Doença do refluxo gastroesofágico e sua relação com a asma
Doença do refluxo gastroesofágico e sua relação com a asma
Doença do refluxo gastroesofágico e sua relação com a asma

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
18 Rev. bras. alerg. imunopatol. – Vol. 30, Nº 1, 2007 RGE e <strong>asma</strong><br />
na área pediátrica têm mostra<strong>do</strong> resulta<strong>do</strong>s se-<br />
Estu<strong>do</strong>s<br />
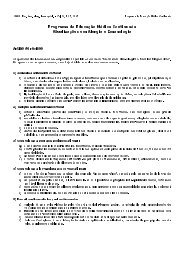
(tabela 3). Após o tratamento de crianças e<br />
melhantes<br />
asmáticos <strong>com</strong> DRGE, utilizan<strong>do</strong> tratamento<br />
a<strong>do</strong>lescentes<br />
(bloquea<strong>do</strong>r H2, agente procinético, mudança <strong>do</strong><br />
clínico<br />
hábito de vida ou uma associação de medicações) ou trata-<br />
cirúrgico, esses pacientes apresentaram redução <strong>do</strong><br />
mento<br />
de sintomas noturnos escore 63 sintomas pulmona-<br />
,<br />
res 32,56,57,63 menor necessidade de medicação para as-<br />
,<br />
ma 32,56,57 melhora <strong>do</strong>s índices da pHmetria intra-esofági-<br />
e<br />
Tabela 3 - Ensaios clínicos de terapia anti-<strong>refluxo</strong> <strong>gastroesofágico</strong> e resposta terapêutica em pacientes pediátricos asmáticos<br />
Autores<br />
(ano)<br />
et al Andze<br />
(1991)<br />
et al<br />
Gustafsson<br />
(1992)<br />
et al Tucci<br />
(1993)<br />
et al<br />
Khoshoo<br />
(2003)<br />
Tratamento<br />
(duração)<br />
proposto<br />
clínico* ou cirúrgico<br />
Ranitidina<br />
semanas)<br />
(4<br />
Cisaprida<br />
meses) (3<br />
(Cisaprida ou<br />
clínico<br />
/<br />
Metoclopramida)<br />
cirúrgico<br />
ca 47 .<br />
de Número<br />
pacientes<br />
105<br />
Resposta terapêutica<br />
tratamento clínico<br />
69%<br />
tratamento cirúrgico<br />
27%<br />
melhora <strong>do</strong>s sintomas e redução de<br />
-<br />
medicações<br />
37 30% redução <strong>do</strong>s sintomas noturnos<br />
11<br />
(clínico)<br />
18<br />
(cirúrgico)<br />
9<br />
redução <strong>do</strong>s sintomas e de uso de<br />
81,8%<br />
medicações<br />
50% redução <strong>do</strong> uso de medicações<br />
* tratamento clínico: medidas posturais, dieta, medicamentoso (metoclopramida, cisaprida, <strong>do</strong>mperi<strong>do</strong>na e /ou antiáci<strong>do</strong>s).<br />
<strong>relação</strong> entre <strong>do</strong>ença <strong>do</strong> <strong>refluxo</strong> <strong>gastroesofágico</strong> e as-<br />
A<br />
ainda não está plenamente conhecida. Os estu<strong>do</strong>s reama<br />
mostram alta prevalência de RGE liza<strong>do</strong>s 47,56,57 pacien-<br />
em<br />
<strong>com</strong> <strong>asma</strong> grave ou moderada, ou ainda naqueles clastes<br />
<strong>com</strong>o porta<strong>do</strong>res de <strong>asma</strong> de difícil controle. Estes<br />
sifica<strong>do</strong>s<br />
sugerem uma possível contribuição <strong>do</strong> RGE no de-<br />
estu<strong>do</strong>s<br />
ou na exacerbação <strong>do</strong>s sintomas da <strong>asma</strong>,<br />
sencadeamento<br />
alguns ensaios clínicos mostram a melhora <strong>do</strong>s sinto-<br />
pois<br />
da <strong>asma</strong> ou redução <strong>do</strong> uso de medicação durante e<br />
mas<br />
o tratamento da DRGE após 57,65 .<br />
disso, alguns estu<strong>do</strong>s tentam estabelecer os meca-<br />
Além<br />
que levam a broncoconstrição, pela sensibilização<br />
nismos<br />
ao áci<strong>do</strong> em esôfago distal esofágica 28,43,59 aspiração <strong>do</strong><br />
ou<br />
gástrico conteú<strong>do</strong> 60-62 .<br />
conclusão, nesta revisão foram aborda<strong>do</strong>s os princi-<br />
Em<br />
mecanismos patofisiológicos que decorrem da presenpais<br />
da DRGE, os méto<strong>do</strong>s laboratoriais disponíveis para a<br />
ça<br />
investigação, bem <strong>com</strong>o os questionamentos sobre os<br />
<strong>sua</strong><br />
mesmos.<br />
Referências<br />
Orenstein SR, Izadnia F, Khan S. Gastroesophageal reflux di-<br />
1.<br />
in children. Gastroenterol Clin North Am 1999; 28:947-<br />
sease<br />
69.<br />
Vandenplas Y, Sacré-Smitis L. Continuos 24-hour esophageal<br />
2.<br />
monitoring in 285 asymptomatic infants 0-15 months old. J<br />
pH<br />
Gastroenterol Nutr 1987;6: 220-4.<br />
Pediatr<br />
Gustafsson PM, Tibbling L. 24-hour oesophageal two-level pH<br />
3.<br />
in healthy children and a<strong>do</strong>lescents. Scand J Gas-<br />
monitoring<br />
1988; 23:91-4.<br />
troenterol<br />
Vandenplas Y, Goyvaerts H, Helven R, Sacre L. Gastroesopha-<br />
4.<br />
reflux, as measured by 24-hour pH monitoring, in 509<br />
geal<br />
infants screened for risk of sudden infant death syn-<br />
healthy<br />
Pediatrics 1991; 88:834-40.<br />
drome.<br />
Jamieson JR, Stein HJ, DeMeester TR, Bonavina L, Schwizer W,<br />
5.<br />
RA et al. Ambulatory 24-h esophageal pH monitoring:<br />
Hinder<br />
values, optimal thresholds, specificity, sensitivity and<br />
normal<br />
reproducibility. Am J Gastroenterol 1992; 87:1102-11.<br />
Richter JE, Laurence AB, DeMeester TR, Wu WC. Normal 24-hr<br />
6.<br />
esophageal pH values. Influence of study center,<br />
ambulatory<br />
electrode, age and gender. Dig Dis Sci 1992; 37:849-56.<br />
pH<br />
Ru<strong>do</strong>lph CD, Mazur LJ, Liptak GS, Baker RD. Guidelines for<br />
7.<br />
and treatment of gastroesophageal reflux in infants<br />
evaluation<br />
children. Re<strong>com</strong>mendations of the North American Society<br />
and<br />
Pediatric Gastroenterology and Nutrition. J Pediatric Gastro-<br />
for<br />
Nutr 2001; 32:S1-S32.<br />
enterol<br />
Ferreira CT, Carvalho E. Refluxo <strong>gastroesofágico</strong>. In: Ferreira<br />
8.<br />
Carvalho E, Silva LR. Gastroenterologia e hepatologia em<br />
CT,<br />
Diagnóstico e tratamento. 1 ed., São Paulo: Medsi,<br />
pediatria.<br />
2003:3-29.<br />
Vandenplas Y, Hassall E. Mechanisms of gastroesophageal re-<br />
9.<br />
and gastroesophageal reflux disease. J Pediatr Gastroenteflux<br />
Nutr 2002; 35:119-36.<br />
rol<br />
Little JP, Matthews BL, Glock MS, Koufman JA, Reboussin DM,<br />
10.<br />
CJ et al. Extraesophageal pediatric reflux: 24-hour<br />
Loughlin<br />
pH monitoring in 222 children. Ann Otol Rhinol<br />
<strong>do</strong>uble-probe<br />
1997; 106:S1-S15.<br />
Laryngol<br />
Vijayaratnam V, Lin CH, Simpson P, Tolia V. Lack of significant<br />
11.<br />
e esophageal acid reflux in infants presenting with<br />
proximal<br />
symptoms. Pediatr Pulmonol 1999;27:231-5.<br />
respiratory<br />
Sheikh S, Goldsmith LJ, Howell L, Hamlyn J, Eid N. Lung func-<br />
12.<br />
in infants with wheezing and gastroesophageal reflux. Petion<br />
Pulmonol 1999; 27:236-41.<br />
diatr<br />
Zielinska I, Czerwionka-Szaflarska M. Assessment of value of<br />
13.<br />
results in diagnostics of gastroesophageal reflux as a<br />
pHmetry<br />
of obstructive bronchitis in children. Med Sci Monit<br />
cause<br />
8:169-74.<br />
2002;<br />
Katz PO. Ambulatory esophageal and hypopharyngeal pH mo-<br />
14.<br />
in patients with hoarseness. Am J Gastroenterol 1990;<br />
nitoring<br />
85:38-40.<br />
Jacob P, Kahrilas PJ, Herzon G. Proximal esophageal pH-metry<br />
15.<br />
patients with reflux laryngitis’. Gastroenterology 1991; 100:<br />
in<br />
305-10.<br />
Matthews BL, Little JP, McGuirt Jr WF, Koufman JA. Reflux in<br />
16.<br />
with laryngomalacia: results of 24-hour <strong>do</strong>uble-probe<br />
infants<br />
monitoring. Arch Otolaringol Head Neck Surg 1999; 120:<br />
pH<br />
860-4.<br />
Rozmanic V, Velepic M, Ahel V, Bonifacic D, Velepic M. Prolon-<br />
17.<br />
esophageal pH monitoring in the evaluation of gastroesoged<br />
reflux in children with chronic tubotympanal disorders.<br />
phageal<br />
Pediatr Gastroenterol Nutr 2002; 34:278-80.<br />
J<br />
Monteiro VRSG, Sdepanian VL, Wecky L, Fagundes-Neto, U,<br />
18.<br />
Morais MB. Twenty-four hour esophageal pH monitoring in