mended, 4,6,32 this length of treatment<br />
may be inadequate. 66,67 In fact, in a study of subclinically<br />
infected dogs treated with doxycycline for 6<br />
weeks, ehrlichial organisms could still be identified by<br />
PCR in one of four dogs. 67 Although the appropriate<br />
length of treatment has not been clearly determined,<br />
treatment for dogs with chronic infection may be quite<br />
long in duration and titers may remain elevated for<br />
months to years, regardless of the treatment length.<br />
Even long courses of treatment (average, 210 days) did<br />
not produce negative titers in a significant proportion<br />
of naturally infected dogs. 30 Although most studies have<br />
been directed at E. canis infections, doxycycline has<br />
proven effective for E. equi and E. ewingii infections<br />
but less effective for E. chaffeensis. 6,12,32<br />
Imidocarb dipropionate, only recently available in<br />
the United States, has also been used successfully to<br />
treat canine ehrlichiosis. Although a study in 1980<br />
found that imidocarb produced more effective clearance<br />
of E. canis than did a 2-week course of tetracycline,<br />
recent studies using doxycycline have documented<br />
no difference in the clinical response of dogs<br />
treated with either drug alone or with both drugs<br />
simultaneously. 68,69 Imidocarb is administered at 5<br />
mg/kg IM, with a second injection 2 weeks after the<br />
first. 4,69 Pretreatment with atropine may lessen the<br />
occurrence of unpleasant anticholinergic side effects,<br />
including salivation, serous nasal discharge, diarrhea,<br />
and dyspnea.<br />
Other antibacterial agents have also been evaluated<br />
for the treatment of ehrlichial infections. Chloramphenicol<br />
may be used in puppies to avoid the discoloration<br />
of erupting teeth associated with tetracycline. 4<br />
Quinolones cannot be re<strong>com</strong>mended currently as a<br />
treatment for ehrlichiosis. Although enrofloxacin has<br />
been used successfully to treat experimental Rickettsia
284 Small Animal/Exotics Compendium April 2002<br />
rickettsii infection in dogs, it does not seem an effective<br />
treatment for E. canis. Most dogs with experimental E.<br />
canis infections that were administered dosages of 10<br />
mg/kg PO q12h for 21 days remained thrombocytopenic<br />
and blood culture positive. 32 Similarly,<br />
ciprofloxacin was unsuccessful in eliminating infection<br />
with E. chaffeensis in humans. 70<br />
In addition to antibiotics, other supportive therapies<br />
may be required during ehrlichial infection. Glucocorticosteroids<br />
can attenuate the immune-mediated<br />
destruction of platelets associated with infection, and<br />
thus a short course (2 to 7 days) of prednisone may be<br />
indicated if thrombocytopenia is severe or pending<br />
diagnostic testing to differentiate ehrlichiosis from<br />
immune-mediated thrombocytopenia. 4,23 Steroids may<br />
also be indicated for the treatment of polyarthritis, vasculitis,<br />
or meningitis associated with certain types of<br />
ehrlichial infections. 4,46,47 Other supportive treatments<br />
might include the administration of parenteral crystalloid<br />
or colloidal fluids or blood transfusion, as indicated.<br />
3,4 Complications of chronic E. canis infection<br />
(e.g., glomerulonephritis, pancytopenia) may likewise<br />
require specific supportive therapy.<br />
EVALUATING TREATMENT<br />
Evaluation of treatment remains problematic. Resolution<br />
of clinical signs and normalization of platelet<br />
counts are usually noted within days of initiating<br />
proper treatment for acute cases and often for mild<br />
chronic cases as well. 4,23,69 Even after rapid clinical<br />
improvement, studies have found that platelet counts<br />
may again decrease after <strong>com</strong>pletion of doxycycline<br />
therapy, titers remain elevated, organisms can still be<br />
cultured, and PCR results remain positive. 64,69 Serum<br />
antibody titers can remain elevated for months to years<br />
after appropriate treatment in dogs that remain clinically<br />
and hematologically normal. 30,31,64,69 These persistently<br />
positive titers, which tend to correlate with the<br />
highest initial titers, may indicate continued infection<br />
or re-infection or may be indicative of a past infection<br />
only. 23,30 PCR may offer the best option for documenting<br />
clearance of the organisms after therapy, but even<br />
PCR evaluation can be problematic. PCR detects bacterial<br />
DNA but cannot distinguish between living and<br />
nonliving organisms. However, it is unlikely that killed<br />
ehrlichial organisms would persist in the body for<br />
more than several weeks, rendering a positive PCR<br />
result strongly suggestive of active infection. The<br />
greater problem is related to false-negative results when<br />
sampling tissues that contain low levels of organisms<br />
(e.g., blood, bone marrow). 64,65 Practically speaking,<br />
treated dogs for which the clinical and laboratory evidence<br />
of disease is resolved need not be further evalu-<br />
ated for the presence of organisms. In animals treated<br />
appropriately for infection but in which evidence of<br />
disease remains, a positive PCR would warrant continuation<br />
or alteration of therapy, while a negative PCR<br />
should prompt consideration that the observed disease<br />
may not be due to ehrlichiosis.<br />
PREVENTION AND CONTROL<br />
Unfortunately, exposure to E. canis does not confer<br />
protective immunity. Effective tick control is the most<br />
important preventive measure for infection or re-infection.<br />
Several highly efficacious products are available<br />
for direct application to dogs, including Frontline ® Top<br />
Spot (Merial Ltd, Iselin, NJ), Preventic ® collars (Virbac,<br />
Inc., Fort Worth, TX), and Kiltix ® Topical Tick<br />
Control for Dogs (Bayer Animal Health, Shawnee Mission,<br />
KS). In addition, many premise sprays are available<br />
to decrease tick populations in the dog’s local environment.<br />
The prophylactic use of tetracycline<br />
antibiotics during tick season has also been advocated<br />
for prevention of infection, but this option is not free<br />
from either the cost or risk associated with antibiotic<br />
use. 4 To prevent disease associated with chronic E. canis<br />
infection, it has been suggested that dogs in endemic<br />
areas be serologically monitored and positive animals<br />
treated regardless of the presence of clinical signs. 4 We<br />
suggest that a positive screening test (e.g., ELISA) be<br />
used as evidence that further evaluation is needed. At a<br />
minimum, such evaluation should include a thorough<br />
physical examination, quantitative platelet count, and<br />
measurement of serum globulin. Positive screening tests<br />
might also prompt confirmatory tests, including either<br />
IFA or PCR, prior to initiation of antibiotic therapy.<br />
ZOONOTIC POTENTIAL<br />
Since the first description of human monocytic ehrlichiosis<br />
(HME) in the United States in 1986, 71 the disease<br />
has garnered both scientific and public attention.<br />
The agent of HME, which shares a penchant for<br />
monocytic cell infection and produces antibodies crossreactive<br />
to E. canis, was named E. chaffeensis. 72 E. chaffeensis<br />
infection in dogs has been identified in both<br />
experimental and natural settings, with the organism<br />
persisting for months. 6,49 These long-lasting infections<br />
raise the concern that dogs may serve as a reservoir of<br />
infection for human disease. 72 Adding to those concerns,<br />
it seems that doxycycline may not easily clear the<br />
organism from naturally infected dogs. 6 In addition to<br />
HME, HGE has been recognized as well. The causative<br />
agent of HGE, which differs from that of HME, has<br />
proven to be nearly identical to E. phagocytophila and<br />
E. equi. Although these agents are most <strong>com</strong>monly<br />
associated with infection in small ruminants and/or
Compendium April 2002 Ehrlichiosis 285<br />
horses, respectively, both organisms have been isolated<br />
from dogs, again raising the possibility that dogs may<br />
serve as a reservoir for human infection. 8,11,73,74 Additionally,<br />
the <strong>com</strong>mon agents of canine ehrilichiosis, E.<br />
canis, and E. ewingii can occasionally cause clinical disease<br />
in humans. 75 The symptoms of HME and HGE<br />
are quite similar and include fever, headache, and myalgia.<br />
Left untreated, either infection may prove fatal to<br />
humans. 8,71,72,76<br />
CONCLUSION<br />
Ehrlichiosis is a bacterial infection transmitted largely<br />
through the bite of infected ticks. Dogs with ehrlichiosis<br />
can no longer be assumed to have an E. canis infection<br />
alone. Veterinarians should be aware of the similarities<br />
and differences between E. canis and other arthropodborne<br />
infections. Dogs with suggestive clinical signs and<br />
laboratory abnormalities may be started on doxycycline<br />
pending specific diagnostic testing. Veterinarians practicing<br />
in endemic areas are confronted with the often<br />
difficult task of sorting out ehrlichial infection from<br />
mere exposure. Once a diagnosis is established, treatment<br />
should continue for at least 3 weeks. Tick prevention<br />
for animals in endemic areas should be maintained<br />
throughout tick season, not only to prevent disease but<br />
also to lessen the potential for dogs to be<strong>com</strong>e carriers of<br />
disease for their human <strong>com</strong>panions.<br />
REFERENCES<br />
1. Donatien A, Lestoquard F: Existence en Algerie d’une Rickettsia<br />
du chien. Bull Soc Pathol Exot 28:418–419, 1935.<br />
2. Keefe TJ, Holland CJ, Salyer PE, Ristic M: Distribution of<br />
<strong>Ehrlichia</strong> canis among military working dogs in the world and<br />
selected civilian dogs in the United States. JAVMA 181:236–238,<br />
1982.<br />
3. Huxsoll DL, Hildebrandt PK, Nims RM, Walker JS: Tropical<br />
canine pancytopenia. JAVMA 157:1627–1632, 1970.<br />
4. Neer TM: Ehrlichiosis: Canine monocytic and granulocytic<br />
ehrlichiosis, in Greene GE (ed): Infectious Diseases of the Dog<br />
and Cat, ed 2. Philadelphia, WB Saunders Co, 1998, pp<br />
139–149.<br />
5. Stockham SL, Schmidt DA, Curtis KS, et al: Evaluation of granulocytic<br />
ehrlichiosis in dogs of Missouri, including serologic status<br />
to <strong>Ehrlichia</strong> canis, <strong>Ehrlichia</strong> equi and Borrelia burgdorferi. Am<br />
J Vet Res 53:63–68, 1992.<br />
6. Breitschwerdt EB, Hegarty BC, Hancock SI: Sequential evaluation<br />
of dogs naturally infected with <strong>Ehrlichia</strong> canis, <strong>Ehrlichia</strong><br />
chaffeensis, <strong>Ehrlichia</strong> equi, <strong>Ehrlichia</strong> ewingii, or Bartonella vinsonii.<br />
J Clin Microbiol 36:2645–2651, 1998.<br />
7. Magnarelli LA, Ijdo JW, Anderson JF, et al: Antibodies to<br />
<strong>Ehrlichia</strong> equi in dogs from the northeastern United States.<br />
JAVMA 211:1134–1137, 1997.<br />
8. Dumler JS, Bakken JS: <strong>Ehrlichia</strong>l diseases of humans: Emerging
286 Small Animal/Exotics Compendium April 2002<br />
tick-borne infections. Clin Infect Dis 20:1102–1110, 1995.<br />
9. Harrus S, Waner T, Bark H, et al: Recent advances in determining<br />
the pathogenesis of canine monocytic ehrlichiosis. J Clin<br />
Microbiol 37:2745–2749, 1999.<br />
10. Murphy GL, Ewing SA, Whitworth LC, et al: A molecular and<br />
serologic survey of <strong>Ehrlichia</strong> canis, E. chaffeensis, and E. ewingii in<br />
dogs and ticks from Oklahoma. Vet Parasitol 79:325–339, 1998.<br />
11. Greig B, Asanovich KM, Armstrong PJ, Dumler JS: Geographic,<br />
clinical, serologic, and molecular evidence of granulocytic ehrlichiosis,<br />
a likely zoonotic disease, in Minnesota and Wisconsin<br />
dogs. J Clin Microbiol 34:44–48, 1996.<br />
12. Goldman EE, Breitschwerdt EB, Grindem CB, et al: Granulocytic<br />
ehrlichiosis in dogs from North Carolina and Virginia. J<br />
Vet Intern Med 12:61–70, 1998.<br />
13. Kakoma I, Hansen RD, Anderson BE, et al: Cultural, molecular,<br />
and immunological characterization of the etiologic agent for<br />
atypical canine ehrlichiosis. J Clin Microbiol 32:170–175, 1994.<br />
14. Pretzman C, Ralph D, Stothard DR, et al: 16S rRNA gene<br />
sequence of Neorickettsia helminthoeca and its phylogenetic<br />
alignment with members of the genus <strong>Ehrlichia</strong>. Int J Syst Bacteriol<br />
45:207–211, 1995.<br />
15. Kordick SK, Breitschwerdt EB, Hegarty BC, et al: Coinfection<br />
with multiple tick-borne pathogens in a Walker Hound kennel<br />
in North Carolina. J Clin Microbiol 37:2631–2638, 1999.<br />
16. Matthewman LA, Kelly PJ, Bobade PA, et al: Infections with<br />
Babesia canis and <strong>Ehrlichia</strong> canis in dogs in Zimbabwe. Vet Rec<br />
133:344–346, 1993.<br />
17. du Plessis JL, Fourie N, Nel PW, Evezard DN: Concurrent<br />
babesiosis and ehrlichiosis in the dog: Blood smear examination<br />
supplemented by the indirect fluorescent antibody test, using<br />
Cowdria ruminantium as antigen. Onderstepoort J Vet Res 57:<br />
151–155, 1990.<br />
18. Magnarelli LA, Anderson JF: Serologic evidence of canine and<br />
equine ehrlichiosis in northeastern United States. J Clin Microbiol<br />
31:2857–2860, 1993.<br />
19. Pancholi P, Kolbert CP, Mitchell PD, et al: Ixodes dammini as a<br />
potential vector of human granulocytic ehrlichiosis. J Infect Dis<br />
172:1007–1012, 1995.<br />
20. Mitchell PD, Reed KD, Hofkes JM: Immunoserologic evidence<br />
of coinfection with Borrelia burgdorferi, Babesia microti, and<br />
human granulocytic <strong>Ehrlichia</strong> species in residents of Wisconsin<br />
and Minnesota. J Clin Microbiol 34:724–727, 1996.<br />
21. Dumler JS, Asanovich KM, Bakken JS, et al: Serologic cross-reactions<br />
among <strong>Ehrlichia</strong> equi, <strong>Ehrlichia</strong> phagocytophila, and human<br />
granulocytic <strong>Ehrlichia</strong>. J Clin Microbiol 33:1098–1103, 1995.<br />
22. Waddle JR, Littman MP: A retrospective study of 27 cases of naturally<br />
occurring canine ehrlichiosis. JAAHA 24:615–620, 1988.<br />
23. Frank JR, Breitschwerdt EB: A retrospective study of ehrlichiosis<br />
in 62 dogs from North Carolina and Virginia. J Vet Intern Med<br />
13:194–201, 1999.<br />
24. Warner T, Harrus S, Weiss DJ, et al: Demonstration of serum<br />
antiplatelet antibodies in experimental acute canine ehrlichiosis.<br />
Vet Immunol Immunopathol 48:177–182, 1995.<br />
25. Grindem CB, Breitschwerdt EB, Perkins PC, et al: Platelet-associated<br />
immunoglobulin (antiplatelet antibody) in canine Rocky<br />
Mountain spotted fever and ehrlichiosis. JAAHA 35:56–61, 1999.<br />
26. Harrus S, Waner T, Eldor A, et al: Platelet dysfunction associated<br />
with experimental acute canine ehrlichiosis. Vet Rec<br />
139:290–293, 1996.<br />
27. Harrus S, Waner T, Avidar Y, et al: Serum protein alteration in<br />
canine ehrlichiosis. Vet Parasitol 66:241–249, 1996.<br />
28. Harrus S, Waner T, Keysary A, et al: Investigation of splenic<br />
functions in canine monocytic ehrlichiosis. Vet Immunol<br />
Immunopathol 62:15–27, 1998.<br />
29. Codner EC, Farris-Smith LL: Characterization of the subclinical<br />
phase of ehrlichiosis in dogs. JAVMA 189:47–50, 1986.<br />
30. Bartsch RC, Greene RT: Post-therapy antibody titers in dogs<br />
with ehrlichiosis: Follow-up study on 68 patients treated primarily<br />
with tetracycline and/or doxycycline. J Vet Intern Med<br />
10:271–274, 1996.<br />
31. Perille AL, Matus RE: Canine ehrlichiosis in six dogs with persistently<br />
increased antibody titers. J Vet Intern Med 5:195–198, 1991.<br />
32. Breitschwerdt EB, Hegarty BC, Hancock SI: Doxycycline<br />
hyclate treatment of experimental canine ehrlichiosis followed<br />
by challenge inoculation with two <strong>Ehrlichia</strong> canis strains.<br />
Antimicrob Agents Chemother 42:362–368, 1998.<br />
33. Troy GC, Vulgamott JC, Turnwald GH: Canine ehrlichiosis: A<br />
retrospective study of 30 naturally occurring cases. JAAHA 16:<br />
181–187, 1980.<br />
34. Harrus S, Kass PH, Klement E, Waner T: Canine monocytic<br />
ehrlichiosis: A retrospective study of 100 cases, and an epidemiological<br />
investigation of prognostic indicators for the disease.<br />
Vet Rec 141:360–363, 1997.<br />
35. Elias E: Diagnosis of ehrlichiosis from the presence of inclusion<br />
bodies or morulae of E. canis. J Small Anim Pract 33:540–543,<br />
1991.<br />
36. Nyindo M, Huxsoll DL, Ristic M, et al: Cell-mediated and<br />
humoral immune responses of German shepherd dogs and beagles<br />
to experimental infection with <strong>Ehrlichia</strong> canis. Am J Vet Res<br />
41:250–254, 1980.<br />
37. Buhles Jr WC, Huxsoll DL, Ristic M: Tropical canine pancytopenia:<br />
Clinical, hematologic, and serologic response of dogs to<br />
<strong>Ehrlichia</strong> canis infection, tetracycline therapy, and challenge<br />
inoculation. J Infect Dis 130:357–367, 1974.<br />
38. Panciera RJ, Ewing SA, Confer AW: Ocular histopathology of<br />
ehrlichial infections in the dog. Vet Pathol 38:43–46, 2001.<br />
39. Cowell RL, Tyler RD, Clinkenbeard KD, Meinkoth JH: Ehrlichiosis<br />
and polyarthritis in three dogs. JAVMA 192:1093–1095, 1988.<br />
40. Bellah JR, Shull RM, Selcer EV: <strong>Ehrlichia</strong> canis-related polyarthritis<br />
in a dog. JAVMA 189:922–923, 1986.<br />
41. Stockham SL, Schmidt DA, Tyler JW: Canine granulocytic<br />
ehrlichiosis in dogs from central Missouri, a possible cause of<br />
polyarthritis. Vet Med Rev 6:63–65, 1985.<br />
42. Breitschwerdt EB, Woody BJ, Zerbe CA, et al: Monoclonal<br />
gammopathy associated with naturally occurring canine ehrlichiosis.<br />
J Vet Intern Med 1:2–9, 1987.<br />
43. Codner EC, Maslin WR: Investigation of renal protein loss in<br />
dogs with acute experimentally induced <strong>Ehrlichia</strong> canis infection.<br />
Am J Vet Res 53:294–299, 1992.<br />
44. Varela F, Font X, Valladares JE, Alberola J: Thrombocytopathia<br />
and light-chain proteinuria in a dog naturally infected with<br />
<strong>Ehrlichia</strong> canis. J Vet Intern Med 11:309–311, 1997.<br />
45. Anderson BE, Greene CE, Jones DC, Dawson JE: <strong>Ehrlichia</strong><br />
ewingii sp. nov., the etiologic agent of canine granulocytic ehrlichiosis.<br />
Int J Syst Bacteriol 42:299–302, 1992.<br />
46. Maretzki CH, Fisher DJ, Greene CE: Granulocytic ehrlichiosis<br />
and meningitis in a dog. JAVMA 205:1554–1556, 1994.<br />
47. Meinkoth JH, Ewing SA, Cowell RL, et al: Morphologic and<br />
molecular evidence of a dual species ehrlichial infection in a dog<br />
presenting with inflammatory central nervous system disease. J<br />
Vet Intern Med 12:389–393, 1998.<br />
48. Lewis GE, Huxsoll DL, Ristic M, Johnson AJ: Experimentally
Compendium April 2002 Ehrlichiosis 287<br />
induced infection of dogs, cats, and nonhuman primates with<br />
<strong>Ehrlichia</strong> equi, etiologic agent of equine ehrlichiosis. Am J Vet<br />
Res 36:85–88, 1975.<br />
49. Dawson JE, Ewing SA: Susceptibility of dogs to infection with<br />
<strong>Ehrlichia</strong> chaffeensis, causative agent of human ehrlichiosis. Am J<br />
Vet Res 53:1322–1327, 1992.<br />
50. Suksawat J, Pitulle C, Arraga-Alvarado C, et al: Coinfection<br />
with three <strong>Ehrlichia</strong> species in dogs from Thailand and<br />
Venezuela with emphasis on consideration of 16S ribosomal<br />
DNA secondary structure. J Clin Microbiol 39:90–93, 2001.<br />
51. Hua P, Yuhai M, Shide T, et al: Canine ehrlichiosis caused<br />
simultaneously by <strong>Ehrlichia</strong> canis and <strong>Ehrlichia</strong> platys. Microbiol<br />
Immunol 44:737–739, 2000.<br />
52. Mathew JS, Ewing SA, Murphy GL, et al: Characterization of a<br />
new isolate of <strong>Ehrlichia</strong> platys (Order Rickettsiales) using electron<br />
microscopy and polymerase chain reaction. Vet Parasitol<br />
68:1–10, 1997.<br />
53. Bradfield JF, Vore SJ, Pryor Jr WH: <strong>Ehrlichia</strong> platys infection in<br />
dogs. Lab Anim Sci 46:565–568, 1996.<br />
54. Harrus S, Aroch I, Lavy E, Bark H: Clinical manifestations of infectious<br />
canine cyclic thrombocytopenia. Vet Rec 141:247–250, 1997.<br />
55. Kontos VI, Papadopoulos O, French TW: Natural and experimental<br />
canine infections with a Greek strain of <strong>Ehrlichia</strong> platys.<br />
Vet Clin Pathol 20:101–105, 1991.<br />
56. Sainz A, Amusategui I, Tesouro MA: <strong>Ehrlichia</strong> platys infection<br />
and disease in dogs in Spain. J Vet Diag Invest 11:382–384, 1999.<br />
57. Stubbs CJ, Holland CJ, Relf JS, et al: Feline ehrlichiosis. Compend<br />
Contin Educ Pract Vet 22(4):307–318, 2000.<br />
58. Dawson JE, Abeygunawardena I, Holland CJ, et al: Susceptibility<br />
of cats to infection with <strong>Ehrlichia</strong> risticii, causative agent of equine<br />
monocytic ehrlichiosis. Am J Vet Res 49:2096–2100, 1988.<br />
59. Peavy GM, Holland CJ, Dutta SK, et al: Suspected ehrlichial infection<br />
in five cats from a household. JAVMA 210:231–234, 1997.<br />
60. Buoro IB, Atwell RB, Kiptoon JC, Ihiga MA: Feline anaemia<br />
associated with <strong>Ehrlichia</strong>-like bodies in three domestic shorthaired<br />
cats. Vet Rec 125:434–436, 1989.<br />
61. Bouloy RP, Lappin MR, Holland CH, et al: Clinical ehrlichiosis<br />
in a cat. JAVMA 204:1475–1478, 1994.<br />
62. Bjoersdorff A, Svendenius L, Owens JH, Massung RF: Feline<br />
granulocytic ehrlichiosis—A report of a new clinical entity and<br />
characterization of the infectious agent. J Small Anim Pract<br />
40:20–24, 1999.<br />
63. Weisiger RM, Ristic M, Huxsoll DL: Kinetics of antibody<br />
response to <strong>Ehrlichia</strong> canis assayed by the indirect fluorescent<br />
antibody method. Am J Vet Res 36:689–694, 1975.<br />
64. Harrus S, Waner T, Aizenberg I, et al: Amplification of ehrlichial<br />
DNA from dogs 34 months after infection with <strong>Ehrlichia</strong> canis.<br />
J Clin Microbiol 36:73–76, 1998.<br />
65. Wen B, Rikihisa Y, Mott JM, et al: Comparison of nested PCR<br />
with immunofluorescent-antibody assay for detection of<br />
<strong>Ehrlichia</strong> canis infection in dogs treated with doxycycline. J Clin<br />
Microbiol 35:1852–1855, 1997.<br />
66. Iqbal Z, Rikihisa Y: Reisolation of <strong>Ehrlichia</strong> canis from blood<br />
and tissues of dogs after doxycycline treatment. J Clin Microbiol<br />
32:1644–1649, 1994.<br />
67. Harrus S, Waner T, Aizenberg I, Bark H: Therapeutic effect of<br />
doxycycline in experimental subclinical canine monocytic ehrlichiosis:<br />
Evaluation of a 6-week course. J Clin Microbiol<br />
36:2140–2142, 1998.
288 Small Animal/Exotics Compendium April 2002<br />
68. Price JE, Dolan TT: A <strong>com</strong>parison of the efficacy of imidocarb dipropionate and tetracycline<br />
hydrochloride in the treatment of canine ehrlichiosis. Vet Rec 107:275–277, 1980.<br />
69. Sainz A, Tesouro MA, Amusategui I, et al: Prospective <strong>com</strong>parative study of 3 treatment<br />
protocols using doxycycline or imidocarb dipropionate in dogs with naturally occurring<br />
ehrlichiosis. J Vet Intern Med 14:134–139, 2000.<br />
70. Brouqui P, Raoult D: In vitro antibiotic susceptibility of the newly recognized agent of<br />
ehrlichiosis in humans, <strong>Ehrlichia</strong> chaffeensis. Antimicrob Agents Chemother 36:2799–2803,<br />
1992.<br />
71. Maeda K, Markowitz N, Hawley RC, et al: Human infection with <strong>Ehrlichia</strong> canis, a leukocytic<br />
rickettsia. N Engl J Med 316:853–856, 1987.<br />
72. Dawson JE, Anderson BE, Fishbein DB, et al: Isolation and characterization of an <strong>Ehrlichia</strong><br />
sp. from a patient diagnosed with human ehrlichiosis. J Clin Microbiol 29:2741–2745,<br />
1991.<br />
73. Chen SM, Dumler JS, Bakken JS, Walker DH: Identification of a granulocytotropic<br />
<strong>Ehrlichia</strong> species as the etiologic agent of human disease. J Clin Microbiol 32:589–595,<br />
1994.<br />
74. Bakken JS, Dumler JS, Chen SM, et al: Human granulocytic ehrlichiosis in the upper midwest<br />
United States. A new species emerging? JAMA 272:212–218, 1994.<br />
75. Buller RS, Arens M, Hmiel SP, et al: <strong>Ehrlichia</strong> ewingii, a newly recognized agent of human<br />
ehrlichiosis. N Engl J Med 341:148–155, 1999.<br />
76. Bakken JS, Krueth J, Wilson-Nordskog C, et al: Clinical and laboratory characteristics of<br />
human granulocytic ehrlichiosis. JAMA 275:199–205, 1996.<br />
ARTICLE<br />
CE<br />
#1 CE TEST<br />
The article you have read qualifies for 1.5 contact hours of Continuing<br />
Education Credit from the Auburn University College of Veterinary<br />
Medicine. Choose the best answer to each of the following questions; then<br />
mark your answers on the postage-paid envelope inserted in Copendium.<br />
1. <strong>Ehrlichia</strong>l organisms are best classified by the<br />
a. type of tick involved in transmission.<br />
b. type of host cell infected.<br />
c. genetic analysis of the 16S rRNA segment.<br />
d. species of host animal infected.<br />
2. Which is the primary transmission vector for E. canis?<br />
a. D. variabilis c. A. americanum<br />
b. R. sanguineus d. Ixodes scapularis<br />
3. Which statement regarding transmission of ehrlichiosis by ticks is true?<br />
a. Ticks can infect dogs only in the fall.<br />
b. Ticks serve as the reservoir for ehrlichial organisms.<br />
c. The ehrlichial organism is passed transovarially prior to infection of dogs.<br />
d. Ticks transmit the infection through salivary secretions released during a bite.<br />
4. What are the most <strong>com</strong>mon presenting <strong>com</strong>plaints in ehrlichiosis?<br />
a. lethargy, fever, and weight loss<br />
b. epistaxis and fever<br />
c. lameness and lethargy<br />
d. secondary infections<br />
5. Which <strong>Ehrlichia</strong> species most <strong>com</strong>monly causes lameness?<br />
a. E. canis c. E. equi<br />
b. E. chaffeensis d. E. ewingii
Compendium April 2002 Ehrlichiosis 289<br />
6. A positive E. canis titer in an asymptomatic dog in an<br />
endemic area indicates that the dog has<br />
a. been exposed and has produced antibodies.<br />
b. entered the subclinical phase of infection.<br />
c. been infected in the past but has cleared the organisms.<br />
d. any of the above<br />
7. Infection with _________ is the most likely explanation<br />
for observed granulocytic morulae and a negative<br />
E. canis titer.<br />
a. E. ewingii c. E. equi<br />
b. E. platys d. E. chaffeensis<br />
8. Six months after treating an infected dog with doxycycline,<br />
a positive E. canis IFA titer can reveal<br />
a. persistence of the titer despite elimination of the<br />
organisms.<br />
b. persistence of the organism.<br />
c. re-infection with organisms.<br />
d. any of the above<br />
9. Administration of ______________ for _______ days<br />
is the re<strong>com</strong>mended treatment protocol for chronic<br />
ehrlichiosis.<br />
a. doxycycline; 21 c. doxycycline; 7 to 10<br />
b. tetracycline; 7 to 10 d. enrofloxacin; 21<br />
10. ___________ has not been reported to infect humans.<br />
a. E. chaffeensis c. E. equi<br />
b. E. ewingii d. E. platys