New Technique for Anal Fistula Showing Success - Cook Medical
New Technique for Anal Fistula Showing Success - Cook Medical
New Technique for Anal Fistula Showing Success - Cook Medical

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
This monograph is designed to be<br />
a summary of in<strong>for</strong>mation. While it is<br />
detailed, it is not an exhaustive clinical<br />
review. McMahon Publishing Group,<br />
<strong>Cook</strong>, and the authors neither affirm<br />
nor deny the accuracy of the in<strong>for</strong>mation<br />
contained herein. No liability will<br />
be assumed <strong>for</strong> the use of this educational<br />
review, and the absence of typographical<br />
errors is not guaranteed.<br />
Readers are strongly urged to consult<br />
any relevant primary literature. Copyright<br />
© 2006, McMahon Publishing<br />
Group, 545 West 45th Street, <strong>New</strong><br />
York, NY 10036. Printed in the USA. All<br />
rights reserved, including the right of<br />
reproduction, in whole or in part, in<br />
any <strong>for</strong>m.<br />
Distributed by McMahon<br />
Publishing Group<br />
<strong>New</strong> <strong>Technique</strong> <strong>for</strong> <strong>Anal</strong><br />
<strong>Fistula</strong> <strong>Showing</strong> <strong>Success</strong><br />
Early Data Indicate Closure Rates of 87%<br />
Over the decades, several techniques have<br />
been developed that allow surgeons to<br />
repair anal fistulas. These include conventional<br />
fistulotomy, endorectal/anal sliding flaps,<br />
the use of setons, fibrin glue, and most recently,<br />
the anal fistula plug.<br />
Just last year, the US Food and Drug Administration<br />
cleared the only device <strong>for</strong> treating<br />
anal fistulas—the Surgisis ® AFP <strong>Anal</strong> <strong>Fistula</strong><br />
plug (<strong>Cook</strong> Incorporated). Made from porcine<br />
small intestinal submucosa, the device is<br />
placed in the fistula tract where it serves as a<br />
bio-scaffold <strong>for</strong> native tissue regeneration. Data<br />
suggest that the technique is safe, easy to per<strong>for</strong>m,<br />
and has few complications.<br />
This Special Report, based on a satellite<br />
symposium conducted at the 2005 Clinical<br />
Congress of the American College of Surgeons,<br />
explores the scientific findings associated<br />
with the Surgisis AFP plug and other<br />
fistula repair techniques, and offers surgeons<br />
suggestions on selecting the best option <strong>for</strong><br />
their individual patients.<br />
Fistulotomy, Endorectal/<br />
<strong>Anal</strong> Sliding Flaps, and<br />
Seton Drainage<br />
Fistulotomy is the oldest and best studied<br />
of the anal fistula treatments. It also is considered<br />
the best option <strong>for</strong> superficial fistulas.<br />
This is exemplified by a recent report of a<br />
series of 101 patients requiring surgery <strong>for</strong> fistula<br />
in ano. 1 Of the 112 fistulas, 72 (64%) were<br />
intersphincteric, 33 (30%) were trans-sphincteric,<br />
6 (5%) were submucosal, and 1 (1%) was<br />
extrasphincteric. After a mean follow-up of 44<br />
weeks, 90 (89%) of the patients were cured.<br />
The 11 recurrences were attributed to wound<br />
BROUGHT TO YOU BY THE PUBLISHER OF<br />
GeneralSurgery<strong>New</strong>s.com<br />
MAY 2006<br />
bridging, misdiagnosis of the tract, or blindended<br />
fistulas. The average time to healing<br />
was 12 weeks <strong>for</strong> simple fistulotomy (range, 3-<br />
21 weeks), 16 weeks <strong>for</strong> seton (range, 4-28<br />
weeks), and 28 weeks <strong>for</strong> the Hanley procedure<br />
(range, 8-48 weeks). Four (4%) of the<br />
patients reported postoperative incontinence.<br />
Another recent study demonstrates fistulotomy<br />
is also efficacious when combined with<br />
primary sphincter reconstruction <strong>for</strong> the management<br />
of complex fistulas. 2 Only 2 of the 35<br />
patients studied had recurrences, and the<br />
patients’ mean incontinence score fell from<br />
7.2 to 2.0 after the procedure (P=0.008).<br />
However, Brad<strong>for</strong>d Sklow, MD, assistant<br />
professor, University of Utah School of Medicine,<br />
Colon and Rectal Surgery, Salt Lake City,<br />
noted at the symposium that fistulotomy is<br />
suboptimal <strong>for</strong> deep trans-sphincteric or<br />
suprasphincteric fistulas because of the<br />
increased likelihood of fecal incontinence. Dr.<br />
Sklow observed that patients’ distress over<br />
this type of incontinence is one of the greatest<br />
sources of litigation in colorectal surgery.<br />
A seton—a loop of flexible material placed<br />
along the track to maintain drainage <strong>for</strong> a period<br />
of time—is one alternative, and a team of<br />
Singapore surgeons has reported a 78% healing<br />
rate in a group of 37 patients in whom<br />
setons were used alone, without accompanying<br />
surgery. 3 However, studies have shown a<br />
36% to 50% incidence of fecal incontinence<br />
with stand-alone seton drainage. 4,5 As Dr.<br />
Sklow noted, the seton is also associated with<br />
pain and inconvenience <strong>for</strong> the patient; thus, it<br />
is generally recommended as a bridge to a<br />
more definitive procedure.<br />
The endorectal/anal sliding advancement<br />
flap is another consideration. There is potential<br />
<strong>for</strong> a 75% success rate as part of a staged
2<br />
approach to complex anal fistulas, 6 and up to an 83% success<br />
rate when per<strong>for</strong>med alone in selected simpler cases. 7<br />
However, this procedure is invasive and difficult to per<strong>for</strong>m<br />
posteriorly.<br />
Fibrin Glue<br />
When it was first cited regularly in the colorectal literature at<br />
the beginning of the 1990s, fibrin glue was reported to be superior<br />
to other approaches in the treatment of anal fistulas. The<br />
use of fibrin glue also is relatively simple and noninvasive.<br />
“Everyone thought this might be the holy grail <strong>for</strong> fistulas,”<br />
remarked Dr. Sklow, noting that early, short-term studies indicated<br />
very high closure rates, which made fibrin glue a serious<br />
contender <strong>for</strong> taking the top spot in surgeons’ treatment choices<br />
<strong>for</strong> anal fistulas.<br />
One of the earliest studies of fibrin glue in the treatment of<br />
anal fistulas was conducted by a team of Danish surgeons. 8 In<br />
a series of 23 patients, 12 patients (52%) showed complete and<br />
permanent fistula closure after 1 application of fibrin glue.<br />
Another 5 (22%) showed fistula healing after 2 or 3 attempts.<br />
The method failed in the remaining 6 patients (26%).<br />
Jose R. Cintron, MD, and his colleagues at the University of<br />
Illinois <strong>Medical</strong> Center, Chicago, had similar results in their<br />
study, published 9 years later in 2000. Patients treated with<br />
autologous fibrin glue (14/26) had a 54% complete-closure<br />
rate at 1 year, and there was a 64% rate among those treated<br />
with commercial fibrin sealant (34/53). 9 Moreover, Ian Lindsey,<br />
MD, and his team in Ox<strong>for</strong>d, England, completed a small randomized,<br />
controlled trial that revealed fibrin glue healed 50%<br />
(3/6) of simple fistulas and 69% (9/13) of complex fistulas. 10<br />
The respective numbers <strong>for</strong> fistulotomy were 100% (7/7) and<br />
13% (2/16). A higher closure rate of anal fistulas—85%<br />
(17/20)—was documented after a mean follow-up of 10 months<br />
by Stephen M. Sentovich, MD, and colleagues, in 2001. 11 However,<br />
Dr. Sentovich noted the healing rate dropped to 69%<br />
(33/48) after a mean follow-up of 22 months. 12<br />
Indeed, other research corroborates the finding that healing<br />
rates decrease as follow-up times increase. One randomized<br />
study of anal fistulas with a mean 27-month follow-up by a team<br />
that included Dr. Cintron and Herand Abcarian, MD, FACS, Turi<br />
Josefsen professor and chairman, Department of Surgery, University<br />
of Illinois College of Medicine at Chicago, revealed a<br />
40% (10/25) healing rate at an average of 27 months when surgical<br />
closure of the internal fistula opening was used. 13 However,<br />
there was only a 31% healing rate with the combination of<br />
surgical closure and fibrin sealant (8/26) and a 21% rate when<br />
fibrin glue and cefoxitin were used (5/24).<br />
Similarly, a team of St. Louis researchers documented a 38%<br />
success rate at an average of 26 months among complex-fistula<br />
patients given a first treatment with fibrin glue, and a 22%<br />
healing rate among those with previously treated fistulas. 14<br />
Most of the failures occurred within 3 months.<br />
“So glue may not be as great as we once thought, but it certainly<br />
has a role [in first-line treatment of anal fistulas],” Dr.<br />
Sklow concluded.<br />
Dr. Abcarian agreed.<br />
“Is glue past its due? No,” he said. “It has its place in the surgeon’s<br />
armamentarium. It is definitely ineffective in rectovaginal<br />
fistulas—[that is], it is ineffective in short, wide tracts. But it is<br />
much more effective in long, complex tracts, and may be used<br />
in Crohn’s disease. You have nothing to lose if you use it as<br />
first-line treatment. If it fails, repeat it once. If it fails again or the<br />
fistula recurs, move to endorectal advancement flap, dermalisland<br />
flap anoplasty, seton drainage, or the anal fistula plug.”<br />
David Armstrong, MD, program director, Georgia Colon and<br />
Rectal Surgical Clinic, Atlanta, is more wary of fibrin glue.<br />
“I think that half the time, the patients have extruded the glue<br />
be<strong>for</strong>e they even get in the car to drive home,” he told meeting<br />
attendees.<br />
<strong>New</strong>est Treatment <strong>for</strong> <strong>Anal</strong> <strong>Fistula</strong>s: the<br />
Surgisis AFP Plug<br />
The FDA cleared the Surgisis AFP plug, <strong>Cook</strong> Incorporated,<br />
Bloomington, Ind., March 9, 2005, as the first surgical device <strong>for</strong><br />
the repair of anal fistulas. The slender, cone-shaped device is<br />
made from porcine small intestinal submucosa. It is placed in the<br />
fistula channel, where it serves as a bio-scaffold <strong>for</strong> native tissue<br />
regeneration, and hence safely closes the fistula tract. Some surgeons<br />
have been using the Surgisis AFP plug <strong>for</strong> as long as 4<br />
years and appear to be very satisfied with it.<br />
Dr. Sklow was highly involved in the development of the Surgisis<br />
AFP plug. He has been using it since April 2002, when the<br />
device was in its earliest <strong>for</strong>m—he rolled a sheet of porcine material<br />
be<strong>for</strong>e insertion into the fistula. At the American Society of<br />
Colon and Rectal Surgeons’ 2004 annual meeting, Dr. Sklow<br />
and his colleagues reported on the rolled <strong>for</strong>m of the plug in 17<br />
patients. 15 The patients were treated between April 2002 and<br />
May 2003, their average age at diagnosis was 53.8 years<br />
(range, 28-79 years), and 14 (82%) were men. One of the subjects<br />
had Crohn’s disease, another had ulcerative colitis, and<br />
one more had a restorative proctocolectomy <strong>for</strong> ulcerative colitis.<br />
Sixteen of the 18 simple or complex fistulas (88.9%) were fistulas<br />
in ano, while 1 (5.6%) was a pouch-cutaneous fistula, and<br />
the remaining fistula (5.6%) was of the recto-pelvic <strong>for</strong>m. There<br />
had been previous attempts to close 5 of the fistulas (27.8%).<br />
The mean fistula length was 5.9 cm (range, 3-10 cm).<br />
The investigators documented a 61% closure rate (11/18) of<br />
the patients’ after an average of 12 months. Four of the patients<br />
(24%) required only local anesthesia, 11 (65%) required spinal<br />
anesthesia, and the remaining 2 (12%) were given general<br />
anesthesia.<br />
Of the fistulas, 13 (72%) were closed with insertion of the<br />
plug combined with closure of the internal opening with<br />
sutures. Seven of these patients (54%) successfully healed.<br />
The remaining 5 involved using the plug together with an<br />
advancement flap, after failure of the internal opening to close<br />
with sutures. All 5 were posterior midline fistulas. Four of these<br />
5 fistulas (80%) healed. Four of the successfully healed<br />
patients had failed previous surgical attempts at closure. One<br />
patient required an additional surgical procedure <strong>for</strong> a second<br />
missed fistula tract. The average time to closure was 4.9 weeks<br />
(range, 2-9 weeks). There was only 1 complication: a patient<br />
with Crohn’s disease developed an abscess at the external<br />
opening. The abscess was drained, and the fistula healed.<br />
The overall rate of closure after the first attempt at plug<br />
placement was 44% (8/18). Dr. Sklow explained that this low<br />
rate can be partly explained by the fact that 3 of the patients<br />
whose fistulas failed to heal after the first attempt should not<br />
have been given the Surgisis AFP plug because they had short,<br />
superficial fistulas. The explanation <strong>for</strong> most of the other failures<br />
was surgeon technique; it should be noted that these surgeons<br />
were early in the learning curve.<br />
“The installation of the Surgisis AFP plug is easy to per<strong>for</strong>m,<br />
safe, noninvasive, and associated with few complications and<br />
minimal discom<strong>for</strong>t <strong>for</strong> the patient,” Dr. Sklow said. “It certainly<br />
can be repeated if it fails initially and may be the procedure of<br />
choice <strong>for</strong> reoperative complex fistulas. Moreover, the commercially<br />
available conical shape may yield superior results.”
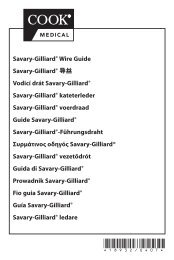
Surgisis ® AFP <br />
<strong>Anal</strong> <strong>Fistula</strong> Plug.<br />
Photo courtesy of <strong>Cook</strong> Biotech, Inc.<br />
The plug is rehydrated<br />
and inserted into the<br />
primary opening until<br />
resistance is first met.<br />
The excess plug is<br />
trimmed at the level of the<br />
primary opening and<br />
sutured in place with a<br />
deep figure-of-eight suture,<br />
using 2-0 Vicryl. It is<br />
essential to use a deep,<br />
secure suture at the<br />
primary opening to prevent<br />
extrusion of the plug.<br />
The plug undergoes<br />
resorption and remodeling<br />
into the native tissue, and<br />
six weeks later the fistula<br />
is firmly closed.<br />
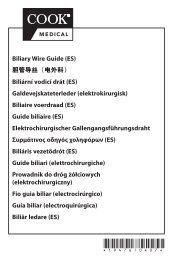
Photos courtesy of David N. Armstrong, MD.<br />
Multiple perianal fistulas<br />
and extensive perianal<br />
induration after multiple<br />
(failed) procedures (see<br />
radial incision in the right<br />
gluteal region). Setons are<br />
inserted to decrease the<br />
induration, and to<br />
“mature” the fistula tracts.<br />
Six weeks later, the<br />
induration has resolved,<br />
and the patient returns <strong>for</strong><br />
surgery <strong>for</strong> definitive fistula<br />
closure. All five secondary<br />
openings and fistula tracts<br />
were found to arise from<br />
the inner (primary) opening,<br />
which was closed<br />
using one fistula plug.<br />
Six weeks following<br />
surgery, all drainage had<br />
resolved; all fistula tracts<br />
are closed.<br />
Photos courtesy of David N. Armstrong, MD.<br />
The next step was a prospective comparison of the Surgisis<br />
AFP plug to fibrin glue <strong>for</strong> the closure of anal fistulas, undertaken<br />
by Dr. Armstrong and his team. They have been using the<br />
Surgisis AFP plug <strong>for</strong> more than 2 years <strong>for</strong> complex fistulas<br />
that have failed at least 1 previous attempt at closure.<br />
“We were exploring ways to work with patients with these<br />
complex fistulas,” explained Dr. Armstrong. “We decided on the<br />
Surgisis AFP plug because it seemed like it was made from an<br />
ideal material. It comes from porcine small intestinal submucosa—which<br />
is very similar to the human equivalent. There’s no<br />
<strong>for</strong>eign-body reaction, [so] it allows tissue ingrowth and it’s<br />
resistant to infection.”<br />
Dr. Armstrong and his colleagues enrolled 25 patients in a<br />
prospective trial. The team used the Surgisis AFP plug on 15<br />
patients and treated 10 with fibrin glue. Patients with Crohn’s<br />
disease were excluded from the study. There were no significant<br />
differences between the 2 groups in average age, number<br />
of men and women, number of prior fistula surgeries, or number<br />
of secondary fistula openings. All of the patients underwent<br />
mechanical bowel preparation accompanied by application of<br />
enteric antibiotics.<br />
Of the 15 patients treated with the Surgisis AFP plug, 13<br />
(87%) had complete closure of all fistula tracts. Only 4 patients<br />
treated with fibrin glue (40%) showed complete closure of all<br />
fistula tracts (P
4<br />
Table. Dos and Don’ts of the Surgisis AFP Plug <strong>Technique</strong><br />
DOs<br />
Rehydrate the plug <strong>for</strong> 5 minutes in saline.<br />
Use a 2-0 Vicryl suture.<br />
Insert a figure-of-eight suture through the primary opening, deep to<br />
the internal sphincter and try to get another 1 or 2 bites of the<br />
plug’s head.<br />
Advise patients to avoid strenuous activity <strong>for</strong> at least 2 weeks after<br />
the procedure.<br />
DON’Ts<br />
Don’t mechanically debride the fistula tract in such a way that would<br />
likely make the tract wider and harder to close.<br />
Don’t use the entire plug. Pull the plug into the fistula tract until<br />
resistance is first met, and trim the excess plug at the level of the<br />
primary opening. If the primary opening is too large, insert a seton<br />
<strong>for</strong> 6 to 8 weeks to narrow the tract and “mature” the fistula.<br />
Don’t leave any of the plug’s head exposed. Pull the plug into the<br />
tract just deep to the primary opening.<br />
Don’t close the secondary opening. Suture the end of the plug to<br />
the edge of the secondary opening to secure tip. This will help<br />
prevent a closed space infection.<br />
Suture a 6-inch tail to the tip of the plug and cut the excess.<br />
This helps prevent the tie from slipping off as the plug is pulled<br />
into the tract. Pull the plug into the primary opening until resistance<br />
is met. This can be done by a variety of means, such as<br />
tying the tail of the suture to the fistula probe. If there is already<br />
an indwelling seton in the tract, the tail of the suture can be tied<br />
to the seton, which is then cut and used to pull the plug into the<br />
primary opening of the tract. The “cut seton” method is very<br />
simple and straight<strong>for</strong>ward, and avoids having to find the primary<br />
opening again.<br />
The surgeon notes where the plug enters the primary opening.<br />
The plug is withdrawn several millimeters and the excess is<br />
trimmed. It is not unusual to trim as much as half the length of<br />
the plug, as the plugs are oversized.<br />
A 2-0 Vicryl suture is inserted into the head of the plug. The<br />
suture is then tied, leaving a 6-inch tail that will later be used<br />
to close the primary opening. This is best done under direct<br />
visualization to ensure the surgeon gets a good bite of the<br />
plug. The plug is pulled back into the tract, just deep to the<br />
primary opening. No part of the plug is left exposed. A figure-<br />
References<br />
1. Gonzalez-Ruiz C, Kaiser AM, Vukasin P, et al. Intraoperative<br />
physical diagnosis in the management of<br />
anal fistula. Am Surg. 2006;72:11-15.<br />
2. Perez F, Arroyo A, Serrano P, et al. Fistulotomy with<br />
primary sphincter reconstruction in the management<br />
of complex fistula-in-ano: prospective study of<br />
clinical and manometric results. J Am Coll Surg.<br />
2005;200:897-903.<br />
3. Theerapol A, So BY, Ngoi SS. Routine use of setons<br />
<strong>for</strong> the treatment of anal fistulae. Singapore Med J.<br />
2002;43:305-307.<br />
4. Hasegawa H, Radley S, Keighley MR. Long-term<br />
results of cutting seton fistulotomy. Acta Chir Iugosl.<br />
2000;47(suppl 1):19-21.<br />
5. Joy HA, Williams JG. The outcome of surgery <strong>for</strong><br />
complex anal fistula. Colorectal Dis. 2002;4:<br />
254-261.<br />
6. van der Hagen SJ, Baeten CG, Soeters PB, et al.<br />
Staged mucosal advancement flap <strong>for</strong> the treatment<br />
of complex anal fistulas: pretreatment with<br />
noncutting setons and in case of recurrent multiple<br />
abscesses a diverting stoma. Colorectal Dis.<br />
of-eight suture is inserted through the primary opening, deep<br />
to the internal sphincter, getting another 1 or 2 bites of the<br />
plug’s head. Resistance is felt when the suture passes<br />
through the plug. Finally, the primary opening is closed over<br />
the plug’s head by tying the suture to the 6-inch tail. This<br />
buries the head of the plug, closes the primary opening and<br />
secures the head of the plug deep to the primary opening to<br />
prevent extrusion.<br />
Dr. Armstrong emphasized the need <strong>for</strong> a deep suture to<br />
secure the head of the plug because of the high pressures that<br />
are generated in the pelvic floor during straining and exercise.<br />
“This has to be a real stitch,” he said. “You’ve got to get a<br />
good, solid, deep bite through the internal sphincter, and also<br />
through the head of the plug and out through the other side of<br />
the internal sphincter. You want to try and stitch this plug so it’s<br />
deep to the internal opening. You need to bury it. At the end of<br />
the procedure, you don’t want to see any plug.”<br />
The tip of the plug is sutured to the edge of the secondary<br />
opening and the excess is trimmed at skin level. The secondary<br />
opening should not be completely closed, as this will<br />
prevent drainage from the fistula tract, and possibly result in an<br />
abscess. Some drainage from the tract generally persists <strong>for</strong> 2<br />
to 4 weeks after the procedure—sometimes longer—as the plug<br />
undergoes reabsorption and remodeling into native tissue. As<br />
the fistula closes, the drainage decreases and eventually dries<br />
up. This is more a biological closure of the fistula than a<br />
mechanical closure, Dr. Armstrong explained. After the procedure,<br />
patients should be told to avoid any strenuous activity <strong>for</strong><br />
at least 2 weeks, bathe standing up (they should not sit in the<br />
bathtub) 2 or 3 times a day, and apply topical 10% metronidazole<br />
externally to help prevent any septic complications. They<br />
should also be instructed to avoid straining during bowel movements—taking<br />
a stool softener will help—and be instructed to<br />
eat a high fiber diet. Patients are reviewed in the office 2 to 4<br />
weeks after the procedure.<br />
Conclusion<br />
2005;7:513-518.<br />
7. Dixon M, Root J, Grant S, et al. Endorectal flap<br />
advancement repair is an effective treatment <strong>for</strong><br />
selected patients with anorectal fistulas. Am Surg.<br />
2004;70:925-927.<br />
8. Hjortrup A, Moesgaard F, Kjaergard J. Fibrin adhesive<br />
in the treatment of perianal fistulas. Dis Colon<br />
Rectum. 1991;34:752-754.<br />
9. Cintron JR, Park JJ, Orsay CP, et al. Repair of fistulas-in-ano<br />
using fibrin adhesive: Long-term followup.<br />
Dis Colon Rectum. 2000;43:944-949.<br />
10. Lindsey I, Smilgin-Humphreys MM, Cunningham C,<br />
et al. A randomized, controlled trial of fibrin glue vs.<br />
conventional treatment <strong>for</strong> anal fistula. Dis Colon<br />
Rectum. 2002;45:1608-1615.<br />
11. Sentovich SM. Fibrin glue <strong>for</strong> all anal fistulas. J Gastrointest<br />
Surg. 2001;5:158-161.<br />
12. Sentovich SM. Fibrin glue <strong>for</strong> anal fistulas: long-term<br />
results. Dis Colon Rectum. 2003;46:498-502.<br />
13. Singer M, Cintron J, Nelson R, et al. Treatment of fistulas-in-ano<br />
with fibrin sealant in combination with<br />
Colorectal surgeons have several options <strong>for</strong> treating simple<br />
and complex fistulas. The most common procedure remains fistulotomy,<br />
although fibrin glue has a role in long, complex tracts<br />
and Crohn’s disease. The Surgisis AFP plug is gaining notable<br />
favor <strong>for</strong> complex fistulas and repeat surgery. By following the<br />
procedure <strong>for</strong> insertion of the plugs advised by field leaders,<br />
surgeons can have considerable success in difficult patients.<br />
intra-adhesive antibiotics and/or surgical closure of<br />
the internal fistula opening. Dis Colon Rectum.<br />
2005;48:799-808.<br />
14. Loungnarath R, Dietz DW, Mutch MG, et al. Fibrin<br />
glue treatment of complex anal fistulas has low success<br />
rate. Dis Colon Rectum. 2004;47:432-436.<br />
15. Robb BW, Vogler SA, Nussbaum MN, et al. Early<br />
experience using porcine small intestinal submucosa<br />
to repair fistulas-in-ano. Paper presented at:<br />
American Society of Colon and Rectal Surgery<br />
2004 annual meeting; May 8-13, 2004;<br />
Dallas,Texas. Abstract P9.<br />
16. Johnson EK, Gaw JU, Armstrong D. Efficacy of<br />
biodegradable “collagen plug” versus fibrin glue in<br />
closure of anorectal fistulas. Paper presented at:<br />
American Society of Colon and Rectal Surgery<br />
2005 annual meeting; April 30-May 5, 2005;<br />
Philadelphia, Pa. Abstract S51.<br />
17. Johnson EK, Gaw JU, Armstrong DN. Efficacy of<br />
anal fistula plug vs. fibrin glue in closure of anorectal<br />
fistulas. Dis Colon Rectum. 2006 Jan. 29 [Epub<br />
ahead of print].<br />
SR604