Emotional response to sport concussion compared to ACL injury
Emotional response to sport concussion compared to ACL injury
Emotional response to sport concussion compared to ACL injury

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
Brain Injury, April 2010; 24(4): 589–597<br />
<strong>Emotional</strong> <strong>response</strong> <strong>to</strong> <strong>sport</strong> <strong>concussion</strong> <strong>compared</strong> <strong>to</strong> <strong>ACL</strong> <strong>injury</strong><br />
LYNDA M. MAINWARING 1 , MICHAEL HUTCHISON 1 , SEAN M. BISSCHOP 2 ,<br />
PAUL COMPER 2 , & DOUG W. RICHARDS 1<br />
1 University of Toron<strong>to</strong>, Faculty of Physical and Health Education, Toron<strong>to</strong>, ON, Canada and<br />
2 Toron<strong>to</strong> Rehabilitation Institute, Toron<strong>to</strong>, ON, Canada<br />
(Received 23 February 2009; revised 21 December 2009; accepted 10 January 2010)<br />
Abstract<br />
Primary objectives: To ascertain and compare the nature of emotional <strong>response</strong> of athletes <strong>to</strong> <strong>concussion</strong> and <strong>to</strong> anterior<br />
cruciate ligament (<strong>ACL</strong>) <strong>injury</strong>.<br />
Research design: Pre-<strong>injury</strong>, post-<strong>injury</strong> and longitudinal emotional functioning of athletes with <strong>concussion</strong> (n ¼ 16),<br />
athletes with <strong>ACL</strong> injuries (n ¼ 7) and uninjured athletes (n ¼ 28) were <strong>compared</strong> in a prospective repeated-measures<br />
design.<br />
Methods and procedures: Participants completed the short version of the Profile of Mood States (POMS). ANOVAs and trend<br />
analysis were used <strong>to</strong> examine between and within group differences across time on two sub-scales, Total Mood<br />
Disturbance and Depression.<br />
Main outcomes and results: Athletes with <strong>ACL</strong> <strong>injury</strong> reported higher levels of depression for a longer duration than athletes<br />
with <strong>concussion</strong>. Relative <strong>to</strong> un-injured controls, athletes with <strong>concussion</strong> reported significant changes in Total Mood<br />
Disturbance and Depression post-<strong>injury</strong>, whereas athletes with <strong>ACL</strong> injuries reported significant changes in Depression<br />
scores only. Different patterns of post-<strong>injury</strong> emotional disturbance for the injured groups were observed by trend analyses.<br />
Conclusions: Concussed athletes do not report as much emotional disturbance as athletes with <strong>ACL</strong> injuries. Differential<br />
patterns of emotional disturbance were detected between injured groups. The authors recommended that clinical pro<strong>to</strong>cols<br />
and educational programmes address emotional sequelae associated with <strong>sport</strong> <strong>concussion</strong> and <strong>ACL</strong> <strong>injury</strong>.<br />
Keywords: Sport <strong>concussion</strong>, emotional disturbance, profile of mood states, recovery, <strong>ACL</strong> <strong>injury</strong><br />
Introduction<br />
Sports <strong>concussion</strong> research has typically focused on<br />
neurocognitive and not on emotional sequelae.<br />
Clinical evidence suggests a connection between<br />
cerebral <strong>concussion</strong> and changes in emotional state.<br />
<strong>Emotional</strong> symp<strong>to</strong>ms such as depression and anxiety<br />
interfere with cognitive processes [1] and may rightly<br />
bear on short-term return-<strong>to</strong>-play decisions. Quite<br />
apart from that, emotional lability and depression, in<br />
particular, may have enduring and far reaching<br />
adverse psychological consequences for the athlete.<br />
Recent research and clinical anecdote suggest that<br />
the empirical investigation of emotional disturbance<br />
following <strong>concussion</strong> is warranted.<br />
In non-athletic mild brain-injured populations,<br />
emotional disturbances have been identified immediately<br />
after <strong>injury</strong> [2–4] and long after severe brain<br />
<strong>injury</strong> [5–8]. Depression is routinely reported after<br />
traumatic brain <strong>injury</strong> (TBI), regardless of <strong>injury</strong><br />
severity [9, 10]. Jorge and Robinson [11] identified<br />
the range of frequencies for depressive disorders<br />
following TBI as 6% in mild TBI <strong>to</strong> 77% in more<br />
severe cases. Despite these findings and clinical<br />
evidence of an association between emotional<br />
sequelae and protracted recovery, empirical studies<br />
are sparse [12].<br />
Recent prospective research of concussed athletes<br />
have revealed acute elevated depression, confusion,<br />
Correspondence: Dr Lynda Mainwaring, Faculty of Physical Education and Health, University of Toron<strong>to</strong>, 55 Harbord St. Toron<strong>to</strong>, ON M5S 2W6, Canada.<br />
Tel: (416) 946-5134. Fax: (416) 978-4384. E-mail: lynda.mainwaring@u<strong>to</strong>ron<strong>to</strong>.ca<br />
ISSN 0269–9052 print/ISSN 1362–301X online ß 2010 Informa Healthcare Ltd.<br />
DOI: 10.3109/02699051003610508
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
590 L. Mainwaring et al.<br />
fatigue, anger, overall mood disturbance and<br />
reduced vigour following <strong>sport</strong>s <strong>concussion</strong><br />
[13, 14]. Functional magnetic resonance imaging<br />
(fMRI) studies have shown a reduction in cerebral<br />
activity in the dorsolateral prefrontal cortex and<br />
increased neural activation in the anterior cingulate<br />
and medial orbi<strong>to</strong> frontal cortices of concussed<br />
athletes with depression [15]. Such findings are<br />
typically found in patients with major depressive<br />
disorder [16]. Depression increases the likelihood of<br />
anger, aggression, the risk of suicide and cognitive<br />
dysfunction following TBI [17–19]. Depression has<br />
also been identified as a possible long-term consequence<br />
of <strong>concussion</strong> in athletes by a large retrospective<br />
study. For example, football players with<br />
his<strong>to</strong>ries of previous <strong>concussion</strong> were found <strong>to</strong> be<br />
three times more likely diagnosed with depression<br />
after retirement [20].<br />
The <strong>sport</strong> psychology literature has not examined<br />
long-term consequences of <strong>sport</strong> <strong>injury</strong>, but has<br />
clearly established that temporary emotional disturbances<br />
exist as a consequence of athletic <strong>injury</strong>.<br />
Athletes report increased tension, anger, depression,<br />
reduced vigour and overall emotional disturbance<br />
following musculoskeletal injuries [21–24]. It is not<br />
clear, however, if different patterns of emotional<br />
sequelae are associated with different types of <strong>injury</strong><br />
and no research has examined whether different<br />
emotional <strong>response</strong>s are experience by athletes with<br />
musculoskeletal <strong>injury</strong> and athletes with cerebral<br />
<strong>concussion</strong>.<br />
The empirical literature on emotional reaction <strong>to</strong><br />
<strong>injury</strong> in <strong>sport</strong> is fraught with methodological<br />
difficulties related <strong>to</strong> terminology and measurement.<br />
For example, the terms mood, emotion and affect<br />
are often used interchangeably when distinct meanings<br />
associated with each of these constructs are used<br />
in the theoretical literature. It is beyond the scope of<br />
this paper <strong>to</strong> examine these shortcomings. For the<br />
purpose of this paper, emotional disturbance refers<br />
<strong>to</strong> changes in the characteristic way a person<br />
interprets and expresses his/her emotions or feelings.<br />
The purpose of this prospective study was <strong>to</strong><br />
examine and compare emotional disturbance and<br />
depression following <strong>sport</strong>s <strong>concussion</strong> and musculoskeletal<br />
<strong>injury</strong> relative <strong>to</strong> un-injured controls.<br />
Because much of the research on emotional <strong>response</strong><br />
<strong>to</strong> athletic <strong>injury</strong> has focused on anterior cruciate<br />
ligament (<strong>ACL</strong>) injuries and revealed that athletes<br />
experiences negative emotions following <strong>ACL</strong> <strong>injury</strong><br />
[25–29], athletes with <strong>ACL</strong> injuries were recruited as<br />
an <strong>injury</strong> control group. Three hypotheses were<br />
examined: The first, with the aim of ruling out<br />
pre-morbid emotional dysfunction, stated that there<br />
would be no differences in baseline scores of<br />
emotional functioning between groups of injured<br />
athletes and a control group of un-injured athletes;<br />
the second stated that emotional disturbance, as<br />
measured by changes in Total Mood Disturbance<br />
and Depression Scales of the Profile of Mood States<br />
(POMS) [30], would be evident post-<strong>injury</strong> for both<br />
injured groups; and the third examined whether<br />
emotional disturbance of athletes with cerebral<br />
<strong>concussion</strong> varied from that of athletes with <strong>ACL</strong><br />
injuries. Such research aims <strong>to</strong> enhance understanding<br />
of the nature of emotional sequelae of <strong>sport</strong><br />
<strong>concussion</strong> and shed light on whether those sequelae<br />
are a result of athletic <strong>injury</strong> experience in general or<br />
<strong>concussion</strong> specifically.<br />
Method<br />
Participants<br />
Three groups of University of Toron<strong>to</strong> undergraduate<br />
student-athletes participated: (1) Concussed<br />
varsity athletes (CONC: M ¼ 12, F ¼ 4), (2) athletes<br />
with confirmed anterior cruciate ligament injuries<br />
(<strong>ACL</strong>: M ¼ 1, F ¼ 6) and (3) Un-injured athletes<br />
(CTL: M ¼ 8, F ¼ 20). Athletes from nine varsity<br />
<strong>sport</strong>s teams (basketball, field hockey, football,<br />
hockey, lacrosse, mountain biking, rugby, soccer<br />
and volleyball) completed manda<strong>to</strong>ry baseline testing.<br />
If injured, and they met the inclusion/exclusion<br />
criteria and they volunteered for the study the<br />
athletes were assigned as appropriate <strong>to</strong> either the<br />
concussed or <strong>ACL</strong> group. The inclusion criteria for<br />
the <strong>ACL</strong> group specified that the <strong>injury</strong> had <strong>to</strong> meet<br />
diagnostic criteria for either suspect or confirmed<br />
<strong>ACL</strong> <strong>injury</strong> by a physician. All athletes approached<br />
with <strong>ACL</strong> injuries agreed <strong>to</strong> volunteer in the study;<br />
however, in some cases (n ¼ 2) the <strong>injury</strong> was not<br />
detected or reported within the time-frame necessary<br />
for participation in the research and so the athletes<br />
were not tested. The non-injured athletes were<br />
volunteers from a pool of students who were<br />
involved in <strong>sport</strong>s other than collision <strong>sport</strong>s and<br />
completed the baseline and serial test batteries.<br />
Written informed consent was completed at the first<br />
testing time and included a request for permission <strong>to</strong><br />
contact the athlete in the event s/he sustained a<br />
<strong>concussion</strong> or <strong>ACL</strong> <strong>injury</strong> at any game or practice<br />
throughout the athlete’s inter-university <strong>sport</strong> career.<br />
Consenting athletes who subsequently sustained<br />
cerebral <strong>concussion</strong> or <strong>ACL</strong>-<strong>injury</strong> were contacted<br />
by a research coordina<strong>to</strong>r, completed a second<br />
informed consent and were scheduled for a series<br />
of repeated assessments <strong>to</strong> moni<strong>to</strong>r recovery if they<br />
wished <strong>to</strong> volunteer for the research.<br />
Design and procedure<br />
The research pro<strong>to</strong>col was approved by the<br />
Ethics Review Office of the University of Toron<strong>to</strong>.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
The quasi-experimental design was a prospective<br />
mixed cohort design with repeated measures collected<br />
by two independent and mutually-blinded<br />
teams: (1) McIn<strong>to</strong>sh Sports Medicine Clinic physicians<br />
and therapists who identified and cared for<br />
injured athletes and (2) Toron<strong>to</strong> Rehabilitation<br />
Institute and University of Toron<strong>to</strong> psychologists<br />
and psychometrists. The clinicians were blinded <strong>to</strong><br />
neuropsychological test results so that return-<strong>to</strong>-play<br />
decisions were not influenced. Similarly, the<br />
researchers were not provided with the medical<br />
record data <strong>to</strong> provide objectivity in test administration<br />
and data collection. The <strong>sport</strong> medicine personnel<br />
were only informed of the results of the<br />
neuropsychological testing when a concussed athlete’s<br />
neuropsychological tests showed abnormal<br />
scores (determined by a neuropsychologist) and the<br />
athlete’s his<strong>to</strong>ry of <strong>concussion</strong> suggested the athlete<br />
may be at risk if returned <strong>to</strong> play prematurely.<br />
Baseline emotional states for all student-athletes<br />
participating in contact or collision <strong>sport</strong>s were<br />
measured during a 60-minute pre-season medical<br />
and neuropsychological assessment. All athletes<br />
were assessed during the competitive season,<br />
August through March. Participants in the noninjured<br />
control group completed serial tests during a<br />
similar assessment schedule from January <strong>to</strong> March.<br />
Concussions were identified by a physician,<br />
Certified Athletic Therapist or student therapist<br />
present at the sideline during either a practice or<br />
game, who applied specific assessment/diagnosis<br />
guidelines determined by the <strong>sport</strong>s medicine direc<strong>to</strong>r.<br />
Concussion was diagnosed based on the following<br />
criteria developed by the research team:<br />
(1) Observed or reported acceleration/deceleration<br />
of the head; (2) Any observable alteration in mental<br />
status; (3) Observable signs such as confusion,<br />
vacant stare, poor coordination, difficulty concentrating,<br />
poor balance; and/or (4) Any self-reported<br />
symp<strong>to</strong>ms such as headache, loss of consciousness,<br />
nausea, balance problems or difficulty reading<br />
or concentrating. After emergency was ruled out,<br />
a brief sideline mental status exam was administered<br />
<strong>to</strong> document post-concussive behaviour and<br />
symp<strong>to</strong>ms. Positive neurologic signs or unusual<br />
cognitive performance led <strong>to</strong> removal from competition<br />
and scheduling of serial post-<strong>injury</strong><br />
assessments.<br />
When possible, athletes were scheduled for<br />
post-<strong>injury</strong> assessments on days 1 (date of <strong>injury</strong>),<br />
4, 8, 15, 22 and 29. Team travel and student-athlete<br />
schedules often delayed the first post-<strong>injury</strong> time. As<br />
a consequence, the two groups of injured athletes<br />
completed their first post-<strong>injury</strong> assessments at<br />
significantly different time points during recovery<br />
[F(1, 20) ¼ 39.0, p < 0.05, 2 p ¼ 0.66]. Athletes in the<br />
concussed group completed Time 2 assessments an<br />
<strong>Emotional</strong> <strong>response</strong> <strong>to</strong> <strong>sport</strong> <strong>concussion</strong> 591<br />
average of 3.6 days (SD ¼ 2.2, Median ¼ 3 days,<br />
Range 1–9) post-<strong>injury</strong>. The athletes with <strong>ACL</strong><br />
injuries were seen an average of 11 days (SD ¼ 3.3,<br />
Median ¼ 11 days, Range 6–16) post-<strong>injury</strong>, largely<br />
due <strong>to</strong> <strong>injury</strong>-related mobility issues and delayed<br />
referral times. Because of the differences in<br />
post-<strong>injury</strong> testing days between groups, the data<br />
are presented by reference <strong>to</strong> the median days<br />
post-<strong>injury</strong> as well as by assessment time for each<br />
group. A matched cohort control group drawn from<br />
the contact/collision <strong>sport</strong>s was deliberately avoided.<br />
Exposing a sub-set of such uninjured cohort athletes<br />
<strong>to</strong> serial assessment would have jeopardized any<br />
subsequent clinical neuropsychological assessment<br />
and forced the exclusion of these athletes from<br />
participation in the research should they have<br />
sustained <strong>concussion</strong> [31].<br />
Measures<br />
Demographics. All participants completed a demographic<br />
questionnaire that assessed background<br />
information including age, sex, height, weight and<br />
previous <strong>concussion</strong> his<strong>to</strong>ry (up <strong>to</strong> a maximum of<br />
five previous <strong>concussion</strong>s).<br />
<strong>Emotional</strong> disturbance. Pre- and post-<strong>injury</strong> emotional<br />
<strong>response</strong>s were assessed with a short version of<br />
the Profile of Mood States (POMS) [30], which was<br />
chosen for its brief administration time and its use in<br />
<strong>sport</strong>. This version of the POMS consisted of 40<br />
adjectives (e.g. restless, discouraged) organized in<strong>to</strong><br />
seven sub-scales (1) Tension, (2) Depression, (3)<br />
Anger, (4) Vigour, (5) Fatigue, (6) Confusion and<br />
(7) Self-esteem. Participants rated each adjective on<br />
a 5-point Likert scale from 0 (not at all) <strong>to</strong> 4<br />
(extremely) according <strong>to</strong> how they feel ‘right now’.<br />
Total Mood Disturbance was calculated by subtracting<br />
positive mood scores (vigour and<br />
self-esteem) from the sum of negative mood scores<br />
then adding a constant of 100 [30]. These<br />
sub-scales have been previously assessed for reliability<br />
and validity, demonstrating Cronbach’s alphas<br />
ranging from 0.664–0.954 with a mean of<br />
0.798 [30].<br />
Statistical analysis<br />
POMS sub-scale reliabilities were examined with<br />
Cronbach’s alpha coefficients [32]. Demographics<br />
and physical characteristics were <strong>compared</strong> across<br />
groups using univariate analysis of variance<br />
(ANOVA) and Bonferroni-adjusted pairwise comparisons.<br />
Non-parametric Kruskal-Wallis tests were<br />
used for univariate ANOVAs when the data violated<br />
the parametric assumption of homogeneity of
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
592 L. Mainwaring et al.<br />
variances, as identified by Levene’s test for<br />
homogeneity.<br />
A one-way ANOVA for group and planned<br />
pairwise group comparisons at Time 1 were conducted<br />
<strong>to</strong> rule out pre-morbid dysfunction and test<br />
Hypothesis 1. To assess emotional dysfunction<br />
following <strong>injury</strong>, hypothesis 2, change scores for<br />
Total Mood and Depression between baseline and<br />
the first post-<strong>injury</strong> assessment were examined<br />
across the three groups with a one-way ANOVA<br />
with subsequent planned pairwise comparisons.<br />
Bonferroni-adjustments were used <strong>to</strong> control for<br />
Type I error inflation typically associated with<br />
multiple comparisons.<br />
To identify group differences in longitudinal<br />
emotional profiles (Hypothesis 3) a 3 (group) 4<br />
(time) repeated measures ANOVA (RM-ANOVA)<br />
was performed for each POMS sub-scale. Significant<br />
Group Time interactions were examined with<br />
polynomial trend analysis. Estimates of effect size<br />
are reported as partial eta-squared ( 2 p ), which can be<br />
thought of as the proportion of variance in the<br />
dependent variable that is explained by differences<br />
among the groups regardless of group size. For the<br />
RM-ANOVAs Mauchly’s test of sphericity was used<br />
<strong>to</strong> identify violations in the assumption of sphericity<br />
(homogeneity of variances for repeated fac<strong>to</strong>rs).<br />
Where violations in sphericity were identified,<br />
Greenhouse-Geisser corrections were made <strong>to</strong> the<br />
F-statistic.<br />
Results<br />
Descriptive statistics<br />
Reliabilities for each sub-scale of the POMS<br />
short-form were calculated with Cronbach alpha<br />
coefficients [32]. All alphas exceeded the recommended<br />
0.70 [33] except for Self-Esteem.<br />
The average age across the groups was 21.2 years<br />
(SD ¼ 2.94; Range 17.5–37.0) with no differences<br />
between groups [F(2, 48) ¼ 0.80, p ¼ 0.46,<br />
2<br />
p ¼ 0.03]. There were significant differences in<br />
2 height [F(2, 48) ¼ 6.75, p < 0.01, p ¼ 0.22] and<br />
2 weight [F(2, 48) ¼ 9.04, p < 0.01, p ¼ 0.27] among<br />
the groups, with the Concussed group being<br />
significantly taller (4.2; p ¼ 0.02, 95% CI ¼ 1.4,<br />
7.1) and heavier (32 lbs; p < 0.01, 95% CI ¼ 13.0,<br />
50.7) than the control group. The concussed athletes<br />
were an average of 28 pounds heavier than the<br />
athletes with <strong>ACL</strong> injuries. Concussed athletes were<br />
removed from play for an average of 25 days and<br />
returned <strong>to</strong> play 10 days after the fourth assessment<br />
time, which was day 14 post-<strong>injury</strong>. Athletes<br />
with <strong>ACL</strong> injuries failed <strong>to</strong> report a single prior<br />
<strong>concussion</strong>, contributing <strong>to</strong> a significant Levene’s<br />
test (homogeneity of variance) [Levene’s statistic<br />
(2, 48) ¼ 6.75, p < 0.01]. The ensuing nonparametric<br />
Kruskal-Wallis test was significant<br />
[ 2 2 (2, 48) ¼ 10.9, p < 0.01] and indicated differences<br />
in the average number of prior <strong>concussion</strong>s reported<br />
by each group. The concussed group had the highest<br />
number of mean previous <strong>concussion</strong>s (1.4,<br />
SD ¼ 1.3) followed by the uninjured group (1.00,<br />
SD ¼ 1.00) and the athletes with <strong>ACL</strong> injuries (0).<br />
Baseline assessments. A one-way ANOVA revealed<br />
that injured groups did not differ from uninjured<br />
healthy controls in baseline assessment on any of the<br />
sub-scales of the POMS and, thus, Hypothesis 1 was<br />
supported. Table I shows POMS means and standard<br />
deviations for each group at each assessment<br />
time for the main outcome measures, Total Mood<br />
and Depression. Homogeneity of variance was<br />
demonstrated for each sub-scale.<br />
First post-<strong>injury</strong> assessment. A one-way ANOVA by<br />
group on change scores between pre-<strong>injury</strong> and the<br />
first post-<strong>injury</strong> assessment revealed significant<br />
differences for Total Mood Disturbance<br />
[F(2, 48) ¼ 3.369, p < 0.04] and Depression<br />
[F(2, 48) ¼ 6.866, p < 0.002]. Tukey HSD tests<br />
determined that the Concussed group differed<br />
from the uninjured control (p ¼ 0.03) for Total<br />
Mood Disturbance and also for Depression<br />
(p ¼ 0.03). The <strong>ACL</strong> group was significantly different<br />
from the uninjured control group on Depression<br />
(p ¼ 0.005). Although concussed athletes endorsed<br />
almost three times more Depression at the first<br />
post-<strong>injury</strong> assessment (Time 2) than they did prior<br />
<strong>to</strong> <strong>injury</strong> at baseline, athletes with <strong>ACL</strong> injuries<br />
Table I. Profile of mood state depression and <strong>to</strong>tal mood<br />
disturbance scores for three groups (CON, <strong>ACL</strong> and CTL) at<br />
each of four test sessions.<br />
CONC (n ¼ 16) <strong>ACL</strong> (n ¼ 7) CTL (n ¼ 28)<br />
Session M SD M SD M SD<br />
Depression<br />
1 1.31 2.55 0.71 0.95 1.54 3.13<br />
2 3.75 4.55 5.00 4.40 1.54 2.41<br />
3 1.69 2.63 2.71 2.56 0.86 1.69<br />
4 0.63 1.78 0.86 1.22 1.32 2.23<br />
Total*<br />
1 97.81 18.89 105.43 15.55 102.21 15.19<br />
2 116.69 22.39 114.71 14.12 106.36 13.38<br />
3 108.44 17.17 110.86 18.18 100.89 14.52<br />
4 100.69 12.29 104.57 12.51 105.61 14.04<br />
*Total ¼ (tension þ depression þ anger þ fatigue þ confusion) þ<br />
(vigour þ esteem) þ 100.<br />
1 ¼ baseline test; 2 ¼ first post-<strong>injury</strong> assessment (4 days); 3 ¼ 7<br />
days post-<strong>injury</strong>; 4 ¼ 14 days post-<strong>injury</strong>.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
reported over seven times more Depression after<br />
<strong>injury</strong> than at baseline (see Table I).<br />
Longitudinal emotional functioning<br />
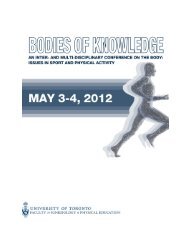
Total mood disturbance. A 3 (group) 4 (time)<br />
RM-ANOVA detected a significant interaction for<br />
Total Mood Disturbance scores [F(6, 144) ¼ 2.99,<br />
2 p < 0.01, p ¼ 0.11] with a significant simple main<br />
effect for the concussed group [F(3, 45) ¼ 6.20,<br />
2<br />
p < 0.01, ¼ 0.29]. Polynomial trend analyses<br />
revealed a significant quadratic trend for the<br />
concussed group [F(1, 15) ¼ 11.72, p < 0.01,<br />
2<br />
p ¼ 0.44] (see Figure 1). Again, homogeneity of<br />
variance was present for all assessment times except<br />
Time 2, in which concussed athletes showed a<br />
strikingly large variability relative <strong>to</strong> athletes with<br />
<strong>ACL</strong> <strong>injury</strong>.<br />
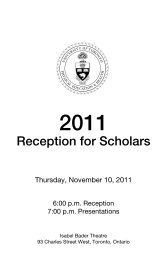
Depression. A3 4 RM-ANOVA detected a significant<br />
Group Time interaction [F(6, 144) ¼ 4.53,<br />
2 p < 0.01, p ¼ 0.16] for Depression scores and a<br />
significant simple main effect for time for the<br />
concussed athletes [F(3, 45) ¼ 4.90, p < 0.01,<br />
2<br />
p ¼ 0.25] (see Figure 2). Polynomial trend analyses<br />
revealed a significant quadratic trend [F(1,48) ¼<br />
2 6.98, p < 0.02, p ¼ 0.32] and near significant cubic<br />
trend for depression (p ¼ 0.056). For the athletes<br />
with <strong>ACL</strong> injuries there was also a significant simple<br />
main effect of time for depression [F(3, 18) ¼ 6.46,<br />
2 p < 0.01, p ¼ 0.52] which followed a quadratic<br />
2 trend [F(1, 6) ¼ 11.3, p < 0.02, p ¼ 0.65].<br />
<strong>Emotional</strong> <strong>response</strong> <strong>to</strong> <strong>sport</strong> <strong>concussion</strong> 593<br />
Homogeneity of variance was noted at all times<br />
except Time 2, when the injured athlete groups<br />
showed marked within-group variability relative <strong>to</strong><br />
uninjured controls.<br />
No simple main effects were significant for the<br />
control group (CTL) for any sub-scale.<br />
Discussion<br />
Consistent with other research, results of this study<br />
suggest <strong>response</strong> <strong>to</strong> athletic <strong>injury</strong> is not a result of<br />
pre-morbid emotional dysfunction [34, 35]. This<br />
study supported the first hypothesis and ruled out<br />
pre-<strong>injury</strong> emotional disturbances in athletes with<br />
<strong>concussion</strong> and those with <strong>ACL</strong> injuries.<br />
The second hypothesis that emotional functioning<br />
would deteriorate post-<strong>injury</strong> for both injured groups<br />
was partially accepted in that both groups reported<br />
significant increases in depression scores post-<strong>injury</strong><br />
<strong>compared</strong> with the un-injured group. Concussed<br />
athletes reported significant changes in overall emotional<br />
disturbance post-<strong>injury</strong> <strong>compared</strong> with the<br />
un-injured athletes, but not when <strong>compared</strong> <strong>to</strong> the<br />
athletes with <strong>ACL</strong> injuries. These findings support<br />
the suspected causal link between athletic <strong>injury</strong> and<br />
subsequent emotional distress [22, 25, 29, 36–40],<br />
but indicate that there are different patterns of<br />
emotional disturbance associated with different<br />
injuries. Athletes with <strong>ACL</strong> injuries reported over<br />
seven times more depression 11 days post-<strong>injury</strong><br />
than at baseline. In contrast, 4 days post-<strong>injury</strong><br />
Figure 1. Profile of POMS <strong>to</strong>tal mood disturbance scores for each group over time—using group median post-<strong>injury</strong> testing dates.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
594 L. Mainwaring et al.<br />
Figure 2. Profile of POMS depression ratings for each group over time—using group median post-<strong>injury</strong> testing dates.<br />
concussed athletes showed elevated depression<br />
scores three times greater than scores at baseline,<br />
but the elevations resolved 1 week after <strong>injury</strong><br />
Statistical differences in patterns of recovery<br />
between injured groups and the un-injured controls<br />
(Hypothesis 3) were not supported by analysis of<br />
variance. Detectable differences between groups<br />
may have been concealed by the variability in the<br />
data and small sample sizes. In order <strong>to</strong> detect<br />
statistically significant between-group post-<strong>injury</strong><br />
differences in emotions, if they are <strong>to</strong> be found,<br />
very large samples or more sensitive measures are<br />
needed. Low incidence and reporting of <strong>ACL</strong> <strong>injury</strong><br />
and incomplete post-<strong>injury</strong> serial tests were limiting<br />
fac<strong>to</strong>rs <strong>to</strong> increased sample sizes in this study. It is<br />
difficult <strong>to</strong> recruit athletes with <strong>ACL</strong> injuries for<br />
serial neuropsychological and emotional testing<br />
because of the nature of the <strong>injury</strong> and the physical<br />
treatment required. Also, there is little incentive for<br />
these athletes <strong>to</strong> devote hours of their time <strong>to</strong><br />
repeated and seemingly irrelevant neuropsychological<br />
testing. Systematic patterns of disturbance in<br />
<strong>to</strong>tal mood disturbance and depression, however,<br />
were revealed in the two injured groups by polynomial<br />
trend analysis. No systematic differences in<br />
patterns of <strong>response</strong> over time were observed in the<br />
uninjured control group. Polynomial analyses<br />
showed more prolonged <strong>to</strong>tal disturbance and<br />
depression in the <strong>ACL</strong> group, whereas the concussed<br />
group displayed acute brief (1-week) elevated <strong>to</strong>tal<br />
disturbance and depression scores post-<strong>injury</strong>. The<br />
more prolonged and intense overall disturbance and<br />
depression in the <strong>ACL</strong> group may have been<br />
due <strong>to</strong> the <strong>injury</strong> severity, mobility limitations<br />
and greater rehabilitation involvement (e.g. MRI,<br />
surgery etc.).<br />
Other research [13] found depression scores for<br />
athletes with minor musculoskeletal injuries (ankle,<br />
wrist and shoulder strains and sprains) resolved over<br />
2-weeks post-<strong>injury</strong>, whereas elevated depression<br />
scores for concussed athletes returned <strong>to</strong> baseline in<br />
just over 1-week post-<strong>injury</strong>. Those findings, along<br />
with the results from this study, suggest that the<br />
nature and quality of emotional disturbance and<br />
perhaps the causal mechanism for <strong>concussion</strong> is<br />
different from that of musculoskeletal injuries.<br />
In this study changes in Total Mood Disturbance<br />
was also shown post-<strong>injury</strong> for the concussed<br />
athletes but not for the athletes with <strong>ACL</strong> <strong>injury</strong>.<br />
Prior research has demonstrated significant, albeit<br />
temporary, overall emotional disturbance following<br />
<strong>ACL</strong> <strong>injury</strong> [25, 27, 28]. The non-significant<br />
findings for the <strong>ACL</strong> group were probably a result<br />
of the small sample and variability within the sample<br />
and the inability <strong>to</strong> test the athletes 4 days<br />
post-<strong>injury</strong>. Although these findings are consistent<br />
with findings that TMD scores were not elevated in<br />
athletes with minor musculoskeletal injuries [13],<br />
they are inconsistent with the graphic representation<br />
(Figure 1), which illustrates post-<strong>ACL</strong>-<strong>injury</strong> elevation<br />
in TMD that returns <strong>to</strong> baseline 23 days<br />
post-<strong>injury</strong>, later than that of the concussed athletes.<br />
It is recommended that future studies take a closer<br />
look at post-<strong>injury</strong> differences in overall emotional
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
disturbance of athletes with <strong>concussion</strong> and those<br />
with musculoskeletal injuries.<br />
Overall emotional disturbance and depression<br />
seen in the first week post-<strong>concussion</strong> in the study<br />
mirrors the neurocognitive changes identified in<br />
many other <strong>concussion</strong> studies [41–48]. These<br />
transient changes in cognitive and emotional functioning<br />
seem <strong>to</strong> reflect athletes’ feelings of being ‘off’<br />
or in a ‘fog’ [49] and it is speculated that they<br />
resonate with the transient neurochemical cascade<br />
[50–52] and physiologic disturbances [15] associated<br />
with brain trauma. Silver et al. [53] suggested<br />
that early post-traumatic depression was more likely<br />
related <strong>to</strong> a ‘host-<strong>injury</strong> interaction’ (p. 657) than<br />
later post-traumatic depression.<br />
Some authors have argued that emotional disturbance<br />
following <strong>injury</strong> is related <strong>to</strong> removal from<br />
competition rather than the <strong>injury</strong> itself [36].<br />
Therefore, return-<strong>to</strong>-play dates were examined.<br />
<strong>Emotional</strong> changes abated prior <strong>to</strong> the athlete’s<br />
return <strong>to</strong> play, which was on average 25 days<br />
post-<strong>injury</strong> for the concussed group: Total Mood<br />
Disturbance scores returned <strong>to</strong> baseline levels 14<br />
days post-<strong>concussion</strong> and depression scores returned<br />
<strong>to</strong> baseline by the 7th day post-<strong>concussion</strong>. This<br />
finding suggests that removal from play is not the<br />
underlying fac<strong>to</strong>r that triggers depression or emotional<br />
disturbance in concussed athletes.<br />
The elevated overall emotional disturbance and<br />
depression scores post-<strong>concussion</strong> could also represent<br />
withdrawal from the endogenous opiates associated<br />
with feelings of well-being. The daily routines<br />
of athletes involve intense training, and it is possible<br />
that the short abrupt disruption in training associated<br />
with <strong>concussion</strong> disturbs neurochemistry.<br />
There is evidence that aerobic exercise increases<br />
endogenous opiates and feelings of well-being<br />
[54–57]. Athletes who are unable <strong>to</strong> train because<br />
of <strong>injury</strong> may experience an absence of such<br />
neurochemical boosts as emotional disturbance in<br />
association with the neurochemical cascade identified<br />
with cerebral <strong>concussion</strong> [50–52]. These ideas<br />
need <strong>to</strong> be examined in future research.<br />
Physical differences were seen between groups.<br />
The concussed group was physically heavier than the<br />
<strong>ACL</strong> group and taller and heavier than the uninjured<br />
control group. These physical differences were likely<br />
the result of a disproportionate number of females in<br />
the uninjured comparison group and the <strong>ACL</strong><br />
group. In addition, the athletes with <strong>ACL</strong> injuries<br />
did not report any his<strong>to</strong>ry of <strong>concussion</strong>, whereas,<br />
consistent with previous research [58–60], the<br />
concussed group reported a significantly different<br />
number (1.4) of previous <strong>concussion</strong>s. There were<br />
no sex differences in emotional <strong>response</strong> <strong>to</strong> <strong>injury</strong>,<br />
but this could have been an artifact of insufficient<br />
power <strong>to</strong> detect differences. Ideally, groups would be<br />
<strong>Emotional</strong> <strong>response</strong> <strong>to</strong> <strong>sport</strong> <strong>concussion</strong> 595<br />
matched on sex and other variables such as time<br />
intervals between testing sessions for all <strong>injury</strong><br />
sub-groups. The authors recognize these as limitations<br />
<strong>to</strong> this study.<br />
In summary, over a 3-week period of assessment,<br />
both concussed and <strong>ACL</strong>-injured groups had emotional<br />
disturbance that declined as athletes recovered.<br />
Depression was more prolonged and intense<br />
for the athletes with <strong>ACL</strong> injuries, whereas concussed<br />
athletes reported elevated depression as well<br />
as overall emotional disturbance that resolved within<br />
1-week post-<strong>injury</strong>.<br />
Assessing emotional <strong>response</strong> <strong>to</strong> <strong>concussion</strong> has<br />
many methodological challenges, such as inconsistencies<br />
in <strong>injury</strong> reporting, the logistics of <strong>injury</strong><br />
reporting mechanisms, sensitivity <strong>to</strong> the varied<br />
interests of coaches, athletes and medical personnel<br />
and the appropriateness of sensitive and brief measures.<br />
Well-articulated pro<strong>to</strong>cols for <strong>injury</strong> reporting,<br />
sound communication patterns and computerized<br />
measures of emotion [61] are recommended for<br />
future studies.<br />
These findings need <strong>to</strong> be replicated and the<br />
methods refined <strong>to</strong> make any definitive statements<br />
about the nuanced emotional differences after <strong>concussion</strong><br />
and <strong>ACL</strong> <strong>injury</strong> or musculoskeletal <strong>injury</strong> in<br />
general. The variability in individual <strong>response</strong> <strong>to</strong><br />
<strong>injury</strong> in both injured groups reinforces the assertion<br />
that individuals need <strong>to</strong> be treated relative <strong>to</strong> their<br />
own pre-<strong>injury</strong> and post-<strong>injury</strong> performance on any<br />
assessment [41, 43]. It also points <strong>to</strong> the importance<br />
of interpreting an individual’s data in terms of<br />
clinical significance and not merely statistical<br />
significance.<br />
In conclusion, it is believed that it is important <strong>to</strong><br />
assess and study emotional functioning following<br />
<strong>concussion</strong> and <strong>to</strong> compare it <strong>to</strong> the <strong>response</strong><br />
associated with musculoskeletal <strong>injury</strong> in order <strong>to</strong><br />
discern which <strong>response</strong>s are associated with brain<br />
<strong>injury</strong> and which are a result of the psychosocial–<br />
behavioural consequences of the <strong>injury</strong> experience<br />
overall. Assessment of post-<strong>injury</strong> emotional functioning<br />
could help <strong>to</strong> inform return-<strong>to</strong>-play decisions<br />
so that athletes do not return-<strong>to</strong>-play with emotional<br />
disturbance, which might create a risk for further<br />
injuries. Often, athletes will not report emotional<br />
disturbance because they do not realize that such<br />
symp<strong>to</strong>ms may be related <strong>to</strong> <strong>injury</strong> and because<br />
attitudes that reflect a play despite <strong>injury</strong> mentality<br />
associated with the culture of risk in <strong>sport</strong> [62] often<br />
influence under-reporting and denial of symp<strong>to</strong>ms<br />
and injuries. In addition, moni<strong>to</strong>ring post-traumatic<br />
emotional disturbances, in particular depression, in<br />
both concussed athletes and athletes with <strong>ACL</strong><br />
injuries can potentially prevent emotional deterioration<br />
and facilitate early intervention.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
596 L. Mainwaring et al.<br />
It is recommended that future research on <strong>concussion</strong><br />
in <strong>sport</strong> expands beyond the typical neurocognitive<br />
test battery <strong>to</strong> include the following: (1) An<br />
examination of short- and long-term emotional<br />
reactions post-<strong>injury</strong>, (2) Risk fac<strong>to</strong>rs for depressive<br />
reaction following <strong>concussion</strong>, (3) Enhanced and<br />
au<strong>to</strong>mated measures of emotion, which include a<br />
broader range of emotions and more sensitive and<br />
specific tests, and (4) Examination of injured<br />
sub-group comparisons (minor musculoskeletal injuries,<br />
for example). Finally, it is recommended that<br />
<strong>concussion</strong> management pro<strong>to</strong>cols include<br />
post-<strong>injury</strong> emotional testing and moni<strong>to</strong>ring in the<br />
interest of early comprehensive intervention and<br />
successful outcome; and that educational programmes<br />
acknowledge and emphasize emotional<br />
symp<strong>to</strong>ms as sequelae of <strong>concussion</strong>. <strong>Emotional</strong><br />
symp<strong>to</strong>ms post-<strong>concussion</strong> need <strong>to</strong> be assessed<br />
clinically and empirically [63].<br />
Declaration of interest: The authors report<br />
no conflicts of interest. The authors alone are<br />
responsible for the content and writing of the paper.<br />
References<br />
1. Bechara A, Damasio H, Damasio AR, Lee GP. Different<br />
contributions of the human amygdala and ventromedial<br />
prefrontal cortex <strong>to</strong> decision-making. The Journal of<br />
Neuroscience 1999;19:5473–5481.<br />
2. Paniak C, Reynolds S, Toller-Lobe G, Melnyk A, Nagy J,<br />
Schmidt D. A longitudinal study of the relationship between<br />
financial compensation and symp<strong>to</strong>ms after treated mild<br />
traumatic brain <strong>injury</strong>. Journal of Clinical and Experimental<br />
Neuropsychology 2002;24:187–193.<br />
3. Dikmen S, McLean A, Temkin N. Neuropsychological and<br />
psychosocial consequences of minor head <strong>injury</strong>. Journal of<br />
Neurology, Neurosurgery and Psychiatry 1986;49:<br />
1227–1232.<br />
4. Levin HS, Mattis S, Ruff RM, Eisenberg HM, Marshall LF,<br />
Tabaddor K, et al. Neurobehavioral outcome following<br />
minor head <strong>injury</strong>: A three-center study. Journal of<br />
Neurosurgy 1987;66:234–243.<br />
5. Malia K, Powell G, Torode S. Personality and psychosocial<br />
function after brain <strong>injury</strong>. Brain Injury 1995;9:697–712.<br />
6. Bornstein RA, Miller HB, van Schoor JT.<br />
Neuropsychological deficit and emotional disturbance in<br />
head-injured patients. Journal of Neurosurgery 1989;70:<br />
509–513.<br />
7. Gasquoine PG. Post<strong>concussion</strong> symp<strong>to</strong>ms. Neuropsychology<br />
Review 1997;7:77–85.<br />
8. Brooks DN, McKinlay W. Personality and behavioural<br />
change after severe blunt head <strong>injury</strong>—a relative’s view.<br />
Journal of Neurology, Neurosurgery and Psychiatry 1983;46:<br />
336–344.<br />
9. Kreutzer JS, Seel RT, Gourley E. The prevalence and<br />
symp<strong>to</strong>m rates of depression after traumatic brain <strong>injury</strong>: A<br />
comprehensive examination. Brain Injury 2001;15:563–576.<br />
10. Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J,<br />
DeKosky S. Prevalence of neuropsychiatric symp<strong>to</strong>ms in<br />
dementia and mild cognitive imipairment: Results from the<br />
cardiovascular health study. JAMA 2002;288:1475–1483.<br />
11. Jorge R, Robinson R. Mood disorders following traumatic<br />
brain <strong>injury</strong>. NeuroRehabiliation 2002;17:11–324.<br />
12. Johns<strong>to</strong>n KM, McCrory P, Mohtadi NG, Meeuwisse W.<br />
Evidence-based review of <strong>sport</strong>-related <strong>concussion</strong>: Clinical<br />
science. Clinical Journal of Sport Medicine 2001;11:<br />
150–159.<br />
13. Hutchison M, Mainwaring L, Comper P, Richards DW,<br />
Bisschop S. Differential emotional <strong>response</strong>s of varsity<br />
athletes <strong>to</strong> <strong>concussion</strong> and musculoskeletal injuries. Clinical<br />
Journal of Sport Medicine 2009;19:13–19.<br />
14. Mainwaring LM, Bisschop SM, Green R, An<strong>to</strong>niazzi M,<br />
Comper P, Kristman V, et al. <strong>Emotional</strong> reaction of varsity<br />
athletes <strong>to</strong> <strong>sport</strong>-related <strong>concussion</strong>. Journal of Sport and<br />
Exercise Psychology 2004;26:119–135.<br />
15. Chen J-K, Johns<strong>to</strong>n KM, Petrides M. Neural substrates of<br />
symp<strong>to</strong>ms of depression following <strong>concussion</strong> in male<br />
athletes with persisting post<strong>concussion</strong> symp<strong>to</strong>ms. Archives<br />
of General Psychiatry 2008;65:81–89.<br />
16. Liotti M, Mayberg HS, Brannan SK, McGinnis S, Jerabek P,<br />
Fox PT. Differential limbic-cortical correlates of sadness and<br />
anxiety in healthy subjects: Implications for affective disorders.<br />
Biological Psychiatry 2000;48:30–42.<br />
17. Fann JR, Ka<strong>to</strong>n WJ, Uomo<strong>to</strong> JM, Esselman PC. Psychiatric<br />
disorders and functional disability in outpatients with traumatic<br />
brain injuries. American Journal of Psychiatry<br />
1995;152:1493–1499.<br />
18. Hibbard MR, Uysal S, Kepler K, Bogdany J, Silver J. Axis I<br />
psychopathology in inidividuals with traumatic brain <strong>injury</strong>.<br />
Journal of Head Trauma Rehabilitation 1998;13:24–39.<br />
19. Rapoport MJ, McCullagh S, Shammi P, Feinstein A.<br />
Cognitive impairment associated with major depression<br />
following mild and moderate traumatic brain <strong>injury</strong>. Journal<br />
of Neuropsychiatry and Clinical Neuroscience 2005;17:<br />
61–65.<br />
20. Guskiewicz KM, Marshall SW, Bailes J, McCrea M,<br />
Harding HP, Matthews A, et al. Recurrent <strong>concussion</strong> and<br />
risk of depression in retired professional football players.<br />
Medicine and Science in Sports and Exercise 2007;39:<br />
903–909.<br />
21. Leddy MH, Lamber MJ, Ogles BM. Psychological<br />
consequences of athletic <strong>injury</strong> among high-level competi<strong>to</strong>rs.<br />
Research Quarterly for Exercise and Sport 1994;65:<br />
347–354.<br />
22. Smith AM, Stuart MJ, Wiese-Bjornstal DM, Milliner EK,<br />
O’Fallon WM, Crowson CS. Competitive athletes: Pre-<strong>injury</strong><br />
and post<strong>injury</strong> mood state and self-esteem. Mayo Clinic<br />
Proceedings 1993;68:939–947.<br />
23. Roh J, Newcomer RR, Perna FM, Etzel EF. Depressive<br />
mood states among college athletes: Pre- and post-<strong>injury</strong>.<br />
Journal of Applied Sport Psychology 1998;10(Suppl):S54.<br />
24. Miller WN. Athletic <strong>injury</strong>: Mood disturbances and hardiness<br />
of intercollegiate athletes. Journal of Applied Sport<br />
Psychology 1998;10(Suppl):S127–S128.<br />
25. Brewer BW, Van Raalte JL, Cornelius AE, Petitpas AJ,<br />
Sklar JH, Pohlman MH. Psychological fac<strong>to</strong>rs, rehabilitation<br />
adherence and rehabilitation outcome after anterior cruciate<br />
ligament reconstruction. Rehabilitation Psychology 2000;45:<br />
20–37.<br />
26. Brewer BW, Linder DE, Phelps CM. Situational correlates of<br />
emotional adjustment <strong>to</strong> athletic <strong>injury</strong>. Clinical Journal of<br />
Sport Medicine 1995;5:241–245.<br />
27. Daly JM, Brewer BW, Van Raalte JL, Petitpas AJ, Sklar JH.<br />
Cognitive appraisal, emotional adjustment, and adherence <strong>to</strong><br />
rehabilitation following knee surgery. Journal of Sport<br />
Rehabilitation 1995;4:23–30.<br />
28. Mainwaring LM. Res<strong>to</strong>ration of self: A model for the<br />
psychological <strong>response</strong> of athletes <strong>to</strong> severe knee injuries.<br />
Canadian Journal of Rehabilitation 1999;12:145–156.
Brain Inj Downloaded from informahealthcare.com by University of Toron<strong>to</strong> on 07/12/11<br />
For personal use only.<br />
29. Morrey MA, Stuart MJ, Smith AM, Wiese-Bjornstal DM. A<br />
longitudinal examination of athletes’ emotional and cognitive<br />
<strong>response</strong>s <strong>to</strong> anterior cruciate ligament <strong>injury</strong>. Clinical<br />
Journal of Sport Medicine 1999;9:63–69.<br />
30. Grove J, Prapavessis H. Preliminary evidence for the reliability<br />
and validity of an abbreviated Profile of Mood States.<br />
International Journal of Sport Psychology 1992;23:93–109.<br />
31. Hin<strong>to</strong>n-Bayre AD, Geffen GM, Geffen LB, McFarland KA,<br />
Friis P. Concussion in contact <strong>sport</strong>s: Reliable change indices<br />
of impairment and recovery. Journal of Clinical and<br />
Experimental Neuropsychology 1999;21:70–86.<br />
32. Cronbach LJ, Meehl PE. Construct validity in psychological<br />
tests. Psychological Bulletin 1955;52:281–302.<br />
33. Nunnely J. Psychometric theory. 2nd ed. New York:<br />
McGraw Hill; 1978.<br />
34. Leddy MH, Lambert MJ, Ogles BM. Psychological consequences<br />
of athletic <strong>injury</strong> among high-level competi<strong>to</strong>rs.<br />
Research Quarterly for Exercise and Sport 1994;65:347–354.<br />
35. Smith AM, Stuart MJ, Wiese-Bjornstal DM, Milliner EK,<br />
O’Fallon WM, Crowson CS. Competitive athletes: Pre-<strong>injury</strong><br />
and post<strong>injury</strong> mood state and self-esteem. Mayo Clinic<br />
Proceedings 1993;68:939–947.<br />
36. Chan CS, Grossman HY. Psychological effects of running<br />
loss on consistent runners. Perceptual and Mo<strong>to</strong>r Skills<br />
1988;66:875–883.<br />
37. Chute N. Psychological <strong>response</strong>s and adjustments <strong>to</strong> <strong>sport</strong><br />
injuries by varsity athletes. Master’s Thesis. Kings<strong>to</strong>n,<br />
Canada: Queen’s University; 1997.<br />
38. McDonald SA, Hardy DJ. Affective <strong>response</strong> patterns of the<br />
injured athlete: An explora<strong>to</strong>ry analysis. The Sport<br />
Psychologist 1990;4:261–274.<br />
39. Smith AM, Scott SG, O’Fallon WM, Young ML. <strong>Emotional</strong><br />
<strong>response</strong>s of athletes <strong>to</strong> <strong>injury</strong>. Mayo Clinic Proceedings<br />
1990;65:38–50.<br />
40. Pearson L, Jones G. <strong>Emotional</strong> effects of <strong>sport</strong>s injuries:<br />
Implications for physiotherapists. Physiotherapy 1992;78:<br />
762–770.<br />
41. Echemendia RJ, Putukian M, Mackin RS, Julian L, Shoss N.<br />
Neuropsychological test performance prior <strong>to</strong> and following<br />
<strong>sport</strong>s-related mild traumatic brain <strong>injury</strong>. Clinical Journal of<br />
Sport Medicine 2001;11:23–31.<br />
42. Lovell MR, Collins MW, Iverson GL, Field M, Maroon JC,<br />
Cantu R, et al. Recovery from mild <strong>concussion</strong> in high school<br />
athletes. Journal of Neurosurgery 2003;98:296–301.<br />
43. Lovell MR, Collins MW, Iverson GL, Johns<strong>to</strong>n KM,<br />
Bradley JP. Grade 1 or ‘ding’ <strong>concussion</strong>s in high school<br />
athletes. American Journal of Sports Medicine 2004;32:<br />
47–54.<br />
44. Macciocchi SN, Barth JT, Alves W, Rimel RW, Jane JA.<br />
Neuropsychological functioning and recovery after mild head<br />
<strong>injury</strong> in collegiate athletes. Neurosurgery 1996;39:510–514.<br />
45. McCrea M, Guskiewicz KM, Marshall SW, Barr W,<br />
Randolph C, Cantu RC, et al. Acute effects and recovery<br />
time following <strong>concussion</strong> in collegiate football players: The<br />
NCAA Concussion Study. JAMA 2003;290:2556–2563.<br />
46. McCrea M, Kelly JP, Randolph C, Cisler R, Berger L.<br />
Immediate neurocognitive effects of <strong>concussion</strong>.<br />
Neurosurgery 2002;50:1032–1040, discussion 1040–1042.<br />
47. Pellman EJ, Lovell MR, Viano DC, Casson IR, Tucker AM.<br />
Concussion in professional football: Neuropsychological<br />
<strong>Emotional</strong> <strong>response</strong> <strong>to</strong> <strong>sport</strong> <strong>concussion</strong> 597<br />
testing—part 6. Neurosurgery 2004;55:1290–1303, discussion<br />
1303–1305.<br />
48. Bleiberg J, Cernich AN, Cameron K, Sun W, Peck K,<br />
Ecklund PJ, et al. Duration of cognitive impairment after<br />
<strong>sport</strong>s <strong>concussion</strong>. Neurosurgery 2004;54:1073–1078, discussion<br />
1078–1080.<br />
49. Iverson GL, Gaetz M, Lovell MR, Collins MW. Relation<br />
between subjective fogginess and neuropsychological testing<br />
following <strong>concussion</strong>. Journal of the International<br />
Neuropsychological Society 2004;10:904–906.<br />
50. Giza CC, Hovda DA. The neurometabolic cascade of<br />
<strong>concussion</strong>. Journal of Athletic Training 2001;36:228–235.<br />
51. Hovda DA, Becker DP, Katayama Y. Secondary <strong>injury</strong> and<br />
acidosis. Journal of Neurotrauma 1992;9(Suppl 1):S47–S60.<br />
52. Hovda DA, Prins M, Becker DP, Lee S, Bergsneider M,<br />
Martin NA. Neurobiology of <strong>concussion</strong>. In: Bailes JE, Lovell<br />
MR, Maroon JC, edi<strong>to</strong>rs. Sports related <strong>concussion</strong>. St.<br />
Louis: Quality Medical Publishing; 1999. pp 12–51.<br />
53. Silver J, McAllister T, Arciniegas D. Depression and cognitive<br />
complaints following mild traumatic brain <strong>injury</strong>. The<br />
American Journal of Psychiatry 2009;166:653–661.<br />
54. Hoffmann P. Physical activity and mental health. In: Morgan<br />
WP, edi<strong>to</strong>r. Physical activity and mental health. Series in<br />
health psychology and behavioural medicine. Philadelphia,<br />
PA: Taylor & Francis; 1997. pp 163–177.<br />
55. Kraemer WJ, Dziados JE, Marchitelli LJ, Gordon SE,<br />
Harman EA, Mello R, et al. Effects of different<br />
heavy-resistance exercise pro<strong>to</strong>cols on plasma beta-endorphin<br />
concentrations. Journal of Applied Physiology 1993;74:<br />
450–459.<br />
56. Schwarz L, Kindermann W. Beta-endorphin, adrenocorticotropic<br />
hormone, cortisol and catecholamines during aerobic<br />
and anaerobic exercise. European Journal of Applied<br />
Physiology and Occupational Physiology 1990;61:165–171.<br />
57. Schwarz L, Kindermann W. Changes in beta-endorphin<br />
levels in <strong>response</strong> <strong>to</strong> aerobic and anaerobic exercise. Sports<br />
Medicine 1992;13:25–36.<br />
58. Guskiewicz KM, McCrea M, Marshall SW, Cantu RC,<br />
Randolph C, Barr W, et al. Cumulative effects associated<br />
with recurrent <strong>concussion</strong> in collegiate football players: The<br />
NCAA Concussion Study. JAMA: The Journal of the<br />
American Medical Association 2003;290:2549–2555.<br />
59. Kristman VL, Ta<strong>to</strong>r CH, Kreiger N, Richards D,<br />
Mainwaring L, Jaglal S, et al. Does the apolipoprotein<br />
epsilon 4 allele predispose varsity athletes <strong>to</strong> <strong>concussion</strong>? A<br />
prospective cohort study. Clinical Journal of Sport Medicine<br />
2008;18:322–328.<br />
60. Iverson GL, Gaetz M, Lovell MR, Collins MW. Cumulative<br />
effects of <strong>concussion</strong> in amateur athletes. Brain Injury<br />
2004;18:433–443.<br />
61. Reeves DL, Winter KP, Bleiberg J, Kane RL. ANAM<br />
genogram: His<strong>to</strong>rical perspectives, description, and current<br />
endeavors. Archives of Clinical Neuropsychology<br />
2007;22(Suppl 1):S15–S37.<br />
62. Nixon H. A social network analysis of influences on athletes<br />
<strong>to</strong> play with pain and injuries. Journal of Sport and Social<br />
Issues 1992;16:127–135.<br />
63. Driver S, Ede A. Impact of physical activity on mood after<br />
TBI. Brain Injury 2009;23:203–212.