sternocostoclavicular hyperostosis in sapho-syndrome - rbrs
sternocostoclavicular hyperostosis in sapho-syndrome - rbrs
sternocostoclavicular hyperostosis in sapho-syndrome - rbrs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
JBR–BTR, 2005, 88: 158-159.<br />
STERNOCOSTOCLAVICULAR HYPEROSTOSIS IN SAPHO-SYNDROME<br />
M. Vermaat, A.M. De Schepper, J.L. Bloem 1<br />
Key-word: Bones, <strong>in</strong>fection<br />
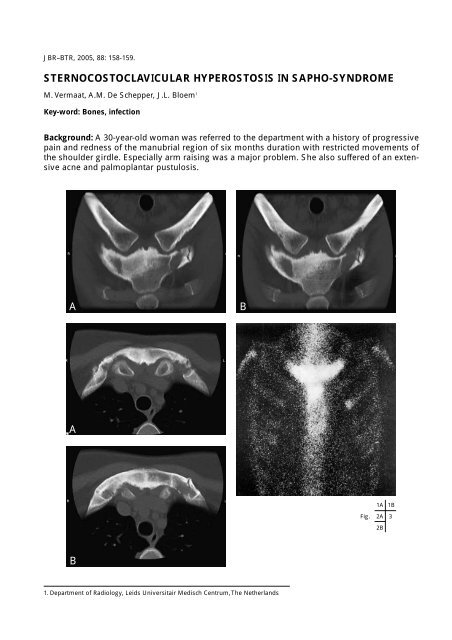
Background: A 30-year-old woman was referred to the department with a history of progressive<br />
pa<strong>in</strong> and redness of the manubrial region of six months duration with restricted movements of<br />
the shoulder girdle. Especially arm rais<strong>in</strong>g was a major problem. She also suffered of an extensive<br />
acne and palmoplantar pustulosis.<br />
A<br />
A<br />
B<br />
1. Department of Radiology, Leids Universitair Medisch Centrum, The Netherlands<br />
B<br />
1A 1B<br />
Fig. 2A<br />
2B<br />
3
Work-up<br />
Coronal CT scan through the sterno-costo-clavicular<br />
region (Fig. 1 A,B) shows sclerosis <strong>in</strong> the<br />
manubrium (the right side be<strong>in</strong>g more affected)<br />
and manubriocostal ossification.<br />
Transverse CT scan through the sterno-costoclavicular<br />
region (Fig. 2 A,B) shows pronounced<br />
sclerosis (<strong>in</strong>creased attenuation) <strong>in</strong> the manubrium<br />
and manubriocostal synchondrosis with foci of<br />
ossification. Both clavicles have a normal radiological<br />
aspect.<br />
Bone sc<strong>in</strong>tigraphy (Fig. 3) demonstrates a typical<br />
“bull head “ pattern of <strong>in</strong>tense radionuclide<br />
uptake <strong>in</strong> the sterno-costo-clavicular region.<br />
Radiological diagnosis<br />
The radiological f<strong>in</strong>d<strong>in</strong>gs <strong>in</strong> association with the<br />
dermatological abnormalities are consistent with<br />
the diagnosis <strong>sternocostoclavicular</strong> <strong>hyperostosis</strong><br />
as part of the SAPHO - <strong>syndrome</strong>.<br />
Discussion<br />
STERNOCOSTOCLAVICULAR HYPEROSTOSIS IN SAPHO-SYNDROME — VERMAAT et al. 159<br />
The Sapho <strong>syndrome</strong> <strong>in</strong>cludes osteoarticular<br />
manifestations of synovitis, osteitis and <strong>hyperostosis</strong><br />
which may be associated with sk<strong>in</strong> lesions,<br />
ma<strong>in</strong>ly acne and palmoplantar pustulosis. SAPHO<br />
stands for synovitis, acne, pustulosis, <strong>hyperostosis</strong><br />
and osteitis. The etiology and pathogenesis are<br />
unclear. A faulty or atypical immune response to<br />
viral or bacterial antigens is mentioned. The major<br />
site of <strong>in</strong>volvement is the anterior chest wall with<br />
less common <strong>in</strong>volvement of the sp<strong>in</strong>e, long<br />
bones, small bones and large and small jo<strong>in</strong>ts. All<br />
the components of the anterior chestwall can be<br />
<strong>in</strong>volved, particularly the sternoclavicular, the<br />
upper costosternal, the costochondral and the<br />
manubriosternal junctions. The earliest cl<strong>in</strong>ical<br />
signs of <strong>sternocostoclavicular</strong> <strong>hyperostosis</strong> (SCCH)<br />
are swell<strong>in</strong>g and redness, ma<strong>in</strong>ly localised to the<br />
manubrial region. Pa<strong>in</strong>, swell<strong>in</strong>g and redness are<br />
due to a destructive <strong>in</strong>flammatory process which<br />
may spread to the clavicles and the anterior rib<br />
segments. It <strong>in</strong>volves the cortex and the medullary<br />
canal with associated endosteal and periosteal<br />
thicken<strong>in</strong>g. Reactive reparation and ankylos<strong>in</strong>g<br />
ossification lead to the radiological f<strong>in</strong>d<strong>in</strong>gs. Jo<strong>in</strong>t<br />
erosions are frequently seen as a result of the primary<br />
arthritis or an extension of the osteitis.<br />
Histological exam<strong>in</strong>ation shows a non-specific<br />
chronic <strong>in</strong>flammatory reaction. Nuclear medic<strong>in</strong>e<br />
is a highly specific tool <strong>in</strong> the diagnosis of SCCH.<br />
The characteristic “bull head” pattern of <strong>in</strong>tense<br />
radionuclide uptake is a specific sign and confirms<br />
the diagnosis. The radiologist plays a key role <strong>in</strong><br />
the diagnosis. Osteomyelitis, osteosarcoma and<br />
Paget’s disease can have similar radiological features<br />
but dermatological abnormalities with typical<br />
bone lesions <strong>in</strong> characteristic target sites or<br />
bone sc<strong>in</strong>tigraphy with the presence of a bull’s<br />
head sign must set you on th<strong>in</strong>k<strong>in</strong>g.<br />
Bibliography<br />
1. Earwaker J.W.S., Cotten A.: SAPHO: <strong>syndrome</strong><br />
or concept? Imag<strong>in</strong>g f<strong>in</strong>d<strong>in</strong>gs. Skel Radiol, 2003,<br />
311-327.<br />
2. Freyschmidt J., Freischmidt G.: Pustulotic Arthroosteitis<br />
(PAO) (Chapter 3). In: Freischmidt J., ed.<br />
skibo- Diseases- Disorders affect<strong>in</strong>g the Sk<strong>in</strong> and<br />
Bones, Verlag Berl<strong>in</strong> Heidelberg: Spr<strong>in</strong>ger, 1999,<br />
101-110.