An overview of sexually transmitted diseases. Part III ... - Dermatology
An overview of sexually transmitted diseases. Part III ... - Dermatology
An overview of sexually transmitted diseases. Part III ... - Dermatology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
The HIV epidemic has drastically altered the medical<br />
community’s approach to <strong>sexually</strong> <strong>transmitted</strong><br />
<strong>diseases</strong> (STDs). For generations, multiple<br />
STDs occurred in individual patients. However, not<br />
until HIV did these infections interact so significantly<br />
with each other. Clinically, HIV can alter the presentation<br />
or treatments <strong>of</strong> other STDs as in, for example, a<br />
case <strong>of</strong> coexistent HIV and scabies. Conversely, an<br />
increasing recognition <strong>of</strong> the ways in which STDs influence<br />
HIV transmission has underscored the importance<br />
<strong>of</strong> early detection and treatment <strong>of</strong> all STDs. In 1998,<br />
the Centers for Disease Control and Prevention (CDC)<br />
published Guidelines for the Treatment <strong>of</strong> Sexually<br />
Transmitted Diseases, 1 and in addition the CDC published<br />
recommendations for the prevention <strong>of</strong> HIV<br />
through early detection and treatment <strong>of</strong> other STDs. 2<br />
From the Department <strong>of</strong> <strong>Dermatology</strong> at the University <strong>of</strong> Texas—<br />
Houston Health Science Center and St Joseph Hospital,<br />
Houston a ; the Department <strong>of</strong> <strong>Dermatology</strong> at the University <strong>of</strong><br />
Texas—Southwestern Medical School and Veterans Affairs<br />
Hospital, Dallas b ; and the Departments <strong>of</strong> <strong>Dermatology</strong>,<br />
Microbiology & Immunology and Internal Medicine at the<br />
University <strong>of</strong> Texas Medical Branch, Galveston. c<br />
Reprint requests: Stephen K. Tyring, MD, PhD, Department <strong>of</strong><br />
<strong>Dermatology</strong>, Route 1070, University <strong>of</strong> Texas Medical Branch,<br />
Galveston, TX 77555-1070. E-mail: styring@utmb.edu.<br />
16/2/105158<br />
doi:10.1067/mjd.2000.105158<br />
CONTINUING MEDICAL EDUCATION<br />
<strong>An</strong> <strong>overview</strong> <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>.<br />
<strong>Part</strong> <strong>III</strong>. Sexually <strong>transmitted</strong> <strong>diseases</strong> in<br />
HIV-infected patients<br />
Adam Czelusta, MD, a <strong>An</strong>gela Yen-Moore, MD, b Melody Van der Straten, MD, c<br />
Daniel Carrasco, MD, c and Stephen K. Tyring MD, PhD c Houston, Dallas, and Galveston, Texas<br />
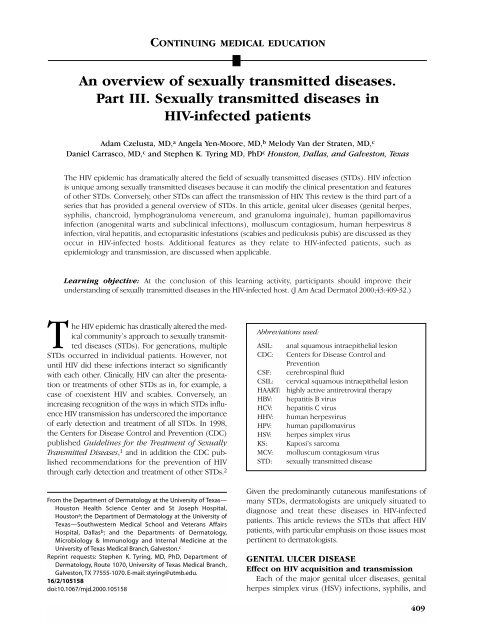
The HIV epidemic has dramatically altered the field <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong> (STDs). HIV infection<br />
is unique among <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong> because it can modify the clinical presentation and features<br />
<strong>of</strong> other STDs. Conversely, other STDs can affect the transmission <strong>of</strong> HIV. This review is the third part <strong>of</strong> a<br />
series that has provided a general <strong>overview</strong> <strong>of</strong> STDs. In this article, genital ulcer <strong>diseases</strong> (genital herpes,<br />
syphilis, chancroid, lymphogranuloma venereum, and granuloma inguinale), human papillomavirus<br />
infection (anogenital warts and subclinical infections), molluscum contagiosum, human herpesvirus 8<br />
infection, viral hepatitis, and ectoparasitic infestations (scabies and pediculosis pubis) are discussed as they<br />
occur in HIV-infected hosts. Additional features as they relate to HIV-infected patients, such as<br />
epidemiology and transmission, are discussed when applicable.<br />
Learning objective: At the conclusion <strong>of</strong> this learning activity, participants should improve their<br />
understanding <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong> in the HIV-infected host. (J Am Acad Dermatol 2000;43:409-32.)<br />
Abbreviations used:<br />
ASIL: anal squamous intraepithelial lesion<br />
CDC: Centers for Disease Control and<br />
Prevention<br />
CSF: cerebrospinal fluid<br />
CSIL: cervical squamous intraepithelial lesion<br />
HAART: highly active antiretroviral therapy<br />
HBV: hepatitis B virus<br />
HCV: hepatitis C virus<br />
HHV: human herpesvirus<br />
HPV: human papillomavirus<br />
HSV: herpes simplex virus<br />
KS: Kaposi’s sarcoma<br />
MCV: molluscum contagiosum virus<br />
STD: <strong>sexually</strong> <strong>transmitted</strong> disease<br />
Given the predominantly cutaneous manifestations <strong>of</strong><br />
many STDs, dermatologists are uniquely situated to<br />
diagnose and treat these <strong>diseases</strong> in HIV-infected<br />
patients. This article reviews the STDs that affect HIV<br />
patients, with particular emphasis on those issues most<br />
pertinent to dermatologists.<br />
GENITAL ULCER DISEASE<br />
Effect on HIV acquisition and transmission<br />
Each <strong>of</strong> the major genital ulcer <strong>diseases</strong>, genital<br />
herpes simplex virus (HSV) infections, syphilis, and<br />
409
410 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
chancroid, have been associated with an increased<br />
risk <strong>of</strong> acquiring and transmitting HIV. One estimation<br />
suggests that STDs increase the overall risk <strong>of</strong><br />
acquiring HIV about 3 to 5 times. 3 Cross-sectional<br />
studies performed in Nairobi, Kenya have consistently<br />
found that HIV seropositivity was more<br />
common in persons with either a history or clinical<br />
evidence <strong>of</strong> genital ulcer disease, 4-7 and one<br />
prospective study from this same region showed an<br />
increased risk <strong>of</strong> seroconversion in patients with<br />
genital ulcer disease. 8 Similarly, Telzak et al 9 found<br />
that 2.9% <strong>of</strong> men with genital ulcer disease turned<br />
HIV-positive, whereas only 1% <strong>of</strong> men without genital<br />
ulcer disease seroconverted. Clearly, a relationship<br />
between genital ulcer disease and HIV transmission<br />
exists; subsequently, prevention <strong>of</strong> genital ulcer<br />
disease should decrease transmission <strong>of</strong> HIV. A<br />
Tanzanian study showed that communities that<br />
improved their recognition and treatment <strong>of</strong> STDs<br />
saw a decrease in the incidence <strong>of</strong> HIV infection in<br />
their population. 10 This is the first documented<br />
intervention involving treatment <strong>of</strong> STDs that was<br />
associated with a decrease in HIV incidence in a<br />
defined population. Thus, through the early recognition<br />
and treatment <strong>of</strong> all STDs, including genital<br />
ulcer disease, HIV transmission can be reduced.<br />
Numerous studies have isolated HIV from genital<br />
ulcer exudates. 11-14 Mechanisms by which genital<br />
ulcer disease appear to facilitate HIV transmission<br />
have been suggested. Disruption <strong>of</strong> the genital<br />
mucosa is associated with the recruitment <strong>of</strong> inflammatory<br />
cells such as CD4 + T lymphocytes and<br />
macrophages. The presence <strong>of</strong> these cells can facilitate<br />
transmission <strong>of</strong> HIV virions from HIV-infected<br />
persons to uninfected persons or provide additional<br />
targets for HIV entry in HIV-negative persons who<br />
are being exposed to the virus. 14-17<br />
Studies implicating the specific agents <strong>of</strong> genital<br />
ulcer disease have focused mostly on genital herpes,<br />
syphilis, and chancroid. Several reports have shown an<br />
association between genital HSV lesions and the acquisition<br />
<strong>of</strong> HIV infection in the affected population.<br />
4,9,18-23 Keet et al 23 showed in a prospective<br />
cohort that pre-existing herpes simplex virus type 2<br />
(HSV-2) seropositivity was a predictor <strong>of</strong> HIV seroconversion.<br />
HIV virions have been shown in HSV ulcers, 24<br />
and in one study HIV RNA was isolated from herpetic<br />
lesions on 67% <strong>of</strong> the days that lesions were present. 13<br />
Similarly, arguments implicating syphilis and chancroid<br />
in the acquisition <strong>of</strong> HIV can be made. Two studies<br />
from Baltimore document strong associations<br />
between HIV seroconversion and either positive<br />
syphilis serology or a history <strong>of</strong> syphilis. 25,26 One<br />
cross-sectional study from Kenya found a similar association<br />
5 ; however, the difficulty in making this associ-<br />
ation statistically significant may reflect the difficulty<br />
in identifying cases <strong>of</strong> syphilis with active genital<br />
ulcers during the study. 8 <strong>An</strong> outbreak <strong>of</strong> chancroid in<br />
Jackson, Mississippi showed a strong association<br />
between this infection and HIV seropositivity, 27 and<br />
most <strong>of</strong> the ulcers in an aforementioned Kenyan<br />
study were due to chancroid and were associated<br />
with increased HIV seropositivity. 6 Lymphogranuloma<br />
venereum and granuloma inguinale are rare <strong>diseases</strong>,<br />
and, as such, they have not been extensively studied<br />
in relation to HIV transmission. Granuloma inguinale<br />
has been associated with a significant number <strong>of</strong> HIV<br />
infections, 28 and its eradication (in an effort to prevent<br />
HIV transmission) has been suggested. 29<br />
Clinical features and treatment<br />
Genital herpes. Genital herpes is the most common<br />
cause <strong>of</strong> genital ulceration worldwide, 30 and its<br />
association with HIV was noticed as early as 1981. 31<br />
Although genital herpes is most commonly caused<br />
by HSV-2, an increasing number <strong>of</strong> cases are suspected<br />
to be caused by HSV-1. 1,32 In HIV-infected<br />
patients, genital herpes can result in severe and atypical<br />
clinical presentations, and treatment may<br />
require increased doses <strong>of</strong> antiviral medications.<br />
Suppressive therapy for HSV appears to significantly<br />
improve survival in HIV-positive patients.<br />
Clinically, HIV-infected patients may experience<br />
an increased number and size <strong>of</strong> lesions in both primary<br />
and reactivated HSV infections as compared<br />
with HIV-uninfected patients. 31,33,34 The vesicles and<br />
ulcers are more painful and heal slower than those<br />
experienced by an immunocompetent host. 35 As<br />
CD4 cell counts drop and immunosuppression worsens,<br />
recurrent outbreaks increase in frequency and<br />
severity. 36,37 Chronic HSV-2 ulcers <strong>of</strong> more than 1<br />
month in duration are an AIDS-defining illness in<br />
HIV-infected patients. 38,39<br />
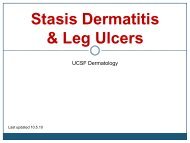
Atypical HSV presentations occur relatively <strong>of</strong>ten<br />
in HIV-infected patients. <strong>Part</strong>icularly severe lesions<br />
have been reported on patients’ lower backs, buttocks,<br />
or perianal regions, and these lesions may<br />
expand to 20 cm in diameter (Fig 1). 31,40 Such ulcers<br />
commonly become impetiginized and require intensive<br />
long-term therapy. 31 Several case reports<br />
describe HSV-2 presenting as hyperkeratotic verrucous<br />
lesions resembling condyloma in severely<br />
immunocompromised patients. 41-44 These masses<br />
can become large 41,43 and may represent concurrent<br />
HSV and cytomegalovirus infection. 44 A recent<br />
report describes a patient with a pseudotumor <strong>of</strong> the<br />
tongue that was discovered to be an atypical recurrence<br />
<strong>of</strong> HSV-2. 45 HSV may also cause esophagitis,<br />
hepatitis, pneumonitis, or life-threatening disseminated<br />
infections in AIDS patients. 46
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
Acyclovir, valacyclovir, and famciclovir are recognized<br />
by the CDC as appropriate therapies for primary<br />
or recurrent genital herpes in the HIV-infected<br />
patient. 1 As in the immunocompetent patient, therapy<br />
should start as soon as possible, preferably during<br />
the prodromal period. Therapy is then continued<br />
until clinical resolution is obtained. 1 For acyclovir<br />
and famciclovir, increased dosages above those recommended<br />
for immunocompetent persons may be<br />
required. For example, whereas the recommended<br />
oral dose <strong>of</strong> acyclovir is either 400 mg 3 times per<br />
day or 200 mg 5 times per day, regimens <strong>of</strong> 400 mg<br />
given 5 times per day have been useful in immunocompromised<br />
patients. 1 Likewise, famciclovir 250<br />
mg twice daily is recommended for suppression <strong>of</strong><br />
genital herpes in the immunocompetent person, but<br />
500 mg twice daily has been effective in decreasing<br />
both the rate <strong>of</strong> recurrences and the rate <strong>of</strong> subclinical<br />
shedding among HIV-seropositive persons. 47<br />
When given at doses <strong>of</strong> 8 g per day to markedly<br />
immunocompromised persons for suppression <strong>of</strong><br />
cytomegalovirus infections, valacyclovir was associated<br />
with either thrombotic thrombocytopenic purpura<br />
or the hemolytic uremic syndrome. 1,48,49 However, no<br />
cause-and-effect relationship was ascertained. When<br />
taken as a dose <strong>of</strong> 500 mg twice daily, valacyclovir<br />
appeared safe and effective for the suppression <strong>of</strong><br />
genital HSV in HIV-seropositive persons and was<br />
superior to acyclovir 400 mg twice daily. 50 Therefore<br />
acyclovir, valacyclovir, and famciclovir all appear useful<br />
for treatment and suppression <strong>of</strong> HSV in immunocompromised<br />
persons. 47-55<br />
Interestingly, acyclovir treatment <strong>of</strong> HSV infections<br />
in HIV-positive patients may <strong>of</strong>fer a significant<br />
survival benefit. Eight randomized controlled trials,<br />
combined in a meta-analysis, showed that patients<br />
treated with acyclovir had a significant survival<br />
advantage compared with those who went untreated.<br />
51 Two multicenter clinical trials noted that<br />
patients given acyclovir and zidovudine lived longer<br />
than those given only zidovudine. 56,57 These studies<br />
suggest that long-term suppressive acyclovir therapy<br />
prolongs survival in AIDS patients with extensive histories<br />
<strong>of</strong> HSV infections.<br />
The mechanism by which this occurs is unclear.<br />
Studies demonstrate that acute or reactivated HSV<br />
infection may stimulate HIV replication. 58-60<br />
Furthermore, Mole et al 61 documented increased<br />
plasma HIV viral loads in HIV patients experiencing<br />
an outbreak <strong>of</strong> HSV. By reducing or attenuating<br />
the occurrences <strong>of</strong> HSV outbreaks, acyclovir therapy<br />
may help reduce these deleterious effects <strong>of</strong><br />
the infections. Clearly, further investigation<br />
regarding this issue is required, as evidenced by<br />
the study <strong>of</strong> Gallant et al, 62 which found no asso-<br />
Czelusta, Yen-Moore, and Tyring 411<br />
Fig 1. HIV-positive patient. Large suprapubic ulcer due to<br />
HSV type 2.<br />
ciation between survival and acyclovir use in HIVinfected<br />
patients.<br />
A preliminary report from the CDC noted that<br />
6.4% <strong>of</strong> HSV isolates from 140 HIV-positive patients<br />
were resistant to acyclovir compared with less than<br />
1% <strong>of</strong> isolates from immunocompetent persons. 63<br />
Typically, resistance to acyclovir is also associated<br />
with resistance to the other thymidine kinase<br />
inhibitors. Resistance rates before the advent <strong>of</strong><br />
these medicines appear similar to those currently<br />
seen in the population. Resistance does not appear<br />
to be increased or induced by long-term suppressive<br />
therapy with these medications. 64 In contrast, the<br />
increased HSV acyclovir-resistance rates seen in HIVpositive<br />
patients may reflect the increased replication<br />
<strong>of</strong> HSV in these patients; therefore resistance<br />
may actually be reduced by long-term suppressive<br />
thymidine kinase inhibitor therapy. 65<br />
Resistance to acyclovir may be mediated by mutations<br />
in either the HSV thymidine kinase or HSV<br />
DNA polymerase genes with decreased substrate<br />
affinity or by decreased or absent production <strong>of</strong> the
412 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
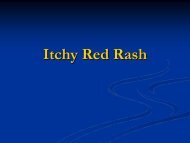
Fig 2. HIV-positive patient. Primary syphilis: perianal<br />
chancres.<br />
HSV thymidine kinase. 66 If resistance is suspected,<br />
HSV cultures and susceptibility testing are indicated.<br />
As such, the virus remains susceptible to foscarnet<br />
(which competitively blocks the pyrophosphate<br />
binding site <strong>of</strong> viral DNA polymerase) and cid<strong>of</strong>ovir<br />
(which is a nucleotide analogue not dependent on<br />
viral thymidine kinase). 67 In cases <strong>of</strong> acyclovir resistance,<br />
intravenous foscarnet, 40 mg/kg <strong>of</strong> body<br />
weight every 8 hours, or topical cid<strong>of</strong>ovir 1% applied<br />
to the lesions daily is suggested therapy from the<br />
CDC. 1<br />
Foscarnet resistance has been reported, and this<br />
may make cid<strong>of</strong>ovir the most viable option. 68,69<br />
Regardless, these two medicines have important<br />
potential side effects. Foscarnet is nephrotoxic and<br />
can produce severe hypocalcemia, and in a phase I/II<br />
trial, topical cid<strong>of</strong>ovir gel in concentrations <strong>of</strong> 3%<br />
and 5% was associated with local toxicity and delayed<br />
healing. 70<br />
Syphilis. The interactions between syphilis and<br />
HIV gained widespread attention after a 1987 case<br />
series described HIV-infected patients whose syphilis<br />
infection was either refractory to appropriate thera-<br />
pies or displayed a rapid progression from primary<br />
syphilis to neurosyphilis. 71 Since this report, many<br />
investigators have studied the atypical features <strong>of</strong><br />
syphilis in the setting <strong>of</strong> HIV disease, but the significance<br />
<strong>of</strong> these features remains unclear. Syphilis in<br />
the HIV patient appears to progress more rapidly<br />
through the clinical stages <strong>of</strong> syphilis, <strong>of</strong>ten will have<br />
an atypical clinical presentation, may have a refractory<br />
course after appropriate intramuscular penicillin,<br />
and may lead to unusual serologic test results (Fig 2).<br />
Numerous reports describe an accelerated progression<br />
through the syphilitic stages in HIV patients. 71-74<br />
This progression may be related to level <strong>of</strong> immunosuppression;<br />
one study described HIV-infected<br />
patients initially presenting to physicians with undiagnosed<br />
secondary syphilis when their CD4 cell counts<br />
were less than 500 cells/mm 3 . 75 Others reported an<br />
association between accelerated ulcerating syphilis<br />
(malignant syphilis) and advancing HIV disease. 76,77<br />
<strong>An</strong> association between advancing HIV disease and<br />
progression to neurosyphilis has also been noted. 76 In<br />
contradiction to these findings, Dowell et al 78 found<br />
no association between HIV stage and syphilitic progression<br />
or relapse after treatment.<br />
Although the clinical presentation is commonly the<br />
same in the HIV-infected host as it is in the otherwise<br />
healthy host, unusual features may be seen. The primary<br />
stage <strong>of</strong> syphilis may consist <strong>of</strong> multiple or more<br />
extensive chancres in the HIV patient. 79 Secondary<br />
syphilis affecting the immunocompetent host can present<br />
in a multitude <strong>of</strong> fashions, and likewise, the HIV<br />
patient can exhibit a wide range <strong>of</strong> cutaneous manifestations<br />
in this stage. Several reports document that<br />
patients with HIV are more likely to progress to neurosyphilis<br />
in the first 2 years after diagnosis, <strong>of</strong>ten<br />
despite appropriate therapy. 71-73,80-85 Unusual manifestations<br />
<strong>of</strong> neurosyphilis 86 have been documented<br />
in HIV-infected patients, as have unusual gummatous<br />
lesions. 87 Furthermore, rapidly developing cases <strong>of</strong><br />
ocular syphilis 82,88,89 and syphilitic aortitis 90 have been<br />
reported in the HIV-infected population. Encephalitis<br />
and arteritis are other potential atypical presentations<br />
<strong>of</strong> syphilis in the HIV-infected host.<br />
For most people with coinfections <strong>of</strong> HIV and<br />
syphilis, laboratory tests can be interpreted as they<br />
would in an immunocompetent person. 1 However,<br />
atypical serologic responses in HIV-infected patients<br />
with syphilis do occur. Most reports involve falsepositive<br />
responses to the two nontreponemal<br />
screening tests: the rapid plasma reagin card test and<br />
the Venereal Disease Research Laboratory (VDRL)<br />
test. This sort <strong>of</strong> false-positive test is termed a “biologic<br />
false positive.” Several studies document an<br />
increased rate <strong>of</strong> biologic false positives in HIVinfected<br />
patients when compared with controls. 91-93
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
In addition, one study noted an increased rate <strong>of</strong> biologic<br />
false-positive findings among those HIV<br />
patients who acquired their disease through intravenous<br />
drug abuse and in those who were coinfected<br />
with the hepatitis B virus (HBV), as compared<br />
with homosexual HIV-positive controls. 94 Other<br />
Czelusta, Yen-Moore, and Tyring 413<br />
Fig 3. HIV-positive patient. Biopsy-confirmed, seronegative secondary syphilis.<br />
Fig 4. Photomicrograph <strong>of</strong> biopsy specimen <strong>of</strong> secondary syphilis shows dense lichenoid infiltrate<br />
with abundant plasma cells and histiocytes.<br />
abnormalities reported in serologic tests involve<br />
delayed titer responses after treatment <strong>of</strong> syphilis in<br />
HIV-infected patients. Typically, a patient’s biologic<br />
titers are expected to drop 4-fold after treatment. In<br />
HIV-infected patients, studies have documented<br />
both a normal serologic titer response after syphilis
414 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
Table I. Recommended management for syphilis in HIV-infected patients 1<br />
Stage Treatment Follow-up<br />
Primary, secondary, or early latent 2.4 × 10 6 U intramuscular benzathine Clinical and serologic exams at 3, 6, 9, 12,<br />
syphilis penicillin G once and 24 mo<br />
Late latent syphilis or syphilis <strong>of</strong> 2.4 × 10 6 U <strong>of</strong> intramuscular Clinical and serologic exams at 6, 12, 18,<br />
unknown duration benzathine penicillin G weekly for and 24 mo<br />
3 wk<br />
Neurosyphilis or ocular syphilis* 3-4 × 10 6 U <strong>of</strong> intravenous aqueous If CSF pleocytosis was initially present,<br />
crystalline penicillin G every 4 h for CSF exams every 6 mo (for up to 2 yr)<br />
10-14 days (or) intramuscular until this parameter returns to normal<br />
procaine penicillin 2.4 × 10 6 U daily<br />
and oral probenicid 500 mg 4 times<br />
per day for 10-14 days<br />
*Some experts recommend the addition <strong>of</strong> a single intramuscular dose <strong>of</strong> 2.4 × 10 6 U <strong>of</strong> benzathine penicillin G to the conclusion <strong>of</strong> therapy<br />
in cases <strong>of</strong> neurosyphilis.<br />
treatment 75,95,96 and a delayed serologic titer<br />
response after syphilis treatment. 79,97-99 Finally,<br />
other reports describe cases <strong>of</strong> seronegative syphilis,<br />
accelerated loss <strong>of</strong> antibody reactivity after treatment,<br />
antibody production to decreased numbers <strong>of</strong><br />
treponemal antigens, and the return <strong>of</strong> titers to nonreactive<br />
as immunosuppression advances (Fig<br />
3). 100-105 When serologic tests are inconsistent with<br />
clinical suspicion, other tests are indicated, such as<br />
lesional biopsy (Fig 4), dark-field microscopy, or<br />
direct fluorescent antibody staining <strong>of</strong> lesion material.<br />
1 Still, the histologic features <strong>of</strong> a biopsied lesion<br />
may be altered in HIV-infected patients. 106<br />
Progression to neurosyphilis despite appropriate<br />
therapy 71-73,80-85 has prompted some experts to recommend<br />
regular cerebrospinal fluid (CSF) examinations<br />
in HIV-infected patients when they are first<br />
diagnosed with either primary or secondary syphilis 1<br />
in addition to current recommendations for CSF<br />
examinations in HIV-infected patients with late latent<br />
syphilis. * These experts recommend modification <strong>of</strong><br />
treatment based on the CSF laboratory results.<br />
However, the CSF results in this population may be<br />
difficult to interpret, given the fact that HIV-positive<br />
patients have high rates <strong>of</strong> CSF abnormalities without<br />
syphilis infection. 1<br />
General treatment guidelines as recommended<br />
by the CDC are outlined in Table I. In the management<br />
<strong>of</strong> patients with primary, secondary, or early<br />
latent syphilis, some specialists recommend supple-<br />
*Early latent syphilis is defined as those asymptomatic patients<br />
with titers suggestive <strong>of</strong> a current syphilis infection who, within<br />
the past year, acquired syphilis as reflected either by a documented<br />
seroconversion, indisputable symptoms <strong>of</strong> primary or<br />
secondary syphilis, or a sex partner who had primary, secondary,<br />
or early latent syphilis in the past year. Almost all other patients<br />
have either late latent syphilis or syphilis <strong>of</strong> unknown duration.<br />
mental antibiotic therapy in addition to that listed,<br />
and some experts recommend a CSF examination at<br />
6 months after therapy in this group. 1 Those patients<br />
in this group who do not respond to treatment but<br />
whose CSF findings remain normal are treated with<br />
intramuscular benzathine penicillin G 2.4 × 10 6 U<br />
weekly for 3 weeks. 1<br />
If during the follow-up <strong>of</strong> any patient with late<br />
latent syphilis or syphilis <strong>of</strong> unknown duration, he or<br />
she develops symptoms or a rise in antibody titers,<br />
then CSF should be examined and retreatment<br />
administered appropriately. 1 In any HIV-infected<br />
patient with syphilis <strong>of</strong> any stage, penicillin desensitization<br />
is recommended if the patient is allergic to<br />
penicillin. 1 The management <strong>of</strong> syphilis in the HIVinfected<br />
host is a complex issue in which further<br />
study is clearly necessary.<br />
Chancroid. Chancroid is the most common cause<br />
<strong>of</strong> genital ulceration in Africa, 107 and outbreaks have<br />
been reported in Europe, Canada, and the United<br />
States. 108,109 Men are most commonly affected, and<br />
the typical clinical presentation is single or multiple<br />
s<strong>of</strong>t-edged ulcers that are accompanied by inguinal<br />
adenopathy in 40% to 70% <strong>of</strong> cases. 110 Although relatively<br />
few studies have evaluated chancroid in HIVpositive<br />
patients, the clinical presentation appears to<br />
have only minor differences from HIV-negative<br />
patients, and the rate <strong>of</strong> treatment failures may be<br />
slightly increased in HIV-positive patients. 111-115<br />
Ulcer size was consistently unaffected by HIV<br />
serostatus in all studies surveyed. 111-114 The only differences<br />
reported include a longer ulcer duration<br />
113,114 and a greater number <strong>of</strong> ulcers at initial<br />
presentation 113 in HIV-positive patients. Nonetheless,<br />
atypical presentations can occur as evidenced<br />
by an HIV-positive patient from New York who had<br />
chancroid that presented as a chronic penile ulcer
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
Fig 5. HIV-positive patient. Chancroid with typical “kissing” ulcers.<br />
accompanied by the development <strong>of</strong> ulcers on his<br />
legs and digits 115 (Fig 5).<br />
Two studies that evaluated histologic features <strong>of</strong><br />
punch biopsy specimens from chancroid ulcers<br />
found that specimens from HIV-negative and -positive<br />
patients had no notable differences. 114,116 As in<br />
the immunocompetent host, diagnosis <strong>of</strong> chancroid<br />
in the HIV-positive patient is ideally made by culture<br />
<strong>of</strong> the causative organism, Haemophilus ducreyi, or,<br />
if this is not possible, by the presence <strong>of</strong> a clinical<br />
presentation typical <strong>of</strong> chancroid (ie, genital ulcers,<br />
usually painful, <strong>of</strong>ten multiple, with ragged edges<br />
and a base covered by a necrotic, yellow-gray exudate),<br />
and negative laboratory evaluations for both<br />
Treponema pallidum and HSV. 1<br />
Several clinical trials report the efficacy <strong>of</strong> antibiotic<br />
therapy for chancroid on the basis <strong>of</strong> their subjects’<br />
HIV serostatus. 112-114,117-120 Studies <strong>of</strong> a single<br />
quinolone (fleroxacin) dose demonstrated that HIVpositive<br />
patients are cured <strong>of</strong> chancroid less frequently<br />
with these treatments than are HIV-negative<br />
patients. 117,118 However, despite the apparent consistent<br />
difference in response rates, none <strong>of</strong> these studies<br />
achieved statistical significance in this comparison.<br />
One study actually extended the quinolone therapy <strong>of</strong><br />
HIV-negative patients to 5 days and compared it with<br />
single-dose therapy in HIV-positive patients. 112 Again,<br />
while the HIV-positive patients were cured at a lower<br />
rate than the HIV-negative patients, the difference was<br />
not statistically significant. Single-dose ceftriaxone and<br />
single-dose azithromycin demonstrate statistically sig-<br />
Czelusta, Yen-Moore, and Tyring 415<br />
nificant failure rates in treating HIV-positive patients<br />
with chancroid when compared with HIV-negative<br />
patients. 119,120 Similarly, 7-day erythromycin therapy<br />
has shown significantly lower rates <strong>of</strong> curing chancroid<br />
infections in HIV-infected patients at 1 and 2 weeks<br />
after starting therapy, 113,114,120 but when these<br />
patients are observed to 3 weeks, the cure rates are<br />
not significantly different between HIV-positive and<br />
-negative patients. 114 Current CDC recommendations<br />
for treatment <strong>of</strong> chancroid in immunocompetent and<br />
HIV-infected patients are the same: oral azithromycin<br />
1 g in a single dose, intramuscular ceftriaxone 250 mg<br />
in a single dose, oral cipr<strong>of</strong>loxacin 500 mg twice daily<br />
for 3 days, or oral erythromycin base 500 mg 4 times<br />
daily for 7 days. 1 In addition, the CDC notes that HIVpositive<br />
patients may require longer courses <strong>of</strong> therapy<br />
than those listed and that any <strong>of</strong> the regimens may<br />
fail. For this reason, close follow-up <strong>of</strong> HIV-positive<br />
chancroid patients with chancroid is essential.<br />
Granuloma inguinale. Granuloma inguinale,<br />
caused by Calymmatobacterium granulomatis, is<br />
endemic to the Caribbean, South America, South<br />
Africa, Southeast India, Papua New Guinea, and<br />
among the Aborigines in central Australia, 121 but it is<br />
extremely rare in North America. 122 It typically<br />
involves the genitalia with a chronic, destructive,<br />
beefy red, nontender granulomatous ulcer, and diagnosis<br />
is made in both HIV-positive and HIV-negative<br />
patients by visualizing characteristic intracytoplasmic<br />
Donovan bodies on microscopic evaluation <strong>of</strong> either<br />
tissue smears or biopsy specimens. 123 Few data are
416 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
Table II. Recommended therapy for granuloma inguinale and lymphogranuloma venereum 1<br />
Infection Recommended therapy Alternative therapy<br />
Granuloma inguinale* Oral trimethoprim-sulfamethoxazole Oral cipr<strong>of</strong>loxacin 750 mg twice daily (or)<br />
double-strength tablet twice daily oral erythromycin base 500 mg 4 times<br />
(or) oral doxycycline 100 mg twice daily until lesions heal or for at least 3 wk<br />
daily until lesions heal or for at least<br />
3 wk<br />
Lymphogranuloma venereum Aspiration or incision and drainage <strong>of</strong> Aspiration or incision and drainage <strong>of</strong><br />
buboes if necessary and oral buboes if necessary and oral erythromycin<br />
doxycycline 100 mg twice daily for 3 wk base 500 mg 4 times daily for 3 wk<br />
*Gentamicin (1 mg/kg intravenously every 8 h) should be strongly considered in HIV-positive patients.<br />
available about the effects <strong>of</strong> HIV infection on this<br />
disease, but it appears that HIV-positive patients<br />
have ulcers that persist for a longer duration and<br />
may require more intensive antibiotic therapy as<br />
compared with HIV-negative patients. 124 A prospective<br />
case-control study <strong>of</strong> 50 patients (21 HIV-positive<br />
and 29 HIV-negative) in India demonstrated<br />
that, while the ulcer size and clinical presentations <strong>of</strong><br />
HIV-positive and HIV-negative patients with granuloma<br />
inguinale were not significantly different, the<br />
mean duration to complete ulcer healing was significantly<br />
longer in HIV-positive patients (25.7 vs 16.8<br />
days) and associated with greater tissue destruction.<br />
124 A retrospective study <strong>of</strong> pregnant women<br />
with granuloma inguinale demonstrated no difference<br />
in pregnancy outcome between HIV-negative<br />
and HIV-positive patients. 125 Although extragenital<br />
dissemination <strong>of</strong> granuloma inguinale has been<br />
reported in association with HIV infection, 126 most<br />
case reports note the failure <strong>of</strong> traditional antibiotic<br />
treatments. 127-129 In one case, a patient who did not<br />
respond to therapy or relapsed after treatment with<br />
doxycycline, tetracycline, erythromycin, cephalexin,<br />
ceftriaxone, and trimethoprim-sulfamethoxazole<br />
finally responded to a combination <strong>of</strong> trimethoprimsulfamethoxazole<br />
and <strong>of</strong>loxacin. 129<br />
Currently the CDC recommends the same treatments<br />
for granuloma inguinale in HIV-negative and<br />
HIV-positive patients (Table II) with the note that<br />
gentamicin (1 mg/kg administered intravenously<br />
every 8 hours) should be strongly considered in HIVpositive<br />
patients. 1 Although granuloma inguinale is a<br />
relatively rare infection, O’Farell, Windsor, and<br />
Becker 28 have recommended a unified public health<br />
effort for its eradication based on its ease <strong>of</strong> treatment<br />
and strong association with HIV transmission.<br />
LYMPHOGRANULOMA VENEREUM<br />
Lymphogranuloma venereum, caused by the L 1 ,<br />
L 2 , and L 3 immunotypes <strong>of</strong> Chlamydia trachomatis,<br />
may present clinically as primary (papule), secondary<br />
(inguinal), and tertiary (rectal) lesions. 130,131<br />
Lymphogranuloma venereum occurs most frequently<br />
in tropical countries and is rare in the United<br />
States. 132 In both HIV-positive and HIV-negative<br />
patients, diagnosis is made by a combination <strong>of</strong> clinical<br />
presentation and high chlamydial complement<br />
fixation antibody titers (≥ 1:64). No studies have<br />
been performed on patients with concomitant HIV<br />
infection and lymphogranuloma venereum, and<br />
remarkably little anecdotal evidence regarding clinical<br />
features and treatment has been published.<br />
Retrospective analysis <strong>of</strong> 27 cases <strong>of</strong> lymphogranuloma<br />
venereum seen in a Paris hospital found 6<br />
cases <strong>of</strong> concomitant HIV and lymphogranuloma<br />
venereum infection. HIV appeared to have no effect<br />
on the clinical presentation in each <strong>of</strong> these 6<br />
cases. 133 Similarly, Heaton et al 134 reported a case in<br />
which an HIV-positive pregnant woman had uncomplicated<br />
lymphogranuloma venereum.<br />
Nonetheless, an atypical presentation <strong>of</strong><br />
Parinaud’s oculoglandular syndrome (unilateral follicular<br />
conjunctivitis followed by enlargement <strong>of</strong><br />
preauricular lymph nodes) with associated inguinal<br />
lymphadenopathy due to Chlamydia trachomatis<br />
immunotype L 2 has been reported. This patient<br />
responded well to surgical management, topical<br />
(ocular) cefazolin and gentamicin, and oral tetracycline.<br />
135 The CDC recommends the same treatments<br />
for lymphogranuloma venereum in HIV-negative and<br />
HIV-positive patients (see Table II), with the note<br />
that disease duration may be prolonged in HIV-positive<br />
patients. 1<br />
HUMAN PAPILLOMAVIRUS<br />
Subclinical genital human papillomavirus<br />
infections<br />
Subclinical genital human papillomavirus (HPV)<br />
can affect the cervix, vagina, vulva, penis, anus, or<br />
any other genital skin. 136 The same types can also
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
Fig 6. HIV-positive patient. Oral condyloma acuminatum (ie, HPV type 6).<br />
infect the oral epithelium (Fig 6). The association<br />
between certain HPV types (eg, HPV types 16, 18, 31,<br />
and 45) and the development <strong>of</strong> dysplastic lesions in<br />
the cervix is well known. 137 The dysplastic lesion,<br />
termed a cervical squamous intraepithelial lesion<br />
(CSIL), occurs in the transformation zone along the<br />
squamocolumnar junction near the cervical os. CSIL<br />
is a precursor to cervical cancer. Similarly, the anal<br />
canal has a squamocolumnar junction and transformation<br />
zone that is affected by HPV infections.<br />
Specifically, the anal squamous intraepithelial lesion<br />
(ASIL) and invasive anal cancer appear to be associated<br />
with HPV infections, most notably HPV type 16<br />
infections. 138-141<br />
Genital HPV infections occur more commonly in<br />
HIV-infected men and women when compared with<br />
age-matched healthy control populations. 140,142-145<br />
The lesions are more frequently diffuse, dysplastic,<br />
and subclinical in HIV patients, whereas control populations<br />
more commonly have condylomatous<br />
lesions and less commonly have subclinical and dysplastic<br />
lesions. 146 In addition, HIV-positive patients<br />
tend to be infected with more HPV types than control<br />
populations. 144,147-149 As CD4 cell count decreases,<br />
shedding <strong>of</strong> HPV and extent <strong>of</strong> disease appear to<br />
increase. 150,151<br />
Given these clinical features, HPV replication and<br />
disease progression appear to be potentiated by HIV<br />
infections. 150,151 The mechanism behind this phenomena<br />
is unclear. HIV appears to influence gene<br />
transcription in HPV. 152,153 This may lead to a defect<br />
in the host’s local immune defenses and, when<br />
Czelusta, Yen-Moore, and Tyring 417<br />
accompanied by the systemic immunosuppression<br />
<strong>of</strong> HIV infection, may explain the increased severity<br />
<strong>of</strong> HPV infections observed in this setting.<br />
Regardless <strong>of</strong> the exact mechanism, it is clear that<br />
HIV-infected persons have higher rates <strong>of</strong> cervical,<br />
anal, and other genital cancers (Figs 7 and 8). Those<br />
persons most at risk are women with a history <strong>of</strong><br />
abnormal Papanicolaou (pap) smears and men or<br />
women who participate in receptive anal intercourse<br />
or have a history <strong>of</strong> anal condyloma. Not surprisingly,<br />
anal cancer is currently the fourth most common<br />
reportable cancer among HIV-positive men 154 and is<br />
about 7 times more common in homosexual men<br />
with HIV than those who are HIV seronegative.<br />
Likewise, cervical cancer in an HIV patient is an<br />
AIDS-defining illness. 38<br />
Clinically, full genital examinations in HIV-positive<br />
patients are extremely important. In women, the<br />
CDC recommends two pap smears and pelvic examinations<br />
during the first year after a diagnosis <strong>of</strong> HIV. 1<br />
If the results are normal, yearly pap smears and<br />
pelvic examinations are indicated thereafter. 1<br />
Abnormal results should be managed in consultation<br />
with a gynecologist, and current CDC recommendations<br />
regarding this issue are listed in the “Interim<br />
Guidelines for Management <strong>of</strong> Abnormal Cervical<br />
Cytology.” 155 Some research suggests that pap<br />
smears are an insensitive method to screen for cervical<br />
cancer in AIDS patients. 156 Subsequently, some<br />
experts support colposcopy as a regular screening<br />
tool in patients when they are initially diagnosed<br />
with HIV. 156 Nonetheless, a more recent study con-
418 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
Fig 7. HIV-positive patient. Adenocarcinoma <strong>of</strong> the anus.<br />
(Courtesy <strong>of</strong> Axel Hoke, MD, Novato, Calif.)<br />
tradicts these arguments by finding that pap smears<br />
are adequately sensitive in HIV-infected patients. 157<br />
The CDC specifically states that colposcopy is not<br />
indicated as a regular screening tool for women with<br />
HIV. 1<br />
There is no established method <strong>of</strong> screening for<br />
anal disease in HIV patients. Certainly inspection <strong>of</strong><br />
the anal region is an important part <strong>of</strong> the evaluation.<br />
Often, dysplastic lesions are highlighted in<br />
white after the application <strong>of</strong> acetic acid. Moreover,<br />
ASIL may present as Bowen’s disease <strong>of</strong> the perianal<br />
region. 151 This usually presents as pigmented<br />
papules or plaques. Condylomata acuminata may<br />
harbor dysplastic lesions, and anal cancer frequently<br />
originates from epithelium external to the anal<br />
verge. <strong>An</strong>al cancer may present with perirectal bleeding,<br />
constipation, or tenesmus, and occasionally<br />
perirectal induration or erythema. For these reasons,<br />
external inspection is an important tool in the<br />
screening for anal disease in HIV-infected patients.<br />
Palefsky 151 supports an ASIL screening process<br />
that would test only the persons at highest risk for<br />
Fig 8. HIV-positive patient. Verrucous carcinoma <strong>of</strong> the<br />
penis.<br />
ASIL in whom treatment would be most appropriate.<br />
Specifically, the group would include HIV-positive<br />
men with a history <strong>of</strong> receptive anal intercourse who<br />
might benefit from aggressive treatment <strong>of</strong> premalignant<br />
lesions. Excluded from this group would be<br />
HIV-infected patients with a poor prognosis, as<br />
determined by either CD4 cell counts or HIV plasma<br />
RNA levels. In addition, HIV-negative men who participate<br />
in receptive anal intercourse or have a history<br />
<strong>of</strong> perianal or intra-anal condylomas may represent<br />
an appropriate group for screening. Palefsky<br />
recognizes that similar risk groups in women might<br />
be appropriate for screening but admits that too few<br />
studies have evaluated ASIL in women for sound scientific<br />
recommendations regarding this population.<br />
<strong>An</strong>ogenital warts<br />
In the immunocompetent host anogenital warts<br />
are most commonly caused by HPV types 6 and 11.<br />
Studies have demonstrated that when compared<br />
with normal hosts, HIV-infected patients’ anogenital<br />
warts more frequently represent infections with mul
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
tiple HPV types, including oncogenic types. 146,158-60<br />
Clinically, although HIV patients may have the same<br />
condylomas as normal persons, they may also have<br />
more extensive or even disseminated condylomas<br />
that may be relatively refractory to treatment.<br />
Furthermore, HIV-infected patients’ condylomas are<br />
associated with a significant risk <strong>of</strong> transformation<br />
into squamous cell carcinoma.<br />
Proper diagnosis is essential in these cases.<br />
Usually, anogenital warts are diagnosed by clinical<br />
acumen, but in HIV-infected patients biopsy should<br />
be considered before therapy so that appropriate<br />
diagnosis <strong>of</strong> dysplastic changes or squamous cell<br />
cancer can be ascertained early in the disease management<br />
process. 1,158 Treatment options available to<br />
the HIV-infected host do not differ from those available<br />
to the immunocompetent host and are discussed<br />
by Brown, Tyring, and Yen-Moore 161 in part II<br />
<strong>of</strong> this series on <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>. Some<br />
clinicians advocate treatment by excision and electrodesiccation<br />
because <strong>of</strong> the poor response and frequent<br />
recurrences after topical treatments 162 and<br />
the association between HPV and cancer in this population.<br />
158,163<br />
Notwithstanding, some studies have evaluated<br />
nonsurgical treatment modalities for genital warts<br />
in the immunocompromised host. Podophyllotoxin<br />
has been studied for genital warts in HIV-positive<br />
Tanzanian patients, 164 but given the association <strong>of</strong><br />
HPV in HIV-infected patients with squamous cell<br />
cancer, this therapy may be inappropriate for this<br />
population. 165 Interferon has been studied in this<br />
population, 166,167 as has imiquimod. 168 Although<br />
both have some efficacy in treating HPV infection in<br />
HIV patients, neither appears to be effective as<br />
monotherapy in completely clearing clinical lesions<br />
from the most severely immunocompromised<br />
patients. Use <strong>of</strong> imiquimod as adjunctive therapy<br />
after surgical or cytodestructive treatment <strong>of</strong><br />
condyloma acuminatum does appear effective in<br />
HIV-seropositive and in other immunocompromised<br />
patients in terms <strong>of</strong> significant delays or prevention<br />
<strong>of</strong> recurrences. Cid<strong>of</strong>ovir gel has been<br />
studied in a phase I/II trial <strong>of</strong> HIV-positive patients<br />
with condylomata acuminata and appears safe and<br />
potentially effective in this population. 169 Finally,<br />
Orlando et al 170 recently reported that relapse<br />
rates <strong>of</strong> condyloma in HIV-infected patients<br />
decreased with improved treatment <strong>of</strong> their underlying<br />
HIV infection with antiretroviral medication.<br />
Successful treatment <strong>of</strong> condylomas thus appears<br />
easier when a person’s underlying HIV infection is<br />
better controlled. Clearly, treatment <strong>of</strong> HPV infections<br />
in HIV-infected patients is an issue that<br />
deserves further study.<br />
Czelusta, Yen-Moore, and Tyring 419<br />
MOLLUSCUM CONTAGIOSUM<br />
The association between HIV infection and molluscum<br />
contagiosum was first noticed in 1983<br />
through an autopsy study <strong>of</strong> 10 patients with<br />
AIDS. 171 Many reports <strong>of</strong> severe and atypical infections<br />
have surfaced, and in AIDS patients, the prevalence<br />
<strong>of</strong> molluscum contagiosum lesions ranges<br />
from 5% to 18%. 172-176 Dann and Tabibian 177 document<br />
molluscum contagiosum as one <strong>of</strong> the 3 most<br />
common reasons nondermatologists referred HIVinfected<br />
patients to a university-based immunosuppression<br />
skin clinic.<br />
In HIV-infected patients, molluscum contagiosum<br />
manifests itself most commonly when immune function<br />
has been dramatically reduced. Several studies<br />
document that molluscum contagiosum infection is<br />
a clinical sign <strong>of</strong> marked HIV progression and very<br />
low CD4 cell counts. 176,178-181 Specifically, when the<br />
CD4 cell count drops below 200/mm 3 , the incidence<br />
<strong>of</strong> molluscum contagiosum appears to increase dramatically.<br />
182 The unfortunate clinical correlate with<br />
this finding is that AIDS patients in whom molluscum<br />
contagiosum occurs have a poor prognosis,<br />
with a median survival time <strong>of</strong> 12 months in one<br />
study. 176 The presence <strong>of</strong> mollusca, however, does<br />
not appear to be an independent prognostic indicator<br />
after accounting for immunosuppression.<br />
Considerable debate remains as to whether the<br />
disease is caused by the reactivation <strong>of</strong> latent virus or<br />
whether it represents a recently acquired infection<br />
complicating patients’ progressive immunosuppression.<br />
The molluscum contagiosum virus commonly<br />
infects the general population. In an Australian study<br />
incorporating both HIV-positive and HIV-negative<br />
patients, 23% <strong>of</strong> the studied population had antibodies<br />
consistent with either a current or previous<br />
infection. 183 As the age <strong>of</strong> the studied population<br />
increased, so did the frequency <strong>of</strong> molluscum contagiosum<br />
antibodies. 183 These findings were believed<br />
to support the theory that mollusca in AIDS patients<br />
reflect the reactivation <strong>of</strong> a latent infection. 184<br />
However, other studies contradict this supposition.<br />
Molecular research demonstrates that molluscum<br />
contagiosum viruses can be divided into two<br />
major types (designated MCV-1 and MCV-2) based<br />
upon restriction fragment cleavage patterns <strong>of</strong> the<br />
viruses’ genome. 185 Although it is not yet clear what<br />
clinical implications these types may have, the ratio<br />
<strong>of</strong> MCV-1 to MCV-2 in one Japanese population was<br />
found to be 13:1. 186 MCV-1 occurred in highest frequency<br />
in children and adult women, whereas MCV-<br />
2 occurred more frequently in adult men and<br />
patients with HIV. 186 This study was consistent with<br />
an earlier Australian study that showed HIV-positive<br />
patients were significantly more likely to be infected
420 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
Fig 9. HIV-positive patient. Molluscum contagiosum.<br />
by the MCV-2 virus than control patients. 187 The<br />
presence <strong>of</strong> MCV-2 in these patients may suggest<br />
that HIV-positive patients are manifesting an adult<br />
acquired infection because young and healthy<br />
patients are more commonly infected with MCV-1. 187<br />
Clinically, molluscum contagiosum in HIV-positive<br />
persons appears to be <strong>transmitted</strong> in both sexual and<br />
nonsexual patterns. Lesions in healthy, <strong>sexually</strong><br />
active adults commonly occur on the lower<br />
abdomen, inner thighs, and genitalia. HIV-infected<br />
patients may have lesions with this distribution, but<br />
lesions on the face and neck are more common (Fig<br />
9). In one study <strong>of</strong> mostly homosexual HIV-positive<br />
men, 14 <strong>of</strong> 27 patients had lesions on the face and<br />
neck, whereas only 7 patients had lesions in locations<br />
associated with sexual transmission. 188<br />
Ophthalmologists have described many cases <strong>of</strong><br />
complicated eyelid mollusca in HIV-infected<br />
patients. 189,190 The lesions can become quite large<br />
(up to 2 cm) 191 and numerous (numbering up to the<br />
hundreds). 192 They are prone to autoinoculation,<br />
and in male patients, shaving the beard area has<br />
been reported to cause particularly severe infec-<br />
tions, with lesions encompassing their entire<br />
face. 184,193,194 Certainly, numerous lesions on a<br />
patient who is not yet diagnosed with HIV disease<br />
should prompt discussion <strong>of</strong> an HIV test. 195<br />
Atypical molluscum contagiosum is common in<br />
HIV patients. Lesions may resemble comedones,<br />
abscesses, furuncles, condylomas, syringomas, keratoacanthomas,<br />
basal cell carcinomas, ecthyma, a<br />
sebaceous nevus <strong>of</strong> Jadassohn, and a cutaneous<br />
horn. 196-201 Importantly, disseminated fungal infections,<br />
specifically cryptococcosis, 202,203 Penicillium<br />
marneffei infection, and histoplasmosis, 204 are<br />
reported to clinically mimic molluscum contagiosum<br />
and should be included in the differential diagnosis<br />
for these patients.<br />
Because <strong>of</strong> the atypical nature <strong>of</strong> mollusca in the<br />
HIV-positive patient, diagnosis is in large part dependent<br />
on biopsy. Studies evaluating the microscopic<br />
and ultrastructural (electron microscopic) features<br />
<strong>of</strong> mollusca identified no major differences between<br />
samples taken from healthy patients as compared<br />
with patients with AIDS. 184,205 One possible exception<br />
to this might be that AIDS patients are less likely<br />
to have the inflammation and lymphocytic infiltrates<br />
associated with mollusca regression in their<br />
tissue. Interestingly, Smith et al 206 noted ultrastructural<br />
evidence for the presence <strong>of</strong> viral particles in<br />
“immunocompetent” skin adjacent to mollusca in<br />
HIV-infected patients. This was thought to help<br />
explain the high recurrence rates <strong>of</strong> lesions after<br />
treatment. 206,207<br />
Molluscum contagiosum in HIV-positive patients<br />
is notoriously difficult to treat, 208 and unlike otherwise<br />
healthy hosts, there is no evidence that lesions<br />
spontaneously resolve. Most available evidence<br />
regarding the management <strong>of</strong> molluscum contagiosum<br />
in HIV-infected patients is anecdotal. Some<br />
potential treatment modalities are listed in Table <strong>III</strong>.<br />
Perhaps the most widely used methods are curettage<br />
209 and cryosurgery. Tretinoin may serve as a<br />
helpful adjunct to any locally destructive therapy<br />
through daily applications. 192 Although this medicine<br />
does appear to diminish the appearance <strong>of</strong> new<br />
lesions and help eliminate old lesions, its use is<br />
limited by local irritation. Nonetheless, some<br />
researchers have reported success in AIDS patients<br />
by using nightly tretinoin as an adjunct to cantharidin<br />
(applied for up to 24 hours) on body and<br />
facial lesions followed by curettage for recalcitrant<br />
lesions. 192 One study using trichloroacetic acid peels<br />
yielded an average reduction in molluscum contagiosum<br />
lesion counts <strong>of</strong> 40.5% in 7 HIV-seropositive<br />
patients. 210 Intralesional 211 and systemic interferon<br />
212 have been used with minimal to moderate success<br />
in treating AIDS patients with mollusca.
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
Imiquimod has been studied in AIDS patients and<br />
certainly deserves consideration as a potential therapy.<br />
213 Crude podophyllin extract might be a poor<br />
choice in an HIV-infected patient, given the predisposition<br />
for the development <strong>of</strong> cancer in these<br />
patients and podophyllin’s link to the mutagens<br />
quercetin and kaempherol. 165 Cid<strong>of</strong>ovir is a<br />
nucleotide analog that is used most commonly for<br />
the treatment <strong>of</strong> cytomegalovirus retinitis in AIDS<br />
patients. 214 Because <strong>of</strong> its activity against DNA viruses,<br />
it may be effective as either an intravenous or topical<br />
therapy for recalcitrant mollusca. A recent case<br />
report describes resolution <strong>of</strong> extensive facial lesions<br />
in 3 AIDS patients after beginning either intravenous<br />
or topical cid<strong>of</strong>ovir therapy. 215 The authors <strong>of</strong> this<br />
report point out that the patients’ improvement<br />
most closely correlates with the use <strong>of</strong> cid<strong>of</strong>ovir, but<br />
that it is impossible to exclude the possible immune<br />
system–enhancing effects <strong>of</strong> antiretroviral therapy.<br />
At least 3 case reports describe the reduction in<br />
number <strong>of</strong> patients’ extensive mollusca after beginning<br />
potent combination antiretroviral treatment.<br />
190,216,217 In one early case, a patient improved<br />
after initiation <strong>of</strong> zidovudine, 190 and in a more recent<br />
case, a patient improved after starting ritonavir. 216<br />
This highlights an important point: every attempt<br />
should be made to optimize treatment <strong>of</strong> the HIV<br />
infection in patients afflicted with molluscum contagiosum<br />
because this will make treatment <strong>of</strong> the molluscum<br />
contagiosum infection more feasible. 218<br />
HUMAN HERPESVIRUS 8<br />
Human herpesvirus 8 (HHV-8), formerly known<br />
as Kaposi’s sarcoma–associated herpesvirus, was<br />
originally identified in Kaposi’s sarcoma (KS) from<br />
AIDS patients. 221 It has been linked with all other<br />
forms <strong>of</strong> KS as well. 222-226 HHV-8 is also associated<br />
with a rare type <strong>of</strong> non-Hodgkin’s lymphoma,<br />
termed primary effusion lymphoma, 227,228 and with<br />
the plasma cell variant <strong>of</strong> Castleman’s disease. 229,230<br />
Furthermore, patients with HIV-associated KS are at<br />
a significantly greater risk for the development <strong>of</strong><br />
non-Hodgkin’s lymphoma than their unaffected<br />
counterparts. 231-234 Schwartz 235 discussed the major<br />
issues relating to KS in a comprehensive review, and<br />
a similar discussion would be inappropriate here.<br />
Although the biology <strong>of</strong> HHV-8 is not entirely understood,<br />
it appears to be a <strong>sexually</strong> <strong>transmitted</strong> infection<br />
in the United States and Western Europe.<br />
Most cases <strong>of</strong> AIDS-associated KS have appeared<br />
in men who participated in promiscuous homosexual<br />
activities or had a history <strong>of</strong> STDs. 236-244<br />
Furthermore, homosexual men whose partners live<br />
in areas <strong>of</strong> high HHV-8 prevalence, such as San<br />
Francisco or New York City, appear to be at an<br />
Czelusta, Yen-Moore, and Tyring 421<br />
Table <strong>III</strong>. Treatment modalities for molluscum<br />
contagiosum<br />
Surgical<br />
Curettage 192,209<br />
Electrodesiccation 192,218<br />
Cryotherapy 219<br />
Laser surgery 220<br />
Cytodestructive<br />
Cantharadin 192<br />
Iodine 192,218<br />
Lactic acid 207<br />
Phenol 192,207<br />
Salicylic acid 207<br />
Silver nitrate 192<br />
Tretinoin 192<br />
Trichloroacetic acid 210<br />
Chemotherapeutic/antiviral<br />
Cid<strong>of</strong>ovir 215<br />
Interferon 211,212<br />
Imiquimod 213<br />
increased risk <strong>of</strong> acquiring the virus. Those persons<br />
who acquired HIV non<strong>sexually</strong> (eg, hemophiliacs or<br />
intravenous drug abusers) have much lower rates <strong>of</strong><br />
KS than those people who contracted HIV from<br />
homosexual or bisexual contacts.<br />
Many studies have focused on shedding <strong>of</strong> HHV-8<br />
into semen with variable results. Most studies were<br />
unable to detect HHV-8 in either the semen <strong>of</strong><br />
healthy patients or HIV patients, 245-249 and detection<br />
<strong>of</strong> HHV-8 in the semen <strong>of</strong> patients with KS proved<br />
similarly difficult. However, two controversial studies<br />
reported high rates <strong>of</strong> HHV-8 in the semen <strong>of</strong><br />
healthy patients. 250,251 Oral secretions in patients<br />
with KS appear to consistently shed HHV-8 virions.<br />
252,253 Other suggested, but less investigated<br />
methods <strong>of</strong> transmission, include oral-anal contacts<br />
or exposure to feces. 254-256 Further investigation<br />
regarding this virus, its transmission, and its relationship<br />
to HIV is indicated.<br />
KS was originally described in HIV-seronegative<br />
persons (ie, classic KS). This form usually presents as<br />
purple plaques or papules on the lower extremities<br />
<strong>of</strong> elderly men <strong>of</strong> Mediterranean and/or Jewish<br />
decent. Patients with classic KS may die with this sarcoma<br />
but rarely die from it. In HIV-positive persons,<br />
however, a much wider variety <strong>of</strong> lesions (eg, patches,<br />
plaques, papules, nodules, ulcers) may appear<br />
anywhere on the skin or mucous membranes (Fig<br />
10). Visceral involvement <strong>of</strong> KS is common in HIVseropositive<br />
persons and is associated with significant<br />
morbidity and mortality. KS has been much less<br />
common in the past 3 years since the availability <strong>of</strong><br />
highly active antiretroviral therapy (HAART), which
422 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
suggests that the development or resolution <strong>of</strong> KS is<br />
tightly linked to immune system control <strong>of</strong> HHV-8.<br />
HEPATITIS B VIRUS AND HEPATITIS C<br />
VIRUS<br />
Both hepatitis B virus and hepatitis C virus (HBV<br />
and HCV, respectively) commonly coinfect HIVseropositive<br />
persons. Sexual transmission <strong>of</strong> HBV,<br />
however, appears to be more frequent than with HCV.<br />
Discussion <strong>of</strong> the cutaneous manifestations <strong>of</strong> those<br />
viruses as well as their treatment and prophylaxis can<br />
be found in part II <strong>of</strong> this 3-part STD review. 161<br />
The relationship between hepatitis C infection<br />
and sporadic porphyria cutanea tarda in the<br />
immunocompetent host is well documented. 257,258<br />
Similarly, sporadic porphyria cutanea tarda can occur<br />
in the HIV-positive patient in association with HCV<br />
infection. 259-262 Some reports evaluate the potential<br />
<strong>of</strong> HIV infection as an independent c<strong>of</strong>actor in the<br />
development <strong>of</strong> porphyria cutanea tarda. 262-265 One<br />
recent report describes a case in which an HCV- and<br />
HIV-infected man whose porphyria cutanea tarda<br />
subsided 18 months after starting HAART for HIV<br />
infection. 259 Regardless, any patients presenting with<br />
porphria cutanea tarda should be evaluated for both<br />
HCV and HIV infection.<br />
ECTOPARASITIC INFESTATIONS<br />
Scabies<br />
Scabies occurs commonly in young adults who<br />
acquire it through sexual contact. In 1848, Danielssen<br />
Fig 10. HIV-positive patient. Kaposi’s sarcoma.<br />
and Boeck first described a particularly contagious<br />
and fulminant form <strong>of</strong> scabies in Norwegian patients<br />
immunosuppressed as a consequence <strong>of</strong> Hansen’s<br />
disease. These patients’ infestations were characterized<br />
by thick, friable plaques. This form <strong>of</strong> scabies,<br />
Norwegian or crusted scabies, has emerged as yet<br />
another harbinger <strong>of</strong> HIV infection. Published reports<br />
<strong>of</strong> atypical and crusted scabies infestations in association<br />
with HIV infection have become increasingly frequent<br />
since the first such report in 1986. 266-298<br />
The defining clinical features <strong>of</strong> scabies in the<br />
HIV-positive patient are <strong>of</strong>ten determined by the<br />
degree <strong>of</strong> immunocompromise. 299 The typical presentation<br />
<strong>of</strong> a person infested with scabies (papules<br />
and burrows in the axillae, groin, or digital web<br />
spaces associated with complaints <strong>of</strong> nocturnal pruritus)<br />
occurs in HIV-infected patients with relatively<br />
normal immune function. However, as patients<br />
become progressively more immunosuppressed, the<br />
more contagious and fulminant forms <strong>of</strong> scabies<br />
become apparent. 267-269,271,272,282 This conversion<br />
from ordinary scabies to more severe and unusual<br />
infestations has been documented in individual<br />
patients who experience declines in their CD4 cell<br />
counts to below 200/mm 3 . 266,272,274,285 Still, as noted<br />
by Portu et al, 295 although low CD4 cell counts may<br />
be more commonly associated with the severe and<br />
unusual forms <strong>of</strong> scabies, these fulminant infections<br />
can occur in early stages <strong>of</strong> HIV disease.<br />
These severe and unusual forms <strong>of</strong> scabies can be<br />
divided into two overlapping and broad categories:
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
papular (also known as atypical or exaggerated) scabies<br />
and crusted (also known as Norwegian or<br />
hyperkeratotic) scabies. 285,299,300 The papular forms<br />
are characterized by generalized papules, each <strong>of</strong><br />
which is topped by a scabietic burrow, which may be<br />
scaly. Patients complain <strong>of</strong> severe pruritus with this<br />
form. 266,273,277,285 The crusted forms are characterized<br />
by thick, friable, white-gray plaques, which may<br />
also be diffuse, but are commonly localized to individual<br />
body regions including the scalp, face, back,<br />
buttocks, nails, and feet (Fig 11). The plaques are<br />
<strong>of</strong>ten associated with fissuring that may be mild to<br />
severe. 267-272 Furthermore, as a patient’s lesions<br />
become crusted, they tend to become less pruritic.<br />
The distinction between papular and crusted scabies<br />
is not mutually exclusive, and some reports document<br />
patients with lesions characteristic <strong>of</strong> both<br />
forms. 270,284<br />
Infestations may be mistaken for eczema, psoriasis,<br />
contact dermatitis, drug reactions, seborrheic<br />
dermatitis, Darier’s disease, or dermatophytosis.<br />
Scabies must be suspected in any HIV-infected person<br />
with an atypical or pruritic rash. Similarly, young<br />
patients with HIV risk factors in whom papular or<br />
crusted scabies develops without an apparent underlying<br />
cause should be suspected <strong>of</strong> having HIV infection.<br />
Skin scrapings are <strong>of</strong>ten diagnostic in crusted<br />
or papular scabies and may be taken from any nonexcoriated<br />
region or from underneath the nails; however,<br />
if scrapings are negative and clinical suspicion<br />
remains, a skin biopsy can be very helpful. 285,299,300<br />
It must be noted that a key feature <strong>of</strong> crusted scabies<br />
infestations in the HIV-infected patient is an<br />
exceptionally high mite burden. Whereas an immunocompetent<br />
host is estimated to have 10 to 15 live<br />
female mites during an infestation, 301 individual<br />
crusts in crusted scabies may harbor thousands <strong>of</strong><br />
mites. Furthermore, although the scabies mite has a<br />
limited life span (
424 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
reinfected from other untreated personal contacts or<br />
from improper cleaning <strong>of</strong> bedding and clothing.<br />
The CDC recommendation for HIV-infected<br />
patients with crusted or papular scabies is for “consultation<br />
with an expert.” 1 Five percent permethrin<br />
cream is the best topical agent currently available for<br />
treatment <strong>of</strong> crusted or papular scabies. 300 Although<br />
topical lindane preparations have been used frequently<br />
in published reports, this medicine has the<br />
potential for serious neurotoxicity. In crusted scabies,<br />
deep fissures <strong>of</strong>ten enhance the systemic absorption<br />
<strong>of</strong> lindane resulting in potentially high serum concentrations<br />
<strong>of</strong> the neurotoxin. Furthermore, many HIVpositive<br />
patients have AIDS-related neurologic<br />
changes, which may predispose them to any neurotoxic<br />
effects. At least one death in an HIV-infected<br />
patient with scabies has been attributed to lindane. 290<br />
For these reasons, permethrin is the preferred treatment<br />
in HIV-positive patients. 300<br />
Taplin and Meinking, 300 among others, have recommended<br />
ivermectin as an oral alternative to topical<br />
therapies for the treatment <strong>of</strong> scabies. Several<br />
studies 302-305 document the safety and efficacy <strong>of</strong><br />
ivermectin in the treatment <strong>of</strong> scabies, including one<br />
such study that evaluated the medicine’s effects on<br />
HIV-positive patients who were taking multiple medications<br />
including antiretrovirals and antifungals. 305<br />
However, no reports have directly compared the efficacy<br />
<strong>of</strong> ivermectin with the currently recommended<br />
regimens (permethrin or lindane), and it is not yet<br />
approved by the FDA for this purpose.<br />
In the treatment <strong>of</strong> crusted scabies, it is also clear<br />
that patients benefit from keratolytic agents (eg, 6%<br />
salicylic acid) or, if possible, manual debridement.<br />
This serves to decrease the patient’s mite load and to<br />
facilitate the penetration <strong>of</strong> topical medications.<br />
Some researchers support combined topical permethrin,<br />
keratolytics, and oral ivermectin as a potential<br />
regimen in the management <strong>of</strong> these patients. 298,300<br />
It is believed that the combination <strong>of</strong> topical therapy<br />
and oral therapy maximizes the penetration <strong>of</strong> antiscabietic<br />
medications into the crusts. Therapy for<br />
the infestation in crusted or papular scabies needs to<br />
be persistent because the high mite burdens in these<br />
patients are difficult to eradicate. Special attention<br />
should be paid to the head and neck as well as<br />
underneath the fingernail. Skin scrapings should be<br />
collected <strong>of</strong>ten, and treatment continued until<br />
repeated scrapings yield no mites. Permethrin treatments<br />
may be needed 2 to 3 times per week for up<br />
to 6 weeks to eradicate the menace.<br />
A unique complication that accompanies crusted<br />
scabies is bacteremia. This is seen when the<br />
patients have severe fissuring associated with their<br />
crusts and has led to the patients’ death on several<br />
occasions. Streptococcal, 268 staphylococcal, 271 and<br />
Pseudomonas spp 274,284 have caused bacteremia in<br />
patients with crusted scabies, and antibiotic prophylaxis<br />
appropriate to the bacterial flora pr<strong>of</strong>ile <strong>of</strong><br />
the hospital is highly recommended in these cases<br />
to avoid this complication. 283,288,299,300<br />
Pediculosis pubis<br />
Very little has been written about the effect that<br />
HIV infection has on infestation with Phthirus pubis.<br />
It appears that the ectoparasite behaves the same<br />
clinically regardless <strong>of</strong> HIV serostatus. The CDC recommends<br />
the same treatment for HIV-positive<br />
patients with pediculosis pubis as it does HIV-negative<br />
patients. 1 Permethrin 1% cream rinse applied for<br />
10 minutes, lindane 1% shampoo applied for 4 minutes,<br />
or pyrethrins with piperonyl butoxide applied<br />
for 10 minutes are all appropriate therapies when<br />
accompanied by appropriate decontamination <strong>of</strong><br />
bedding and clothing. Pediculosis <strong>of</strong> the eyes should<br />
be treated with an occlusive ophthalmic ointment<br />
twice daily for 10 days.<br />
In summary, STDs may enhance both the acquisition<br />
and the transmission <strong>of</strong> HIV. This relationship is<br />
especially true <strong>of</strong> STDs causing genital ulcers. STDs<br />
in HIV-seropositive persons may differ qualitatively<br />
or quantitatively, or both, in both clinical and laboratory<br />
parameters from STDs in immuncompetent<br />
persons. Such measures as education, which may<br />
lead to early recognition <strong>of</strong> the signs and symptoms<br />
<strong>of</strong> STDs, have the potential to positively affect the<br />
HIV epidemic. Therefore enhanced efforts should be<br />
devoted to the prevention and treatment <strong>of</strong> STDs.<br />
REFERENCES<br />
1. Centers for Disease Control and Prevention. 1998 Guidelines<br />
for the treatment <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>. MMWR<br />
1998;47(RR-1):1-116.<br />
2. Centers for Disease Control and Prevention. HIV prevention<br />
through early detection and treatment <strong>of</strong> other <strong>sexually</strong><br />
<strong>transmitted</strong> <strong>diseases</strong>—United States. MMWR 1998;47(RR-<br />
12):1-24.<br />
3. Wasserheit JN. Epidemiological synergy: interrelationships<br />
between human immunodeficiency virus infection and other<br />
<strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>. Sex Transm Dis 1992;29:61-77.<br />
4. Greenblatt RM, Lukehart SA, Plummer FA, Quinn TC, Critchlow<br />
CW, Ashley RL, et al. Genital ulceration as a risk factor for<br />
human immunodeficiency virus infection. AIDS 1988;2:47-50.<br />
5. Kreiss JK, Koech D, Plummer FA, Holmes KK, Lightfoote M, Piot<br />
P, et al. AIDS virus infection in Nairobi prostitutes. N Engl J Med<br />
1986;314:414-8.<br />
6. Plourde PS, Plummer FA, Pepin J, Agoki E, Moss G, Ombette J,<br />
et al. Human immunodeficiency virus type 1 infection in<br />
women attending a <strong>sexually</strong> <strong>transmitted</strong> disease clinic in<br />
Kenya. J Infect Dis 1992;166:86-92.<br />
7. Simonsen JN, Cameron DW, Gakinya MN, Ndinya-Achola JO,<br />
D’Costa LJ, Karasira P, et al. Human immunodeficiency virus<br />
infection among men with <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>. N<br />
Engl J Med 1988;319:274-8.
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
8. Plummer FA, Simonsen JN, Cameron DW, Ndinya-Achola JO,<br />
Kreiss JK, Gakinya MN, et al. C<strong>of</strong>actors in male-female sexual<br />
transmission <strong>of</strong> human immunodeficiency virus type 1. J<br />
Infect Dis 1991;163:233-9.<br />
9. Telzak EE, Chaisson MA, Bevier PJ, Stoneburner RL, Castro KG,<br />
Jaffe HN. HIV-1 seroconversion in patients with and without<br />
genital ulcer disease. <strong>An</strong>n Intern Med 1993;119:1181-6.<br />
10. Grosskurth H, Mosha F, Todd J, Mwijarubi E, Klokke A, Senkoro<br />
K, et al. Impact <strong>of</strong> improved treatment <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong><br />
<strong>diseases</strong> on HIV infection in rural Tanzania: randomized controlled<br />
trial. Lancet 1995;346:530-6.<br />
11. Plummer FA, Wainberg MA, Plourde P, Jessamine P, D’Costa LJ,<br />
Wamola IA, et al. Detection <strong>of</strong> human immunodeficiency virus<br />
type 1 (HIV-1) in genital ulcer exudate <strong>of</strong> HIV-1-infected men<br />
by culture and gene amplification. J Infect Dis 1990;161:810-1.<br />
12. Kreiss JK, Coombs R, Plummer F, Holmes KK, Nikora B, Cameron<br />
W, et al. Isolation <strong>of</strong> human immunodeficiency virus from genital<br />
ulcers in Nairobi prostitutes. J Infect Dis 1989;160:380-4.<br />
13. Schacker T, Ryncarz AJ, Goddard J, Diem K, Shaughnessy M,<br />
Corey L. Frequent recovery <strong>of</strong> HIV-1 from genital herpes simplex<br />
virus lesions in HIV-1-infected men. JAMA 1998;280:61-6.<br />
14. Cunningham AL, Turner RR, Miller AC, Para MF, Merigan TC.<br />
Evolution <strong>of</strong> recurrent herpes simplex lesions: an immunohistologic<br />
study. J Clin Invest 1985;75:226-33.<br />
15. Koelle DM, Abbo H, Peck A, Ziegweid K, Corey L. Direct recovery<br />
<strong>of</strong> HSV-specific T lymphocyte clones from recurrent genital<br />
HSV-2 lesions. J Infect Dis 1994;169:956-61.<br />
16. Heng MCY, Heng SY. Coinfection and synergy <strong>of</strong> human<br />
immunodeficiency virus-1 and herpes simplex virus-1. Lancet<br />
1994;343:255-8.<br />
17. De Vincenzi I. A longitudinal study <strong>of</strong> human immunodeficiency<br />
virus transmission by heterosexual partners. N Engl J<br />
Med 1994;331:341-6.<br />
18. Spinola SM, Orazi A, Arno JN, Fortney K, Kotylo P, Chen CY, et al.<br />
Haemophilus ducreyi elicits a cutaneous infiltrate <strong>of</strong> CD4 cells<br />
during experimental human infection. J Infect Dis 1996;173:<br />
394-402.<br />
19. Hook ED, Cannon RD, Nahmias AJ, Lee FF, Campbell CH, Glasser<br />
D, et al. Herpes simplex virus infection as a risk factor for<br />
human immunodeficiency virus infection in heterosexuals. J<br />
Infect Dis 1992;165:251-5.<br />
20. Boulos R, Ruff AJ, Nahmias A, Holt E, Harrison L, Magder L, et al.<br />
Herpes simplex virus type 2 infection, syphilis, and hepatitis B<br />
virus infection in Haitian women with human immunodeficiency<br />
virus type 1 and human T lymphotrophic virus type 1<br />
infections. J Infect Dis 1992;166:418-512.<br />
21. Stamm W, Handsfield H, Rompalo A, Ashley R, Roberts P, Corey<br />
L. The association between genital ulcer disease and acquisition<br />
<strong>of</strong> HIV infection in homosexual men. JAMA 1988;260:<br />
1429-33.<br />
22. Holmberg SD, Stewart JA, Gerber AR, Byers RH, Lee FK,<br />
O’Malley PM, et al. Prior herpes simplex virus type 2 infection<br />
as a risk factor for HIV infection. JAMA 1988;259:1048-50.<br />
23. Keet IP, Lee FK, van Griensven GJ, Lange JM, Nahmias A,<br />
Coutinho RA. HSV type-2 and other genital ulceration infections<br />
as a risk factor for HIV-1 acquisition. Genitourin Med<br />
1990;66:330-3.<br />
24. Gadkari DA, Quinn TC, Gangakhedkar RR, Mehendale SM,<br />
Divekar AD, Risbud AR, et al. HIV-1 DNA shedding in genital<br />
ulcers and its associated risk factors in Pune, India. J Acquir<br />
Immune Defic Syndr Hum Retrovirol 1998;18:277-81.<br />
25. Quinn TC, Cannon RO, Glasser D, Groseclose SL, Brathwaite WS,<br />
Fauci AS, et al. The association <strong>of</strong> syphilis with risk <strong>of</strong> human<br />
immunodeficiency virus infection in patients attending <strong>sexually</strong><br />
<strong>transmitted</strong> <strong>diseases</strong> clinics. Arch Intern Med 1990;150:<br />
1297-302.<br />
Czelusta, Yen-Moore, and Tyring 425<br />
26. Quinn TC, Glasser D, Cannon RO, Matuszak DL, Dunning RW,<br />
Kline RL, et al. Human immunodeficiency virus infection<br />
among patients attending clinics for <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong>.<br />
N Engl J Med 1988;318:197-203.<br />
27. Mertz KJ, Weiss JB, Webb RM, Levine WC, Lewis JS, Orle KA, et<br />
al. <strong>An</strong> investigation <strong>of</strong> genital ulcers in Jackson, Mississippi,<br />
with use <strong>of</strong> a multiplex polymerase chain reaction assay: high<br />
prevalence <strong>of</strong> chancroid and human immunodeficiency virus<br />
infection. J Infect Dis 1998;178:1060-6.<br />
28. O’Farrell N, Windsor I, Becker P. HIV infection among heterosexual<br />
attenders at a <strong>sexually</strong> <strong>transmitted</strong> <strong>diseases</strong> clinic in<br />
Durban. S Afr Med J 1991;80:17-20.<br />
29. O’Farrell N. Global eradication <strong>of</strong> donovanosis: an opportunity<br />
for limiting the spread <strong>of</strong> HIV-1 infection. Genitourin Med<br />
1995;71:27-31.<br />
30. Kinghorn GR. Genital herpes: natural history and treatment <strong>of</strong><br />
acute episodes. J Med Virol 1993;Suppl 1:33-8.<br />
31. Siegal FP, Lopez C, Hammer GS, Brown AE, Kornfeld SJ, Gold J,<br />
et al. Severe acquired immunodeficiency in male homosexuals,<br />
manifested by chronic perianal ulcerative herpes simplex<br />
lesions. N Engl J Med 1981;305:1439-44.<br />
32. Schomogyi M, Wald A, Corey L. Herpes simplex virus-2 infection:<br />
an emerging disease? Infect Dis Clin North Am 1998;12:<br />
47-61.<br />
33. Quinnan G, Masur H, Rook AH, Armstrong G, Fredrick WR,<br />
Epstein J, et al. Herpesvirus infections in the acquired immunodeficiency<br />
syndrome. JAMA 1984;252:72-7.<br />
34. Maier J, Bergman A, Ross M. Acquired immunodeficiency syndrome<br />
manifested by chronic primary genital herpes. Am J<br />
Obstet Gynecol 1986;155:756-8.<br />
35. Skinhoj P. Herpesvirus infections in the immunocompromised<br />
patient. Scand J Infect Dis 1985;47(Suppl):121-7.<br />
36. Bagdades E, Pillay D, Squire S, O’Neil C, Johnson MA, Griffiths<br />
PD. Relationship between herpes simplex virus ulceration and<br />
CD4+ cell counts in patients with HIV infection. AIDS 1992;<br />
6:1317-20.<br />
37. Augenbraun M, Feldman J, Chirgwin K, Zenilman J, Clarke L,<br />
DeHovitz J, et al. Increased genital shedding <strong>of</strong> herpes simplex<br />
virus type 2 in HIV-seropositive women. <strong>An</strong>n Intern Med 1995;<br />
123:845-7.<br />
38. Centers for Disease Control. 1993 Revised classification system<br />
for HIV infection and expanded surveillance case definition<br />
for AIDS among adolescents and adults. MMWR 1992;41(RR-<br />
17):1-19.<br />
39. Tayal SC, Pattman RS, McLelland J, Sviland L, Snow MH. <strong>An</strong><br />
indolent penile herpetic ulcer in a patient with previously<br />
undiagnosed human immunodeficiency virus infection. Br J<br />
Dermatol 1998;138:334-6.<br />
40. Horner P, Harris J. A herpes simplex skin ulcer in a patient with<br />
AIDS: an unusual presentation. Int J STD AIDS 1990;1:288-9.<br />
41. Gretzula J, Penneys N. Complex viral and fungal skin lesions <strong>of</strong><br />
patients with acquired immunodeficiency syndrome. J Am<br />
Acad Dermatol 1987;16:1151-4.<br />
42. Smith K, Skelton H, Frissman D, <strong>An</strong>gritt P.Verrucous lesions secondary<br />
to DNA viruses in patients infected with the human<br />
immunodeficiency virus in association with increased factor<br />
X<strong>III</strong>a–positive dermal dendritic cells. J Am Acad Dermatol<br />
1992;27:943-50.<br />
43. Tong P, Mutasim D. Herpes simplex virus infection masquerading<br />
as condyloma acuminata in a patient with HIV disease. Br<br />
J Dermatol 1996;134:797-800.<br />
44. Smith K, Skelton H, James W, <strong>An</strong>gritt P. Concurrent epidermal<br />
involvement <strong>of</strong> cytomegalovirus and herpes simplex virus in<br />
two HIV-infected patients. J Am Acad Dermatol 1991;25:500-6.<br />
45. Husak R, Tebbe B, Goerdt S, Wolfer LU, Zeichardt H, St<strong>of</strong>fler-<br />
Meilicke M, et al. Pseudotumor <strong>of</strong> the tongue caused by her-
426 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
pes simplex virus type 2 in an HIV-1 infected immunosuppressed<br />
patient. Br J Dermatol 1998;139:118-21.<br />
46. Nelson J, Ghazal P, Wiley C. Role <strong>of</strong> opportunistic viral infections<br />
in AIDS. AIDS 1990;4:1-10.<br />
47. Schacker T, Hu H, Koelle DM, Zeh J, Saltzman R, Boon R, et al.<br />
Famciclovir for the suppression <strong>of</strong> symptomatic and asymptomatic<br />
herpes simplex virus reactivation in HIV-infected persons:<br />
a double-blind, placebo controlled trial. <strong>An</strong>n Intern Med<br />
1998;128:21-8.<br />
48. Augenbraun MH, McCormack WM. Sexually <strong>transmitted</strong> <strong>diseases</strong><br />
in HIV-infected persons. Infect Dis Clin North Am 1994;8:<br />
439-48.<br />
49. Pereira FA. Herpes simplex: evolving concepts. J Am Acad<br />
Dermatol 1996;35:503-20.<br />
50. Lawrence A, Bell A. Valacyclovir for prevention <strong>of</strong> recurrent<br />
herpes virus infection in HIV-infected individuals: a double<br />
blind controlled trial. 8th European Congress <strong>of</strong> Clinical<br />
Microbiology and Infectious Diseases, Lausanne, Switzerland,<br />
May 25-28, 1997.<br />
51. Ioannidis J, Collier A, Cooper D, Corey L, Fiddian AP, Gazzard<br />
BG, et al. Clinical efficacy <strong>of</strong> high-dose acyclovir in patients<br />
with human immunodeficiency virus infection: a meta-analysis<br />
<strong>of</strong> randomized individual patient data. J Infect Dis 1998;<br />
178:349-59.<br />
52. Douglas JM, Critchlow C, Benedetti J, Mertz GJ, Connor JD,<br />
Hintz MA, et al. A double-blind study <strong>of</strong> oral acyclovir for suppression<br />
<strong>of</strong> recurrences <strong>of</strong> genital herpes simplex virus infection.<br />
N Engl J Med 1984;310:1551-6.<br />
53. Strauss SE, Takiff HE, Seidlin M, Bachrach S, Lininger L,<br />
DiGiovanna JJ, et al. Suppression <strong>of</strong> frequently recurring genital<br />
herpes: a placebo-controlled double-blind trial <strong>of</strong> oral acyclovir.<br />
N Engl J Med 1984;310:1545-50.<br />
54. Locke L, Young C, Saltzman R. Famciclovir safety experience in<br />
long-term treatment and in immunocompromised patients.<br />
8th International Congress on Infectious Diseases, Boston,<br />
Massachusetts, May 15-18, 1998.<br />
55. Burnside A, Preston R, Crann R, Young C. Famciclovir for suppression<br />
<strong>of</strong> recurrent genital herpes in HIV-infected patients.<br />
Presented at the 36th <strong>An</strong>nual Meeting <strong>of</strong> the Infectious<br />
Disease Society <strong>of</strong> America, Denver, Colorado, Nov 12-15,<br />
1998.<br />
56. Stein DS, Graham NMH, Park LP, Hoover DR, Phair JP, Detels R,<br />
et al.The effect <strong>of</strong> the interaction <strong>of</strong> acyclovir with zidovudine<br />
on progression to AIDS and survival. <strong>An</strong>n Intern Med 1995;<br />
121:100-8.<br />
57. Englund JA, Zimmerman ME, Swierkosz EM, Goodman JL,<br />
Schall DR, Balfour HH. Herpes simplex virus resistant to acyclovir:<br />
a study in a tertiary care center. <strong>An</strong>n Intern Med 1990;<br />
112:416-22.<br />
58. Golden M, Kim S, Hammer S, Ladd E, Schaffer PA, De Luca N, et<br />
al. Activation <strong>of</strong> human immunodeficiency virus by herpes<br />
simplex virus. J Infect Dis 1992;166:494-9.<br />
59. Griffiths P. Studies to define viral c<strong>of</strong>actors for human immunodeficiency<br />
virus. Infect Agents Dis 1992;1:237-44.<br />
60. Kucera L, Leake E, Iyer N, Raben D, Myrvik Q. Human immunodeficiency<br />
virus type 1 (HIV-1) and herpes simplex virus type<br />
2 (HSV-2) can coinfect and simultaneously replicate in the<br />
same human CD4 cell: effect <strong>of</strong> coinfection on infectious HSV-<br />
2 and HIV-1 replication. AIDS Res Hum Retroviruses 1990;6:<br />
641-7.<br />
61. Mole L, Ripich S, Margolis D, Holodnif M. The impact <strong>of</strong> active<br />
herpes simplex virus infection on human immunodeficiency<br />
virus load. J Infect Dis 1997;176:766-70.<br />
62. Gallant JE, Moore RD, Keruly J, Richman DD, Chaisson R.<br />
Zidovudine epidemiology study group: lack <strong>of</strong> association<br />
between acyclovir use and survival in patients with advanced<br />
human immunodeficiency virus disease treated with zidovudine.<br />
J Infect Dis 1995;172:346-52.<br />
63. Reyes M, Graber J, Reeves W. Acyclovir resistant HSV: preliminary<br />
results from a national surveillance system. International<br />
Conference on Emerging Infectious Diseases, Atlanta, Georgia,<br />
March 8-11, 1998.<br />
64. Fife K. Recurrence and resistance pattern <strong>of</strong> herpes simplex<br />
virus following cessation <strong>of</strong> greater than 6 years <strong>of</strong> chronic<br />
suppression with acyclovir. J Infect Dis 1994;169:1338-41.<br />
65. Severson JL, Tyring SK. The interrelationships between herpes<br />
simplex viruses and human immunodeficiency virus infections.<br />
Arch Dermatol 1999;135:1393-7.<br />
66. Erlich K, Mills J, Chatis P, Mertz GJ, Busch DF, Follansbee SE, et<br />
al. Acyclovir-resistant herpes simplex virus infections in<br />
patients with the acquired immunodeficiency syndrome. N<br />
Engl J Med 1989;320:293-6.<br />
67. Safrin S, Cherrington J, Jaffe HS. Clinical uses <strong>of</strong> cid<strong>of</strong>ovir. Rev<br />
Med Virol 1997;7:145-56.<br />
68. Safrin S, Kemmerly S, Plotkin B, Smith T, Weissbach N, De<br />
Veranez D, et al. Foscarnet resistant herpes simplex virus infection<br />
in patients with AIDS. J Infect Dis 1994;169:193-6.<br />
69. Snoeck R, <strong>An</strong>drei G, Gerard M, Silverman A, Heddeman A,<br />
Balzarini J, et al. Successful treatment <strong>of</strong> progressive mucocutaneous<br />
infection due to acyclovir and foscarnet resistant herpes<br />
simplex virus with (S)-1-(3-hydroxy-2phosphonylmethoxypropyl)<br />
cytosine (HPMPC). Clin Infect Dis 1994;18:<br />
570-8.<br />
70. Sacks SL, Shafran SD, Diaz-Mitoma F, Trottier S, Sibbald RG,<br />
Hughes A, et al. A multicenter phase I/II dose escalation study<br />
<strong>of</strong> single-dose cid<strong>of</strong>ovir gel for treatment <strong>of</strong> recurrent genital<br />
herpes. <strong>An</strong>timicrob Agents Chemother 1998;42:2996-9.<br />
71. Johns DR, Tierney M, Felsenstein D. Alteration in the natural<br />
history <strong>of</strong> neurosyphilis by concurrent infection with the<br />
human immunodeficiency virus. N Engl J Med 1987;316:1569-<br />
72.<br />
72. Brandon WR, Boulos LM, Morse A. Determining the prevalence<br />
<strong>of</strong> neurosyphilis in a cohort co-infected with HIV. Int J STD<br />
AIDS 1993;4:99-101.<br />
73. Musher DM, Hamill RK, Baughn RE. Effect <strong>of</strong> human immunodeficiency<br />
virus infection on the course <strong>of</strong> syphilis and on the<br />
response to treatment. <strong>An</strong>n Intern Med 1990;113:872-81.<br />
74. O’Mahony C, Rodgers C, Mendelsohn S, Sissons G, McKay A,<br />
Devine J, et al. Rapidly progressive syphilis in early HIV infection.<br />
Int J STD AIDS 1997;8:275-7.<br />
75. Hutchinson CM, Hook EW, Shepard M, Verley J, Rompalo AM.<br />
Altered clinical presentation <strong>of</strong> early syphilis in patients with<br />
HIV infection. <strong>An</strong>n Intern Med 1994;121:94-100.<br />
76. Sch<strong>of</strong>er H, Imh<strong>of</strong> M, Thoma-Greber E, Brockmeyer NH,<br />
Hartmann M, Gerken G, et al. Active syphilis in HIV infection: a<br />
multicenter retrospective survey. Genitourin Med 1996;72:<br />
176-81.<br />
77. Bari M, Shulkin D, Abell E. Ulcerative syphilis in acquired<br />
immunodeficiency syndrome: a case <strong>of</strong> precocious tertiary<br />
syphilis in a patient infected with human immunodeficiency<br />
virus. J Am Acad Dermatol 1989;21:1310-2.<br />
78. Dowell ME, Ross PG, Musher DM, Cate TR, Boughn RE. Response<br />
<strong>of</strong> latent syphilis or neurosyphilis to ceftriaxone therapy in persons<br />
infected with HIV. Am J Med 1992;93:481-8.<br />
79. Rolfs RT, Joesoef MR, Hendershot EF, Rompalo AM,<br />
Augenbraun MH, Chiu M, et al. A randomized trial <strong>of</strong> enhanced<br />
therapy for early syphilis in patients with and without HIV<br />
infection. N Engl J Med 1997;337:307-14.<br />
80. Gordon SM, Eaton ME, George R, Larsen S, Lukehart SA,<br />
Kuypers J, et al.The response <strong>of</strong> symptomatic neurosyphilis to<br />
high-dose intravenous penicillin G in patients with HIV infection.<br />
N Engl J Med 1994;331:1469-73.
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
81. Hook EW, Marra CM. Acquired syphilis in adults. N Engl J Med<br />
1992;326:1060-9.<br />
82. Katz DA, Berger JR, Duncan RC. Neurosyphilis: a comparative<br />
study <strong>of</strong> the effects <strong>of</strong> infection with HIV. Arch Neurol<br />
1993;50:243-9.<br />
83. Malone JL, Wallace MR, Hendrick BB, La Rocco A, Tonon E,<br />
Brodine SK, et al. Syphilis and neurosyphilis in a HIV type-1<br />
seropositive population: evidence for frequent serologic<br />
relapse after therapy. Am J Med 1995;99:55-63.<br />
84. Rolfs RT. Treatment <strong>of</strong> syphilis, 1993. Clin Infect Dis<br />
1995;20(Suppl 1):S23-S38.<br />
85. Dibbern DA, Ray SC. Recrudescence <strong>of</strong> treated neurosyphilis in<br />
a patient with human immunodeficiency virus. Mayo Clin Proc<br />
1999;74:53-6.<br />
86. Morgello S, Laufer H. Quarternary neurosyphilis in a Haitian<br />
man with human immunodeficiency virus infection. Hum<br />
Pathol 1989;20:808-11.<br />
87. Hay P, Tam F, Kitchen V, Horner S, Bridger J, Weber J, et al.<br />
Gummatous lesions in men infected with human immunodeficiency<br />
virus and syphilis. Genitourin Med 1990;66:374-9.<br />
88. McLeish W, Pulido J, Holland S, Culbertson WW,Winward K.The<br />
ocular manifestations <strong>of</strong> syphilis in the human immunodeficiency<br />
virus type 1 infected host. Ophthalmology 1990;97:<br />
196-203.<br />
89. Shalaby IA, Dunn JP, Semba RD, Jabs DA. Syphilitic uveitis in<br />
HIV-infected patients. Arch Ophthalmol 1997;115:469-73.<br />
90. Olmos JM, Fernandez-Ayala M, Gutierrez JA, Val JF, Gonzalez-<br />
Marcias J. Superior vena cava syndrome secondary to<br />
syphilitic aneurysm <strong>of</strong> the ascending aorta in a human<br />
immunodeficiency virus-infected patient. Clin Infect Dis 1998;<br />
27:1331-2.<br />
91. Rompalo AM, Cannon RO, Quinn TC, Hook EW. Association <strong>of</strong><br />
biologic false-positive reactions for syphilis with human<br />
immunodeficiency virus infection. J Infect Dis 1992;165:1124-<br />
6.<br />
92. Capoccia A, Ranieri R, Busnelli M, Passaretti B, Milella AM,<br />
Vecchi L. Serologic study on the prevalence <strong>of</strong> HIV, HBV infection<br />
and on the false-positive reaction <strong>of</strong> VDRL at a prison.<br />
Minerva Med 1991;82:125-30.<br />
93. Joyanes B, Borobio MV, Arquez JM, Perea EJ.The association <strong>of</strong><br />
false-positive rapid plasma reagin results and HIV infection.<br />
Sex Transm Dis 1998;25:569-71.<br />
94. Hernandez-Aguado I, Bolumar F, Moreno R, Pardo FJ, Torres N,<br />
Belda J, Espacio A. False-positive tests for syphilis associated<br />
with human immunodeficiency virus and hepatitis B virus<br />
infection among intravenous drug abusers: Valencia Study<br />
Group on HIV Epidemiology. Eur J Clin Microbiol Infect Dis<br />
1998;17:784-7.<br />
95. Goeman J, Kivuvu M, Nzila N, Behets F, Edidi B, Gneore E, et al.<br />
Similar serological response to conventional therapy for<br />
syphilis among HIV-positive and HIV-negative women.<br />
Genitourin Med 1995;71:275-9.<br />
96. Gourevitch MN, Selwyn PA, Davenny K, Buono D, Schoenbaum<br />
EE, Klein RS, et al. Effects <strong>of</strong> HIV infection on the serologic manifestations<br />
and response to treatment <strong>of</strong> syphilis in intravenous<br />
drug users. <strong>An</strong>n Intern Med 1993;118:350-5.<br />
97. Marra CM, Longstreth WT, Maxwell C, Lukehart SA. Resolution<br />
<strong>of</strong> serum and cerebrospinal fluid abnormalities after treatment<br />
<strong>of</strong> neurosyphilis: influence <strong>of</strong> concomitant HIV infection.<br />
Sex Transm Dis 1996;23:184-9.<br />
98. Telzak EE, Greenburg MS, Harrison J, Stoneburner RL, Schultz S.<br />
Syphilis treatment response in HIV-infected individuals. AIDS<br />
1991;5:591-5.<br />
99. Yinnon AM, Coury-Doniger P, Polito R, Reichman RC. Serologic<br />
response to treatment <strong>of</strong> syphilis in patients with HIV infection.<br />
Arch Intern Med 1996;156:321-5.<br />
Czelusta, Yen-Moore, and Tyring 427<br />
100. Hicks CB, Benson PM, Lupton GP, Tramont EC. Seronegative<br />
secondary syphilis in a patient infected with the human<br />
immunodeficiency virus (HIV) with Kaposi’s sarcoma. <strong>An</strong>n<br />
Intern Med 1987;107:492-5.<br />
101. Radolf JD, Kaplan RP. Unusual manifestations <strong>of</strong> secondary<br />
syphilis and abnormal humoral immune response to<br />
Treponema pallidum antigens in a homosexual man with<br />
asymptomatic human immunodeficiency virus infection. J Am<br />
Acad Dermatol 1988;18:423-8.<br />
102. Bowen DL, Lane HC, Fauci AS. Immunopathogenesis <strong>of</strong> the<br />
acquired immunodeficiency syndrome. <strong>An</strong>n Intern Med 1985;<br />
103:704-9.<br />
103. Hutchinson CM, Rompalo AM, Reichart CA, Hook EW.<br />
Characteristics <strong>of</strong> syphilis patients attending Baltimore STD<br />
clinics: multiple high risk subgroups and interactions with HIV<br />
infection. Arch Intern Med 1991;151:511-6.<br />
104. Tikjob G, Russel M, Petersen CS, Gerst<strong>of</strong>t J, Kobayasi T.<br />
Seronegative secondary syphilis in a patient with AIDS: identification<br />
<strong>of</strong> Treponema pallidum in a biopsy specimen. J Am<br />
Acad Dermatol 1991;24:506-8.<br />
105. Johnson PD, Graves SR, Stewart L,Warren R, Dwyer B, Lucas CR.<br />
Specific syphilis serological tests may become negative in HIV<br />
infection. AIDS 1991;5:419-23.<br />
106. Fonseca E, Garcia-Silva J, del Pozo J, Yebra MT, Cuervas J,<br />
Contreras F. Syphilis in an HIV-infected patient misdiagnosed<br />
as leprosy. J Cutan Pathol 1999;26:51-4.<br />
107. Bogaerts J, Ricart CA,Van Dyck E, Piot P.The etiology <strong>of</strong> genital<br />
ulceration in Rwanda. Sex Transm Dis 1989;16:123-6.<br />
108. Schmid GP, Sanders LL, Blount JH, Alexander ER. Chancroid in<br />
the United States: reestablishment <strong>of</strong> an old disease. JAMA<br />
1987;258:3265-8.<br />
109. Jones C, Rosen T, Clarridge J, Collins S. Chancroid: results from<br />
an outbreak in Houston, Texas. South Med J 1990;83:1384-8.<br />
110. Ortiz-Zepeda C, Hernandez-Perez E, Marroquin-Burgos R.<br />
Gross and microscopic features in chancroid: a study in 200<br />
new culture-proven cases in San Salvador. Sex Transm Dis<br />
1994;21:112-7.<br />
111. Manget-Velasco CS, Borbujo-Martinez J, Manzano-de<br />
Arostegui JA, Calderon-Ubeda J, Toribio-Da Pena R, Casado-<br />
Jiminez M. S<strong>of</strong>t chancroid: 4 clinical cases. Atencion Primaria<br />
1993;12:667-70.<br />
112. Tyndall MW, Plourde PJ, Agoki E, Malisa W, Ndinya-Achola JO,<br />
Plummer FA, et al. Fleroxacin in the treatment <strong>of</strong> chancroid: an<br />
open study in men seropositive or seronegative for the<br />
human immunodeficiency virus type 1. Am J Med 1993;<br />
94(Suppl 3A):85S-8S.<br />
113. Kimani J, Bwayo JJ, <strong>An</strong>zala AO, MacLean I, Mwatha A, Choudri<br />
SH. Low dose erythromycin regimen for the treatment <strong>of</strong><br />
chancroid. East Afr Med J 1995;72:645-8.<br />
114. King R, Choudhri SH, Nasio J, Gough J, Nagelkerke NJ, Plummer<br />
FA, et al. Clinical and in situ cellular responses to Haemophilus<br />
ducreyi in the presence or absence <strong>of</strong> HIV infection. Int J STD<br />
AIDS 1998;9:531-6.<br />
115. Quale J, Teplitz E, Augenbraun M. Atypical presentation <strong>of</strong><br />
chancroid in a patient infected with the human immunodeficiency<br />
virus. Am J Med 1990;88(5N):43N-44N.<br />
116. Magro CM, Crowson AN, Alfa M, Nath A, Ronald A, Ndinya-<br />
Achola JO. A morphological study <strong>of</strong> penile chancroid lesions<br />
in human immunodeficiency virus (HIV)-positive and -negative<br />
African men with a hypothesis concerning the role <strong>of</strong><br />
chancroid in HIV transmission. Hum Pathol 1996;27:1066-70.<br />
117. MacDonald KS, Cameron DW, D’Costa LJ, Ndinya-Achola JO,<br />
Plummer FA, Ronald AR. Evaluation <strong>of</strong> fleroxacin (RO 23-6240)<br />
as single-oral-dose therapy <strong>of</strong> culture-proven chancroid in<br />
Nairobi, Kenya. <strong>An</strong>timicrob Agents Chemother 1989;33:612-4.<br />
118. Plourde PJ, D’Costa LJ, Agoki E, Ombette J, Ndinya-Achola JO,
428 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
Slaney LA, et al. A randomized, double-blind study <strong>of</strong> the efficacy<br />
<strong>of</strong> fleroxacin versus trimethoprim-sulfamethoxazole in<br />
men with culture-proven chancroid. J Infect Dis 1992;165:949-<br />
52.<br />
119. Tyndall M, Malisa M, Plummer FA, Ombetti J, NdinyaAchola JO,<br />
Ronald AR. Ceftriaxone no longer predictably cures chancroid<br />
in Kenya. J Infect Dis 1993;167:469-71.<br />
120. Tyndall M, Agoki E, Plummer FA, Malisa W, Ndinya-Achola JO,<br />
Ronald AR. Single dose azithromycin for the treatment <strong>of</strong><br />
chancroid: a randomized comparison with erythromycin. Sex<br />
Transm Dis 1994;21:231-4.<br />
121. Hart G. Donovanosis. Clin Infect Dis 1997;25:24-32.<br />
122. Rosen T, Tschen JA, Ramsdell W, Moore J, Markham B.<br />
Granuloma inguinale. J Am Acad Dermatol 1984;11:433-7.<br />
123. Richens J. The diagnosis and treatment <strong>of</strong> donovanosis (granuloma<br />
inguinale). Genitourin Med 1991;67:441-52.<br />
124. Jamkhedkar PP, Hira SK, Shr<strong>of</strong>f HJ, Lanjewar DN. Clinico-epidemiologic<br />
features <strong>of</strong> granuloma inguinale in the era <strong>of</strong><br />
acquired immune deficiency syndrome. Sex Transm Dis 1998;<br />
25:196-200.<br />
125. Hoosen AA, Mphatsoe M, Kharsany AB, Moodley J, Bassa A,<br />
Bramdev A. Granuloma inguinale in association with pregnancy<br />
and HIV infection. Int J Gynecol Obstet 1996;53:133-8.<br />
126. Sanders CJG. Extragenital donovanosis in a patient with AIDS.<br />
Sex Transm Inf 1998;74:142-3.<br />
127. Jardim ML, Barros ER, Silveria M. Donovanosis in AIDS patients:<br />
description <strong>of</strong> two cases. <strong>An</strong> Bras Dermatol Sifilogr 1990;65:<br />
175-7.<br />
128. Maniar JK, Desai V. Genital ulcer <strong>diseases</strong> and HIV status correlation<br />
in Bombay, India. Presented at the 8th International<br />
Conference on AIDS, Amsterdam, Netherlands, July 19-24,<br />
1992.<br />
129. Manders SM, Baxter JD. Granuloma inguinale and HIV: a<br />
unique presentation and novel treatment regimen. J Am Acad<br />
Dermatol 1997;37:494-6.<br />
130. Becker LE. Lymphogranuloma venereum. Int J Dermatol 1976;<br />
15:26-33.<br />
131. Mauff AC, Ballard RC, Koornh<strong>of</strong> HJ. Problems in the diagnosis<br />
<strong>of</strong> lymphogranuloma venereum: a review <strong>of</strong> 6 cases. S Afr Med<br />
J 1983;63:55-6.<br />
132. Thorsteinsson SB. Lymphogranuloma venereum: review <strong>of</strong><br />
clinical manifestations, epidemiology, diagnosis, and treatment.<br />
Scand J Infect Dis 1982;32(Suppl):127-31.<br />
133. Scieux C, Barnes R, Bianchi A, Casin I, Morel P, Perol Y.<br />
Lymphogranuloma venereum: 27 cases in Paris. J Infect Dis<br />
1989;160:662-8.<br />
134. Heaton S, Hammerschlag MR, Roblin PM, DiPasquale RC.<br />
Lymphogranuloma venereum in a pregnant woman. Sex<br />
Transm Dis 1988;15:148-9.<br />
135. Buus DR, Pflugfelder SC, Schachter J, Miller D, Forster RK.<br />
Lymphogranuloma venereum conjunctivitis with a marginal<br />
corneal perforation. Ophthalmoogyl 1988;95:799-802.<br />
136. Beutner KR, Tyring SK. Human papillomavirus and human disease.<br />
Am J Med 1997;102(Suppl 5A):9-15.<br />
137. Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto<br />
J, et al. Prevalence <strong>of</strong> human papillomavirus in cervical cancer:<br />
a worldwide perspective. J Natl Cancer Inst 1995;87:796-802.<br />
138. Hill SA, Coghill SB. Human papillomavirus in squamous cell<br />
carcinoma <strong>of</strong> the anus. Lancet 1986;2:1333.<br />
139. Beckmann AM, Daling JR, Sherman KJ, Maden C, Miller BA,<br />
Coates RJ, et al. Human papillomavirus infection and anal cancer.<br />
Int J Cancer 1989;43:1042-9.<br />
140. Kiviat N, Rompalo A, Bowden R, Galloway D, Holmes KK, Corey<br />
L, et al. <strong>An</strong>al human papillomavirus among human immunodeficiency<br />
virus-seropositive and -seronegative men. J Infect<br />
Dis 1990;162:358-61.<br />
141. Palefsky J, Gonzales J, Greenblatt R, Ahn DK, Hollander H. <strong>An</strong>al<br />
intraepithelial neoplasia and anal papillomavirus infection<br />
among homosexual males with group IV HIV disease. JAMA<br />
1990;263:2911-6.<br />
142. Critchlow CW, Holmes KK, Wood R, Krueger L, Dunphy C,<br />
Vernon DA, et al. Association <strong>of</strong> human immunodeficiency<br />
virus and anal human papillomavirus infection among homosexual<br />
men. Arch Intern Med 1992;152:1673-6.<br />
143. Palefsky JM, Shiboski S, Moss A. Risk factors for anal human<br />
papillomavirus infection and anal cytologic abnormalities in<br />
HIV-positive and HIV-negative homosexual men. J Acquir<br />
Immune Defic Syndr 1994;7:599-606.<br />
144. Williams AB, Darragh TM, Vranizan K, Ochia C, Moss AR,<br />
Palefsky JM. <strong>An</strong>al and cervical human papillomavirus infection<br />
and risk <strong>of</strong> anal and cervical epithelial abnormalities in human<br />
immunodeficiency virus-infected women. Obstet Gynecol<br />
1994;83:205-11.<br />
145. Breese PL, Judson FN, Penley KA, Douglas JM. <strong>An</strong>al human<br />
papillomavirus infection among homosexual and bisexual<br />
men: prevalence <strong>of</strong> type specific infection and association<br />
with human immunodeficiency virus. Sex Transm Dis 1995;<br />
22:7-14.<br />
146. Aynaud O, Piron D, Barrasso R, Poveda JD. Comparison <strong>of</strong> clinical,<br />
histological, and virological symptoms <strong>of</strong> HPV in HIV-1<br />
infected men and immunocompetent subjects. Sex Transm<br />
Infect 1998;74:32-4.<br />
147. Vernon SD, Reeves WC, Clancy KA, Laga M, St Louis M, Gary HE,<br />
et al. A longitudinal study <strong>of</strong> human papillomavirus DNA<br />
detection in human immunodeficiency virus type 1-seropositive<br />
and seronegative women. J Infect Dis 1994;169:1108-12.<br />
148. Sun XW, Ellerbrock TV, Lungu O, Chaisson MA, Bush TJ, Wright<br />
TC. Human papillomavirus infection in human immunodeficiency<br />
virus-seropositive women. Obstet Gynecol 1995;85:<br />
680-6.<br />
149. Gemignani M, Maiman M, Fruchter RG, Arrastia CD, Gibbon D,<br />
Ellison T. CD4 lymphocytes in women with invasive and preinvasive<br />
cervical neoplasia. Gynecol Oncol 1995;59:364-9.<br />
150. Chopra KF, Tyring SK. The impact <strong>of</strong> the human immunodeficiency<br />
virus on the human papillomavirus epidemic. Arch<br />
Dermatol 1997;133:629-33.<br />
151. Palefsky JM. Cutaneous and genital HPV-associated lesions in<br />
HIV-infected patients. Clin Dermatol 1997;15:439-47.<br />
152. Arany I, Evans T, Tyring SK. Tissue specific HPV expression and<br />
downregulation <strong>of</strong> local immune responses in condylomas<br />
from HIV seropositive individuals. Sex Transm Infect 1998;74:<br />
349-53.<br />
153. Arany I, Tyring SK. Systemic immunosuppression by HIV infection<br />
influences HPV transcription and thus local immune<br />
responses in condyloma acuminatum. Int J STD AIDS 1998;<br />
9:268-71.<br />
154. Rabkin CS, Yellin F. Cancer incidence in a population with a<br />
high prevalence <strong>of</strong> infection with human immunodeficiency<br />
virus type 1. J Natl Cancer Inst 1994;86:1711-6.<br />
155. Kurman RJ, Henson DE, Herbst AL, Noller KL, Schiffman MH,<br />
National Cancer Institute Workshop. Interim guidelines for<br />
management <strong>of</strong> abnormal cervical cytology. JAMA 1994;<br />
271:1866-9.<br />
156. Maiman M, Tarricone N, Vieira J, Suarez J, Serur E, Boyce JG.<br />
Colposcopic evaluation <strong>of</strong> human immunodeficiency virusseropositive<br />
women. Obstet Gynecol 1991;78:84-8.<br />
157. Wright T, Ellerbrock TV, Chiasson MA, Van Devanter N, Sun XW.<br />
Cervical intraepithelial neoplasia in women infected with<br />
human immunodeficiency virus: prevalence, risk factors, and<br />
validity <strong>of</strong> Papanicolaou smears: New York Cervical Disease<br />
Study. Obstet Gynecol 1994;84:591-7.<br />
158. Bryan JT, Stoler MH, Tyring SK, McClowry T, Fife KH, Brown DR.
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
High-grade dysplasia in genital warts from two patients<br />
infected with the human immunodeficiency virus. J Med Virol<br />
1998;54:69-73.<br />
159. Unger ER,Vernon SD, Lee DR, Miller DL, Sharma S, Clancy KA, et<br />
al. Human papillomavirus type in anal epithelial lesions is<br />
influenced by human immunodeficiency virus. Arch Pathol<br />
Lab Med 1997;121:820-4.<br />
160. Brown DR, Bryan JT, Cramer H, Katz BP, Handy V, Fife KH.<br />
Detection <strong>of</strong> multiple human papillomavirus types in condyloma<br />
acuminata from immunosuppressed patients. J Infect<br />
Dis 1994;170:759-65.<br />
161. Brown T, Tyring SK, Yen-Moore A. <strong>An</strong> <strong>overview</strong> <strong>of</strong> <strong>sexually</strong> <strong>transmitted</strong><br />
<strong>diseases</strong>. <strong>Part</strong> II. J Am Acad Dermatol 1999;41:661-77.<br />
162. Modesto VL, Gottesman L. Sexually <strong>transmitted</strong> <strong>diseases</strong> and<br />
anal manifestations <strong>of</strong> AIDS. Surg Clin North Am 1994;74:<br />
1433-64.<br />
163. Weiss EG, Wexner SD. Surgery for anal lesions in HIV-infected<br />
patients. <strong>An</strong>n Med 1995;27:467-75.<br />
164. Kilewo CD, Urassa WK, Pallangyo K, Biberfeld G, Wigzell H.<br />
Response to podophyllotoxin <strong>of</strong> genital warts in relation to<br />
HIV-1 infection among patients in Dar es Salaam, Tanzania. Int<br />
J STD AIDS 1995;6:114-6.<br />
165. Petersen CS,Weismann K. Quercetin and kaempherol: an argument<br />
against the use <strong>of</strong> podophyllin. Genitourin Med 1995;<br />
71:92-3.<br />
166. Zarcone R, Addonizio D, Voto RI, Cardone G, Di Stefano M,<br />
Cardone A. Therapeutic prospects <strong>of</strong> natural alpha interferon<br />
from normal human leucocytes in the treatment <strong>of</strong> genital<br />
condylomata in HIV-positive women. Clin Exp Obstet Gynecol<br />
1994;21:173-6.<br />
167. Frega A, di Renzi P, Stanella P, Pachi A. Management <strong>of</strong> human<br />
papillomavirus vulvo-perineal infection with systemic β-interferon<br />
and thymostimulin in HIV-positive patients. Int J<br />
Gynecol Obstet 1994;44:255-8.<br />
168. Conant MA, Opp KM, Gilson RJC, Shupack JL, Friedman-Kien<br />
AE, HPV Study Group. Imiquimod’s success in HIV-positive<br />
patients with external genital warts. Presented as a poster<br />
(#225) at the 56th <strong>An</strong>nual Meeting <strong>of</strong> the American Academy<br />
<strong>of</strong> <strong>Dermatology</strong>, Orlando, Florida, Feb 27-March 4, 1998.<br />
169. Tyring SK, Douglas J, Corey L, Kriesel J, Solomon L, Bowden B,<br />
et al. A phase I/II study <strong>of</strong> cid<strong>of</strong>ovir gel for refractory condyloma<br />
acuminatum in patients with HIV infection. Presented as a<br />
poster (#296) at the 55th <strong>An</strong>nual Meeting <strong>of</strong> the American<br />
Academy <strong>of</strong> <strong>Dermatology</strong>, San Francisco, California, March 21-<br />
26, 1997.<br />
170. Orlando G, Fasolo MM, Signori R, Schiavini M, Casella A,<br />
Cargnel A. Impact <strong>of</strong> highly active antiretroviral therapy on<br />
clinical evolution <strong>of</strong> genital warts in HIV-1-infected patients.<br />
AIDS 1999;13:291-3.<br />
171. Reichert CM, O’Leary TJ, Levens DL, Simrell CR, Madner AM.<br />
Autopsy pathology in the acquired immunodeficiency syndrome.<br />
Am J Pathol 1983;112:357-82.<br />
172. Matis WL, Triana A, Shapiro R, Eldred L, Polk BF, Hood HF.<br />
Dermatologic findings associated with human immunodeficiency<br />
virus infection. J Am Acad Dermatol 1987;17:746-51.<br />
173. Hira SK, Wadhawan D, Kamanga J, Kavindele D, Macuacua R,<br />
Patil PS, et al. Cutaneous manifestations <strong>of</strong> human immunodeficiency<br />
virus in Lusaka, Zambia. J Am Acad Dermatol<br />
1988;19:451-7.<br />
174. Coldiron BM, Bergstresser PR. Prevalence and clinical spectrum<br />
<strong>of</strong> skin disease in patients infected with human immunodeficiency<br />
virus. Arch Dermatol 1989;125:357-61.<br />
175. Koopman RJJ, Van Merrienboer FCJ, Vreden SGS, Dolmans<br />
WMV. Molluscum contagiosum: a marker for advanced HIV<br />
infection. Br J Dermatol 1992;126:528-9.<br />
176. Husak R, Garbe C, Orfanos CE. Mollusca contagiosa in HIV<br />
Czelusta, Yen-Moore, and Tyring 429<br />
infection: clinical manifestations in relation to immune status<br />
and prognostic value in 39 patients. Hautarzt 1997;48:103-9.<br />
177. Dann FJ, Tabibian P. Cutaneous <strong>diseases</strong> in human immunodeficiency<br />
virus-infected patients referred to the UCLA<br />
Immunosuppression Skin Clinic: reasons for referral and management<br />
<strong>of</strong> selected <strong>diseases</strong>. Cutis 1995;55:85-8.<br />
178. Schaub N, Gilli L, Rufli T, Gyr N, Battegay M, Nuesch R, et al.<br />
Epidemiology <strong>of</strong> skin <strong>diseases</strong> in HIV-infected patients: a<br />
prospective cohort study. Schweiz Rundsch Med Prax 1996;85:<br />
1162-6.<br />
179. Reynaud-Mendel B, Janier M, Gerbaka J, Hakim C, Rabian C,<br />
Chastang C, et al. Dermatologic findings in HIV-1 infected<br />
patients: a prospective study with emphasis on CD4+ cell<br />
count. <strong>Dermatology</strong> 1996;192:325-8.<br />
180. Mahe A, Bobin P, Coulibaly S, Tounkara A. Skin <strong>diseases</strong> disclosing<br />
human immunodeficiency virus infection in Mali. <strong>An</strong>n<br />
Dermatol Venereol 1997;124:144-50.<br />
181. Munoz-Perez MA, Rodriguez-Pichardo A, Camacho F,<br />
Colmenero MA. Dermatological findings correlated with CD4<br />
lymphocyte counts in a prospective 3 year study <strong>of</strong> 1161<br />
patients with human immunodeficiency virus disease predominantly<br />
acquired though intravenous drug abuse. Br J<br />
Dermatol 1998;139:33-9.<br />
182. Jung AC, Paauw DS. Diagnosing HIV-related disease: using the<br />
CD4 count as a guide. J Gen Intern Med 1998;13:131-6.<br />
183. Konya J, Thompson CH. Molluscum contagiosum virus: antibody<br />
responses in persons with clinical lesions and seroepidemiology<br />
in a representative Australian population. J Infect<br />
Dis 1999;179:701-4.<br />
184. Ficarra G, Cortes S, Rubino I, Romagnoli P. Facial and perioral<br />
molluscum contagiosum in patients with HIV infection: a<br />
report <strong>of</strong> eight cases. Oral Surg Oral Med Oral Pathol<br />
1994;78:621-6.<br />
185. Darai G, Reisner H, Scholz J, Schnitzler P, Lorbacher de Ruiz H.<br />
<strong>An</strong>alysis <strong>of</strong> the genome <strong>of</strong> the molluscum contagiosum virus<br />
by restriction endonuclease analysis and molecular cloning. J<br />
Med Virol 1986;18:29-39.<br />
186. Yamashita H, Uemura T, Kwashima M. Molecular epidemiologic<br />
analysis <strong>of</strong> Japanese patients with molluscum contagiosum.<br />
Int J Dermatol 1996;35:99-105.<br />
187. Thompson CH, de Zwart-Steffe RT, Donovan B. Clinical and<br />
molecular aspects <strong>of</strong> molluscum contagiosum infection in<br />
HIV-1 positive patients. Int J STD AIDS 1992;3:101-6.<br />
188. Schwartz JJ, Myskowski PL. Molluscum contagiosum in<br />
patients with human immunodeficiency virus infection: a<br />
review <strong>of</strong> twenty-seven patients. J Am Acad Dermatol 1992;<br />
27:583-8.<br />
189. Biswas J, Therese L, Kumarasamy N, Solomon S, Yesudian P. Lid<br />
abscess with extensive molluscum contagiosum in a patient<br />
with acquired immunodeficiency syndrome. Indian J<br />
Opthalmol 1997;45:234-6.<br />
190. Leahey AB, Shane JJ, Listhaus A,Trachtman M. Molluscum contagiosum<br />
eyelid lesions as the initial manifestation <strong>of</strong><br />
acquired immunodeficiency syndrome. Am J Ophthalmol<br />
1997;124:240-1.<br />
191. Betlloch I, Pinazo I, Mestre F, Altes J, Villalonga C. Molluscum<br />
contagiosum in human immunodeficiency virus infection:<br />
response to zidovudine. Int J Dermatol 1989;28:351-2.<br />
192. Redfield RR, James WD, Wright DC, Brown C, Salahuddin SZ,<br />
Markham PO, et al. Severe molluscum contagiosum infection<br />
in a patient with human T-cell lymphotrophic (HTLV-<strong>III</strong>) disease.<br />
J Am Acad Dermatol 1985;13:821-4.<br />
193. Gottlieb SL, Myskowski PL. Molluscum contagiosum. Int J<br />
Dermatol 1994;33:453-61.<br />
194. Williams LR, Webster G. Warts and molluscum contagiosum.<br />
Clin Dermatol 1991;9:87-93.
430 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
195. Delescluse J, Goens J. Multiple mollusca contagiosa revealing<br />
HTLV-<strong>III</strong> infection. Dermatologica 1986;172:283-5.<br />
196. Brandrup F, Asschenfeldt P. Molluscum contagiosum-induced<br />
comedo and secondary abscess formation. Pediatr Dermatol<br />
1989;6:118-21.<br />
197. Felman YM. Molluscum contagiosum. Cutis 1984;33:113-7.<br />
198. Fivenson DP, Weltman RE, Gibson SH. Giant molluscum contagiosum<br />
presenting as a basal cell carcinoma in an acquired<br />
immunodeficiency syndrome patient. J Am Acad Dermatol<br />
1988;19:912-4.<br />
199. Cockerell CJ. Cutaneous manifestations <strong>of</strong> HIV infection other<br />
than Kaposi’s sarcoma: clinical and histologic aspects. J Am<br />
Acad Dermatol 1990;22:1260-9.<br />
200. Itin PH, Gilli L. Molluscum contagiosum mimicking sebaceous<br />
nevus <strong>of</strong> Jadassohn, ecthyma, and giant condylomata acuminata<br />
in HIV-infected patients. <strong>Dermatology</strong> 1994;189:396-8.<br />
201. Schwartz JJ, Myskowski PL. HIV-related molluscum contagiosum<br />
presenting as a cutaneous horn. Int J Dermatol 1992;31:<br />
142-4.<br />
202. Rico MJ, Penneys NS. Cutaneous cryptococcosis resembling<br />
molluscum contagiosum in a patient with AIDS. Arch<br />
Dermatol 1985;121:901-2.<br />
203. Concus AP, Helfand RF, Imber MJ, Lerner EA, Sharpe RJ.<br />
Cutaneous cryptococcosis mimicking molluscum contagiosum<br />
in a patient with AIDS. J Infect Dis 1988;158:897-8.<br />
204. Feuilhade de Chavin M, Revuz J, Deniau M. Histoplasmose a<br />
histoplasma duboisii: lesions cutanees simulant des molluscum<br />
contagiosum. <strong>An</strong>n Dermatol Venereol 1983;113:715-6.<br />
205. Cavicchini S, Brezzi A, Alessi E. Ultrastructural findings in<br />
mucocutaneous infections <strong>of</strong> patients seropositive to HIV. Am<br />
J Dermatopathol 1993;15:320-5.<br />
206. Smith KJ, Skelton HG, Yeager J, James WD, Wagner KF.<br />
Molluscum contagiosum: ultrastructural evidence for its presence<br />
in skin adjacent to clinical lesions in patients infected<br />
with human immunodeficiency virus type I. Arch Dermatol<br />
1992;128:223-7.<br />
207. Birthistle K, Carrington D. Molluscum contagiosum virus. J<br />
Infect 1997;34:21-8.<br />
208. Cronin TA, Resnik BI, Elgart G, Kerdel FA. Recalcitrant giant molluscum<br />
contagiosum in a patient with AIDS. J Am Acad<br />
Dermatol 1996;35:266-7.<br />
209. de Waard-van der Spek FB, Oranje AP, Lillieborg S, Hop WCJ,<br />
Stolz E. Treatment <strong>of</strong> molluscum contagiosum using a lidocaine/prilocaine<br />
cream (EMLA) for analgesia. J Am Acad<br />
Dermatol 1990;23:685-8.<br />
210. Garrett SJ, Robinson JK, Roenogk HH. Trichloroacetic acid peel<br />
<strong>of</strong> molluscum contagiosum in immunocompromised<br />
patients. J Dermatol Surg Oncol 1992;18:855-8.<br />
211. Nelson MR, Chard S, Barton SE. Intralesional interferon for the<br />
treatment <strong>of</strong> recalcitrant molluscum contagiosum in HIV-antibody<br />
positive individuals, a preliminary report. Int J STD AIDS<br />
1995;6:351-2.<br />
212. Mayumi H,Yamaoka K,Tsutsui T, Mizue H, Doi A, Matsayuma M,<br />
et al. Selective immunoglobulin M deficiency associated with<br />
disseminated molluscum contagiosum. Eur J Pediatr 1986;<br />
145:99-103.<br />
213. Smith K, Liota E, Yeager J, Menon P. Treatment <strong>of</strong> molluscum<br />
contagiosum virus with topical imiquimod. Presented as a<br />
poster (#352) at the 57th <strong>An</strong>nual Meeting <strong>of</strong> the American<br />
Academy <strong>of</strong> <strong>Dermatology</strong>, New Orleans, Louisian, March 19-<br />
24, 1999.<br />
214. Zabawski EJ, Cockerell CJ.Topical and intralesional cid<strong>of</strong>ovir: a<br />
review <strong>of</strong> pharmacology and therapeutic effects. J Am Acad<br />
Dermatol 1998;39:741-5.<br />
215. Meadows KP, Tyring SK, Pavia AT, Rallis TM. Resolution <strong>of</strong> recalcitrant<br />
molluscum contagiosum lesions in HIV-infected<br />
patients treated with cid<strong>of</strong>ovir. Arch Dermatol 1997;133:987-<br />
90.<br />
216. Hicks CB, Myers SA, Giner J. Resolution <strong>of</strong> intractable molluscum<br />
contagiosum in a human immunodeficiency virus-infected<br />
patient after institution <strong>of</strong> antiretroviral therapy with ritonavir.<br />
Clin Infect Dis 1997;24:1023-5.<br />
217. Horn CK, Scott GR, Benton EC. Resolution <strong>of</strong> severe molluscum<br />
contagiosum on effective antiretroviral therapy. Br J Dermatol<br />
1998;138:715-7.<br />
218. Olansky S, Clair A. How we treat molluscum contagiosum.<br />
Postgrad Med 1970;47:259-60.<br />
219. Bolier IC, Myskowski PL, Torre DP. Disposable attachments in<br />
cryosurgery: a useful adjunct in the treatment <strong>of</strong> HIV-associated<br />
neoplasms. J Dermatol Surg Oncol 1991;17:277-8.<br />
220. Hughes PS. Treatment <strong>of</strong> molluscum contagiosum with the<br />
585-nm pulsed tuneable dye laser. Dermatol Surg 1998;24:<br />
229-30.<br />
221. Chang Y, Cesarman E, Pessin MS, Lee F, Culpepper J, Knowles<br />
DM, et al. Identification <strong>of</strong> herpesvirus-like DNA sequences in<br />
AIDS-associated Kaposi’s sarcoma. Science 1994;266:1865-9.<br />
222. Lebbe C, de Cremoux P, Rybojad M, Costa da Cunha C, Morel P,<br />
Calvo F. Kaposi’s sarcoma and a new herpesvirus. Lancet 1995;<br />
345:1180.<br />
223. Moore PS, Chang Y. Detection <strong>of</strong> herpesvirus-like DNA<br />
sequences in Kaposi’s sarcoma lesions from persons with and<br />
without HIV infection. N Engl J Med 1995;332:1181-5.<br />
224. Bosh<strong>of</strong>f C, Whitby D, Hatziioannou T, Fisher C, van der Walt J,<br />
Hatzakisk A, et al. Kaposi’s sarcoma-associated herpesvirus in<br />
HIV-negative Kaposi’s sarcoma. Lancet 1995;345:1043-4.<br />
225. Chang Y, Zeigler J, Wabinga H, Katangole-Mbidde E, Bosh<strong>of</strong>f C,<br />
Schulz TK, et al. Kaposi’s sarcoma-associated herpesvirus and<br />
Kaposi’s sarcoma in Africa. Arch Intern Med 1996;156:202-4.<br />
226. Rady PL, Yen A, Martin RW, Nedelcu I, Hughes TK, Tyring SK.<br />
Herpesvirus-like DNA sequences in classic Kaposi’s sarcoma. J<br />
Med Virol 1995;47:179-83.<br />
227. Strauchen JA, Hauser AD, Burstein DA, Jiminez R, Moore PS,<br />
Chang Y. Kaposi’s sarcoma, Kaposi’s sarcoma-associated herpesvirus,<br />
and body cavity-based malignant lymphoma in an<br />
HIV-negative man. <strong>An</strong>n Intern Med 1997;125:822-5.<br />
228. <strong>An</strong>sari MQ, Dawson DB, Nador R, Rutherford C, Schneider NR,<br />
Latimer MJ, et al. Primary body cavity-based AIDS related lymphomas.<br />
Am J Clin Pathol 1996;105:221-9.<br />
229. Corbellino M, Poirel L, Aubin JT, Paulli M, Magrini U, Bestetti G,<br />
et al.The role <strong>of</strong> human herpesvirus 8 and Epstein-Barr virus in<br />
the pathogenesis <strong>of</strong> giant lymph node hyperplasia<br />
(Castleman’s disease). Clin Infect Dis 1996;22:1120-1.<br />
230. Soulier J, Grollet L, Oksenhandler E, Cacoub P, Cazals-Hatem D,<br />
Babinet P, et al. Kaposi’s sarcoma-associated herpesvirus-like<br />
DNA sequences in multicentric Castleman’s disease. Blood<br />
1995;86:1275-80.<br />
231. Biggar RJ, Curtis RE, Cote TR, Rubkin CS, Melbye M. Risk <strong>of</strong> other<br />
cancers following Kaposi’s sarcoma: relation to acquired<br />
immunodeficiency syndrome. Am J Epidemiol 1994;139:362-8.<br />
232. Piette WW.The incidence <strong>of</strong> second malignancies in subsets <strong>of</strong><br />
Kaposi’s sarcoma. J Am Acad Dermatol 1987;16:855-61.<br />
233. Reynolds P, Saunders LD, Layefsky ME, Lemp GF. The spectrum<br />
<strong>of</strong> acquired immunodeficiency (AIDS)-associated malignancies<br />
in San Francisco, 1980-1987. Am J Epidemiol 1993;137:19-<br />
30.<br />
234. Owor R. Multiple primary malignant tumors in Ugandan<br />
Africans. East Afr Med J 1980;57:692-5.<br />
235. Schwartz RA. Kaposi’s sarcoma: advances and perspectives. J<br />
Am Acad Dermatol 1996;34:804-14.<br />
236. Beral V, Peterman TA, Berkelman RL, Jaffe HW. Kaposi’s sarcoma<br />
among persons with AIDS: a <strong>sexually</strong> <strong>transmitted</strong> infection?<br />
Lancet 1990;335:123-8.
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
237. Archibald CP, Schechter MT, Le TN, Craib KJ, Montaner JS,<br />
O’Shaughnessy MV. Evidence for a <strong>sexually</strong> <strong>transmitted</strong> c<strong>of</strong>actor<br />
for AIDS-related Kaposi’s sarcoma in a cohort <strong>of</strong> homosexual<br />
men. Epidemiology 1992;3:203-9.<br />
238. Jaffe HW, Choi K, Thomas PA, Haverkos HW, Auerbach DM,<br />
Guinan ME, et al. National case-control study <strong>of</strong> Kaposi’s sarcoma<br />
and pneumocystis carinii pneumonia in homosexual<br />
men: <strong>Part</strong> I. epidemiologic results. <strong>An</strong>n Intern Med 1983;99:<br />
145-51.<br />
239. Darrow WW, Jaffe HW, Curran JW. Passive anal intercourse as a<br />
risk factor for AIDS in homosexual men. Lancet 1983;2:160.<br />
240. Lifson AR, Darrow WW, Hessol NA, O’Malley PM, Barnhart JL,<br />
Jaffe HW, et al. Kaposi’s sarcoma in a cohort <strong>of</strong> homosexual<br />
and bisexual men. Am J Epidemiol 1990;131:221-31.<br />
241. Jacobson LP, Munos A, Fox R. Incidence <strong>of</strong> Kaposi’s sarcoma in<br />
a cohort <strong>of</strong> homosexual men with human immunodeficiency<br />
virus type 1. J Acquir Immune Defic Syndr 1990;3(Suppl 1):S24.<br />
242. Rutherford GW, Payne SF, Lemp GF.The epidemiology <strong>of</strong> AIDSrelated<br />
Kaposi’s sarcoma in San Francisco. J Acquir Immune<br />
Defic Syndr 1990;3(Suppl 1):S4-S7.<br />
243. Goedert JJ, Biggar RJ, Melbye M, Mann DL,Wilson S, Gail MH, et<br />
al. Effect <strong>of</strong> T4 count and c<strong>of</strong>actors on the incidence <strong>of</strong> AIDS in<br />
homosexual men infected with human immunodeficiency<br />
virus. JAMA 1987;257:331-4.<br />
244. Martin JN, Ganem DE, Osmond DH, Page-Shafer KA, Macrae D,<br />
Kedes DH. Sexual transmission and the natural history <strong>of</strong><br />
human herpesvirus 8 infection. N Engl J Med 1998;280:31-2.<br />
245. Ambroziak JA, Blackbourn DJ, Herndier BG, Glogau RG, Gullett<br />
JH, MacDonald AR. Herpes-like sequences in HIV-infected and<br />
uninfected Kaposi’s sarcoma patients. Science 1995;268:582-3.<br />
246. Gupta P, Singh MK, Rinaldo C, Ding M, Farzadegan H, Saah A, et<br />
al. Detection <strong>of</strong> Kaposi’s sarcoma herpesvirus DNA in semen <strong>of</strong><br />
homosexual men with Kaposi’s sarcoma. AIDS 1996;10:1596-8.<br />
247. Howard MR, Whitby D, Bahadur G, Sugget F, Bosch<strong>of</strong>f C,<br />
Tenant-Flowers CM, et al. Detection <strong>of</strong> Kaposi’s sarcoma-associated<br />
herpesvirus (KSHV) DNA in semen from HIV-infected<br />
individuals but not from healthy semen donors. J AIDS<br />
1997;11:F15-F19.<br />
248. Corbellino M, Bestetti G, Galli M, Parravicini C. Absence <strong>of</strong> HHV-<br />
8 in prostate and semen. N Engl J Med 1996;335:1237.<br />
249. Tasaka T, Said JW, Koeffler HP. Absence <strong>of</strong> HHV-8 in prostate<br />
and semen. N Engl J Med 1996;335:1237-8.<br />
250. Monini P, de Lellis L, Fabris M, Rigonlin F, Cassai E. Kaposi’s sarcoma-associated<br />
herpesvirus DNA sequences in prostate tissue<br />
and human semen. N Engl J Med 1996;334:1168-72.<br />
251. Lin JC, Lin SC, Mar EC, Pellett PE, Stamey FR, Stewart JA, et al. Is<br />
Kaposi’s sarcoma-associated herpesvirus detectable in semen<br />
<strong>of</strong> HIV-infected homosexual men? Lancet 1995;346:1601-2.<br />
252. Whitby D, Howard MR, Tennant-Flowers M, Brink NS, Copas A,<br />
Bosh<strong>of</strong>f KC, et al. Detection <strong>of</strong> Kaposi’s sarcoma-associated<br />
herpesvirus in peripheral blood predicts progression to<br />
Kaposi’s sarcoma. Lancet 1995;346:799-802.<br />
253. Boldough I, Szaniszlo P, Bresnahan WA, Flaitz CM, Nichols MC,<br />
Albrecht T, et al. Kaposi’s sarcoma herpesvirus-like DNA<br />
sequences in the saliva <strong>of</strong> individuals infected with human<br />
immunodeficiency virus. Clin Infect Dis 1996;23:406-7.<br />
254. Beral V, Bull D, Darby S, Weller I, Carne C, Beecham M, et al. Risk<br />
<strong>of</strong> Kaposi’s sarcoma and sexual practices associated with fecal<br />
contact in homosexuals or bisexual men with AIDS. Lancet<br />
1992;339:632-5.<br />
255. Papadopoulos-Eleopoulos E, Turner VF, Papadimitriou JM.<br />
Kaposi’s sarcoma and HIV. Med Hypotheses 1992;39:22-9.<br />
256. Schechter MT, Marion SA, Elmslie KD, Ricketts MN, Mault P,<br />
Archibald CP. Geographic and birth cohort associations <strong>of</strong><br />
Kaposi’s sarcoma among homosexual men in Canada. Am J<br />
Epidemiol 1991;134:485-8.<br />
Czelusta, Yen-Moore, and Tyring 431<br />
257. Lacour JP, Bodokh I, Castanet J, Beckri S, Ortonne JP. Porphyria<br />
cutanea tarda and antibodies to hepatitis C virus. Br J<br />
Dermatol 1993;128:121-3.<br />
258. Koester G, Feldman J, Bigler C. Hepatitis C in patients with porphyria<br />
cutanea tarda. J Am Acad Dermatol 1994;31:1054.<br />
259. Rich JD, Mylonakis E, Nossa R, Chapnick RM. Highly active antiretroviral<br />
therapy leading to resolution <strong>of</strong> porphyria cutanea<br />
tarda in a patient with AIDS and hepatitis C. Dig Dis Sci 1999;<br />
44:1034-7.<br />
260. Drobacheff C, Derancourt C, Van Landuyt H, Devred D, de<br />
Wazieres B, Cribier B, et al. Porphyria cutanea tarda associated<br />
with human immunodeficiency virus infection. Eur J Dermatol<br />
1998;8:492-6.<br />
261. O’Connor WJ, Badley AD, Dicken CH, Murphy GM. Porphyria<br />
cutanea tarda and human immunodeficiency virus: two cases<br />
associated with hepatitis C. Mayo Clin Proc 1998;73:895-7.<br />
262. McAlister F, McClean K, Hamilton PG, Houston S. Human<br />
immunodeficiency virus infection and porphyria cutanea<br />
tarda: coexistence <strong>of</strong> risk factors or causative association? Clin<br />
Infect Dis 1995;20:348-51.<br />
263. Lim HW, Pereira A, Sassa S, Kim M, Zolla-Pazner S. Early-stage HIV<br />
infection and hepatitis C infection are associated with elevated<br />
serum porphyrin levels. J Am Acad Dermatol 1998;39:956-9.<br />
264. O’Connor WJ, Murphy GM, Darby C, Fogarty J, Mulcahy F,<br />
O’Moore R, et al. Porphyrin abnormalities in acquired immunodeficiency<br />
syndrome. Arch Dermatol 1996;132:1443-7.<br />
265. Nomura N, Zolla-Pazner S, Simberk<strong>of</strong>f M, Kim M, Sassa S, Lim<br />
HW. Abnormal serum porphyrin levels in patients with the<br />
acquired immunodeficiency syndrome with or without<br />
hepatitis C virus infection. Arch Dermatol 1996;132:906-10.<br />
266. Sadick N, Kaplan MH, Pahwa SG, Sarngadharan MG. Unusual<br />
features <strong>of</strong> scabies complicating human T-lymphotrophic<br />
virus type <strong>III</strong> infection. J Am Acad Dermatol 1986;15:482-6.<br />
267. Rau RC, Baird IM. Crusted scabies in a patient with acquired<br />
immunodeficiency syndrome. J Am Acad Dermatol 1986;15:<br />
1058-9.<br />
268. Glover R, Young L, Goltz RW. Norwegian scabies in acquired<br />
immunodeficiency syndrome: report <strong>of</strong> a case resulting in<br />
death from associated sepsis. J Am Acad Dermatol 1987;16:<br />
396-9.<br />
269. Drabick JJ, Lupton GP, Tompkins K. Crusted scabies in human<br />
immunodeficiency virus infection. J Am Acad Dermatol 1987;<br />
17:142.<br />
270. Dillon SM. <strong>An</strong> HIV-infected patient with an extraordinary rash.<br />
Hosp Pract 1989;24:199-200.<br />
271. Hall JC, Brewer JH, Appl BA. Norwegian scabies in a patient<br />
with acquired immune deficiency syndrome. Cutis 1989;43:<br />
325-9.<br />
272. Jucowics P, Ramon ME, Don PC, Stone RK, Barnji M. Norwegian<br />
scabies in an infant with acquired immunodeficiency syndrome.<br />
Arch Dermatol 1989;125:1670-6.<br />
273. Lim W, Sadick N, Gupta A, Kaplan M, Pawha S. Skin <strong>diseases</strong> in<br />
children with HIV infection and their association with degree<br />
<strong>of</strong> immunosuppression. Int J Dermatol 1990;29:24-30.<br />
274. Sirera J, Ruis F, Romeu J, Llibre J, Ribera M, Soriano V, et al.<br />
Hospital outbreak <strong>of</strong> scabies stemming from two AIDS<br />
patients with Norwegian scabies. Lancet 1990;335:1227.<br />
275. Rostami G, Sorg TB. Nosocomial outbreak <strong>of</strong> scabies associated<br />
with Norwegian scabies in an AIDS patient. Int J STD AIDS<br />
1990;1:209-10.<br />
276. Jessurun J, Romo-Garcia J, Lopez-Denis O, Olvera-Rabiela JE.<br />
Crusted scabies in a patient with the acquired immunodeficiency<br />
syndrome. Virchows Archiv A Pathol <strong>An</strong>at 1990;416:<br />
461-3.<br />
277. Squires J. Scabies: an unusual presentation in a patient with<br />
AIDS. Clin Cases Dermatol 1990;2:5-9.
432 Czelusta, Yen-Moore, and Tyring J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
278. Inserra DW, Bickley LK. Crusted scabies in acquired immunodeficiency<br />
syndrome. Int J Dermatol 1990;29:287-9.<br />
279. Moss VA, Salisbury J. Scabies in an AIDS hospice unit. Br J Clin<br />
Pract 1991;45:35-6.<br />
280. Waldman BA. Crusted (Norwegian) scabies in an HIV-infected<br />
man. Clin Cases Dermatol 1991;3:6-9.<br />
281. Wlotzke U, Thiele B, Wolff HH, Meigel W. Norwegian scabies in<br />
a patient with AIDS. Hautarzt 1992;43:717-20.<br />
282. Donabedian H, Khazan U. Norwegian scabies in a patient with<br />
AIDS. Clin Infect Dis 1992;14:162-4.<br />
283. Hulbert TV, Larsen RA. Hyperkeratotic (Norwegian) scabies<br />
with gram-negative bacteremia as the initial presentation <strong>of</strong><br />
AIDS. Clin Infect Dis 1992;14:1164-5.<br />
284. Skinner SM, DeVillez RL. Sepsis associated with Norwegian<br />
scabies in a patient with acquired immunodeficiency syndrome.<br />
Cutis 1992;50:213-6.<br />
285. Funkhouser ME, Omohundro C, Ross A, Berger TG.<br />
Management <strong>of</strong> scabies in patients with human immunodeficiency<br />
virus disease. Arch Dermatol 1993;129:911-3.<br />
286. Mollison LC, Lo STH, Marning G. HTLV-1 and scabies in<br />
Australian Aborigines. Lancet 1993;341:1281-2.<br />
287. Spach DH, Fritsche TR. Images in clinical medicine: Norwegian<br />
scabies in a patient with AIDS. N Engl J Med 1994;331:777.<br />
288. Schlesinger I, Oelrich DM, Tyring SK. Crusted (Norwegian) scabies<br />
in patients with AIDS: the range <strong>of</strong> clinical presentations.<br />
South Med J 1994;87:352-6.<br />
289. Suarez Fernandez R, Rodriguez FM, Lopez Bran E, Nunez<br />
Alonso C, Sanchez De Paz F, Sanchez Yus E. Norwegian scabies<br />
in a patient with AIDS: report <strong>of</strong> a case. Cutis 1995;56:57-60.<br />
290. Solomon HA, Haut SR, Carr EM, Shalita AR. Neurotoxic reaction<br />
to lindane in an HIV-seropositive patient: an old medication’s<br />
new problem. J Fam Pract 1995;40:291-6.<br />
291. Corbett EL, Crossley I, Holton J, Levell N, Miller RF, De Cock KM.<br />
Crusted (Norwegian) scabies in a specialist HIV unit: successful<br />
use <strong>of</strong> ivermectin and failure to prevent nosocomial transmission.<br />
Genitourin Med 1996;72:115-7.<br />
292. Nandwani R, Pozniak AL, Fuller LC, Wade J. Crusted<br />
(Norwegian) scabies in a specialist HIV unit. Genitourin Med<br />
1996;72:453.<br />
293. DelGuidice P, Carles M, Couppie P, Bernard E, Lacour JP, Marty P,<br />
et al. Successful treatment <strong>of</strong> crusted (Norwegian) scabies<br />
with ivermectin in two patients with human immunodeficiency<br />
virus infection. Br J Dermatol 1996;135:494-5.<br />
294. Valks R, Buezo GF, Dauden E. Scabies and leukocytoclastic vasculitis<br />
in an HIV-seropositive man. Int J Dermatol 1996;35:605-6.<br />
295. Portu JJ, Santamaria JM, Zubero Z, Almeida-Llamas MV,<br />
Aldamiz-Etxebarria San Sebastian M, Gutierrez R. Atypical scabies<br />
in HIV-positive patients. J Am Acad Dermatol 1996;<br />
34:915-7.<br />
296. Farrell AM, Ross JS, Bunker CB, Staughton RCD. Crusted scabies<br />
with scalp involvement in HIV-1 infection. Br J Dermatol 1998;<br />
138:192-3.<br />
297. Bitman LM, Rabinowitz AD. Hyperkeratotic plantar plaques in<br />
an HIV-positive patient. Arch Dermatol 1998;134:1019,1022-3.<br />
298. Guggisberg D, de Viragh PA, Constantin C, Panizzon RG.<br />
Norwegian scabies in a patient with acquired immunodeficiency<br />
syndrome. <strong>Dermatology</strong> 1998;197:306-8.<br />
299. Orkin M. Scabies in AIDS. Semin Dermatol 1993;12:9-14.<br />
300. Taplin D, Meinking TL. Treatment <strong>of</strong> HIV-related scabies with<br />
emphasis on the efficacy <strong>of</strong> ivermectin. Semin Cutan Med<br />
Surg 1997;16:235-40.<br />
301. Mellanby K. Scabies in 1976. R Soc Health J 1977;97:32-6.<br />
302. Currie BJ, Maguire GP, Wood YK. Ivermectin and crusted<br />
(Norwegian) scabies. Med J Aust 1995;163:559-60.<br />
303. Glaziou P, Cartel JL, Alzieu P, Briot C, Moulia-Pelat JP, Martin PM.<br />
Comparison <strong>of</strong> ivermectin and benzyl benzoate for treatment<br />
<strong>of</strong> scabies. Trop Med Parasitol 1993;44:331-2.<br />
304. Marty P, Gari-Toussaint M, Le-Fichoux Y, Gaxotte P. Efficacy <strong>of</strong><br />
ivermectin in the treatment <strong>of</strong> an epidemic <strong>of</strong> sarcoptic scabies.<br />
<strong>An</strong>n Trop Med Parasitol 1994;88:453.<br />
305. Meinking TL, Taplin D, Hermida J, Pardo R, Kerdel FA. The treatment<br />
<strong>of</strong> scabies with ivermectin. N Engl J Med 1995;333:26-30.
Directions for questions 1-16: Give single best response.<br />
1. A patient with AIDS comes to your clinic with her first<br />
case <strong>of</strong> genital herpes. A good estimate <strong>of</strong> the likelihood<br />
that her infection will be resistant to acyclovir is<br />
a. less than 1%<br />
b. 3%<br />
c. 6%<br />
d. 12%<br />
e. 24%<br />
2. A patient comes to your clinic with AIDS and a history<br />
<strong>of</strong> anal warts. Each <strong>of</strong> the following is true except<br />
a. patients with AIDS generally have more human<br />
papillomavirus (HPV) subtypes present in their<br />
infections.<br />
b. as his CD4 cell counts drop, this patient will shed<br />
more HPV virions.<br />
c. concurrent HIV and anal HPV infections increase<br />
this patient’s risk for anorectal carcinoma.<br />
d. optimizing his antiretroviral medications may<br />
make management <strong>of</strong> any anal wart recurrences<br />
more feasible.<br />
d. acetic acid is not a useful diagnostic tool for recognizing<br />
anal squamous intraepithelial lesions in this<br />
patient.<br />
3. Kaposi’s sarcoma (KS)<br />
a. is not associated with human herpesvirus type 8 in<br />
HIV-infected patients<br />
b. is associated with an increased risk for non-<br />
Hodgkin’s lymphoma in HIV-infected patients<br />
c. occurs most commonly among people who<br />
acquired HIV through intravenous drug abuse<br />
d. occurs at similar rates for HIV-infected patients in<br />
all US cities<br />
e. does not follow the epidemiologic patterns <strong>of</strong> an<br />
infectious disease<br />
4. The best approximation for the number <strong>of</strong> scabies<br />
mites on an HIV-infected patient with crusted scabies<br />
is<br />
a. fewer than 5<br />
b. 5-10<br />
c. 10-20<br />
d. 20-50<br />
e. more than 50<br />
5. In the treatment <strong>of</strong> AIDS patients with crusted scabies,<br />
which <strong>of</strong> the following medications has been<br />
CME examination<br />
Identification No. 800-109<br />
Instructions for Category I CME credit appear in the front advertising section. See last page <strong>of</strong> Contents for page number.<br />
Questions 1-31, Czelusta A, Yen-Moore A, Tyring SK. J Am Acad Dermatol 2000;43:409-32.<br />
documented as a potential cause <strong>of</strong> severe neurologic<br />
side effects in case reports?<br />
a. Lindane<br />
b. Permethrin<br />
c. Mebendazole<br />
d. Metronidazole<br />
e. Ivermectin<br />
6. The most likely mechanisms by which herpes simplex<br />
virus (HSV) mediates resistance to thymidine kinase<br />
inhibitors includes each <strong>of</strong> the following except<br />
a. production <strong>of</strong> viral thymidine kinase with decreased<br />
substrate affinity<br />
b. production <strong>of</strong> viral DNA polymerase with decreased<br />
substrate affinity<br />
c. decreased production <strong>of</strong> viral thymidine kinase<br />
d. absence <strong>of</strong> viral thymidine kinase production<br />
e. altered transport <strong>of</strong> thymidine kinase inhibitors<br />
into infected cells<br />
7. <strong>An</strong> HIV-infected patient who is allergic to penicillin<br />
comes to your clinic with early latent syphilis. Which<br />
<strong>of</strong> the following antibiotics is the most appropriate<br />
therapy?<br />
a. Intramuscular benzathine penicillin G<br />
b. Oral cipr<strong>of</strong>loxacin<br />
c. Oral erythromycin<br />
d. Intravenous vancomycin<br />
e. Intramuscular ceftriaxone<br />
8. Chancroid in HIV-positive patients<br />
a. is commonly atypical in its clinical presentation<br />
b. presents with larger ulcers than those seen in HIVnegative<br />
patients<br />
c. has distinct histologic differences from HIV-negative<br />
patients on microscopic examination<br />
d. increases the risk <strong>of</strong> HIV transmission to sexual<br />
partners<br />
e. cannot be cured by the same antibiotic regimens<br />
that are recommended for immunocompetent<br />
patients<br />
9. A patient with advanced AIDS presents with a facial<br />
molluscum contagiosum. Which <strong>of</strong> the following<br />
should he be told about the lesion?<br />
a. Shaving his face will help improve skin cleanliness<br />
and decrease the likelihood <strong>of</strong> new lesions developing.<br />
b. Optimization <strong>of</strong> his antiretroviral medications will<br />
not help in the care <strong>of</strong> this lesion.<br />
433
434 CME examination J AM ACAD DERMATOL<br />
SEPTEMBER 2000<br />
c. Crude podophyllin resin is the safest therapeutic<br />
modality for the removal <strong>of</strong> this lesion.<br />
d. This infection is unlikely to resolve spontaneously.<br />
e. Carbon dioxide laser therapy is the most efficacious<br />
modality for treating this lesion.<br />
10. Each <strong>of</strong> the following statements regarding syphilis in<br />
the HIV-infected host is true except<br />
a. Clinical presentation is usually the same in HIVinfected<br />
persons as it is in HIV-negative hosts.<br />
b. Several studies document increased rates <strong>of</strong> falsepositive<br />
fluorescent treponemal antibody absorption<br />
assays.<br />
c. A patient’s progression through the various stages<br />
<strong>of</strong> syphilis may be faster if he is HIV infected.<br />
d. HIV-infected patients may progress to neurosyphilis<br />
despite treatment with recommended<br />
antibiotic regimens.<br />
e. Histologic examination <strong>of</strong> tissue specimens may be<br />
helpful in cases in which the results <strong>of</strong> HIV-infected<br />
patients’ serologic tests are not consistent with<br />
their dermatologists’ clinical suspicions.<br />
11. Which <strong>of</strong> the following statements is false?<br />
a. Patients with genital herpes are at increased risk <strong>of</strong><br />
acquiring HIV from their HIV-positive partners.<br />
b. <strong>An</strong>tiviral control <strong>of</strong> HSV has no impact on a<br />
patient’s response to antiretroviral drugs.<br />
c. Treatment <strong>of</strong> genital herpes in HIV-positive persons<br />
may require increased doses <strong>of</strong> acyclovir or<br />
famciclovir.<br />
d. A person with both HSV and HIV infections has an<br />
increased risk <strong>of</strong> transmitting HIV relative to an<br />
HSV-negative person with HIV.<br />
e. Taking famciclovir daily reduces both symptomatic<br />
and asymptomatic HSV viral shedding in HIV-positive<br />
persons.<br />
12. Which <strong>of</strong> the following is the most common cause <strong>of</strong><br />
genital ulcer disease worldwide?<br />
a. HIV<br />
b. Chancroid<br />
c. Herpes<br />
d. Lymphogranuloma venereum<br />
e. Granuloma inguinale<br />
13. Which <strong>of</strong> the following drugs is most likely to benefit<br />
a patient with acyclovir-resistant herpes?<br />
a. Cid<strong>of</strong>ovir<br />
b. Famciclovir<br />
c. Valacyclovir<br />
d. Penciclovir<br />
e. Zidovudine<br />
14. Which <strong>of</strong> the following is least likely to mimic molluscum<br />
contagiosum in an HIV-positive person?<br />
a. Cryptococcus<br />
b. Penicillium marneffei<br />
c. Histoplasmosis<br />
d. Condyloma acuminatum<br />
e. Granuloma inguinale<br />
15. Which <strong>of</strong> the following statements is false?<br />
a. <strong>An</strong>al cancer is the most common reportable cancer<br />
among HIV-positive men.<br />
b. <strong>An</strong>al cancer is 7 times more common in homosexual<br />
men with HIV than those who are HIV seronegative.<br />
c. Cervical cancer in an HIV-infected patient is an<br />
AIDS-defining illness.<br />
d. Condyloma acuminatum in an HIV-positive person<br />
may contain dysplastic foci.<br />
e. Crude podophyllin resin contains mutagens.<br />
16. What effect has highly active antiretroviral therapy<br />
had on KS?<br />
a. KS is more treatment resistant.<br />
b. KS is less prevalent.<br />
c. KS is more frequently seen in HIV-positive women.<br />
d. KS is more frequently seen in hemophiliacs<br />
e. KS is more likely to be the immediate cause <strong>of</strong><br />
death in HIV-positive persons.<br />
Directions for questions 17-21: For each numbered item,<br />
choose the appropriate lettered item.<br />
a. Hepatitis C virus<br />
b. Human papillomavirus type 16<br />
c. Chancroid<br />
d. Molluscum contagiosum virus 1<br />
e. Molluscum contagiosum virus 2<br />
17. Children<br />
18. Porphyria cutanea tarda<br />
19. <strong>An</strong>al cancer<br />
20. Genital ulcers in Africa<br />
21. Facial papules in HIV-positive adults<br />
Directions for question 22: Give single best response.<br />
22. Which <strong>of</strong> the following statements is true?<br />
a. Scabies are proven to transmit HIV.<br />
b. KS in HIV-negative persons is not associated with<br />
human herpesvirus type 8.<br />
c. High recurrence rates <strong>of</strong> molluscum contagiosum<br />
are usually due to reinfection.<br />
d. HIV can frequently be found in herpetic ulcers <strong>of</strong><br />
HIV-positive persons.<br />
e. Acyclovir has direct antiretroviral activity.<br />
Directions for questions 23-27: For each numbered item,<br />
choose the appropriate lettered item.<br />
a. Foscarnet<br />
b. Cid<strong>of</strong>ovir<br />
c. Famciclovir<br />
d. Imiquimod<br />
e. Azithromycin<br />
23. May be useful topical therapy for warts and molluscum<br />
contagiosum (also available in a topical formulation)<br />
24. Requires thymidine kinase for activation
J AM ACAD DERMATOL<br />
VOLUME 43, NUMBER 3<br />
25. Approved by the Centers for Disease Control and<br />
Prevention (CDC) in intravenous form for acyclovirresistant<br />
herpes<br />
26. Nucleotide analog<br />
27. Recommended by the CDC for therapy <strong>of</strong> chancroid<br />
in HIV-positive persons<br />
Directions for questions 28-31: Give single best response.<br />
28. What is the approximate relative increase in risk <strong>of</strong><br />
HIV transmission from having a <strong>sexually</strong> <strong>transmitted</strong><br />
disease?<br />
a. 1- to 2-fold<br />
b. 3- to 5-fold<br />
c. 6- to 10-fold<br />
d. 11- to 20-fold<br />
e. 21- to 50-fold<br />
29. Which statement is false regarding herpetic ulcers in<br />
HIV-positive persons?<br />
a. Hyperkeratotic verrucous lesions may resemble<br />
condyloma acuminatum.<br />
b. Higher doses <strong>of</strong> antiherpes agents may be required.<br />
c. Ulcers may be coinfected with cytomegalovirus.<br />
d. Therapy may prevent visceral spread <strong>of</strong> HSV.<br />
e. Foscarnet therapy has the same safety pr<strong>of</strong>ile as<br />
acyclovir.<br />
AVAILABILITY OF JOURNAL BACK ISSUES<br />
CME examination 435<br />
30. Which statement is true regarding scabies in HIV-positive<br />
persons?<br />
a. Mites are difficult to detect.<br />
b. Crusted lesions are more pruritic than papular<br />
lesions.<br />
c. Papular and crusted lesions are not mutually exclusive.<br />
d. Crusted scabies is clearly distinguishable clinically<br />
from eczema.<br />
e. Plaques <strong>of</strong> crusted scabies rarely fissure.<br />
31. Which statement is false regarding granuloma<br />
inguinale in HIV-positive persons?<br />
a. It is strongly associated with HIV transmission.<br />
b. CDC-recommended treatment <strong>of</strong> granuloma<br />
inguinale is different than in HIV-negative persons.<br />
c. The mean duration <strong>of</strong> ulcer healing may be longer<br />
in HIV-positive persons.<br />
d. Greater tissue destruction may be seen in HIV-positive<br />
persons.<br />
e. Extragenital dissemination has been reported in<br />
HIV-positive persons.<br />
As a service to our subscribers, copies <strong>of</strong> back issues <strong>of</strong> the Journal <strong>of</strong> the American Academy <strong>of</strong><br />
<strong>Dermatology</strong> for the preceding 5 years are maintained and are available for purchase from Mosby until<br />
inventory is depleted. The following quantity discounts are available: 25% <strong>of</strong>f on quantities <strong>of</strong> 12 to 23,<br />
and one third <strong>of</strong>f on quantities <strong>of</strong> 24 or more. Please write to Mosby, Subscription Customer Service,<br />
6277 Sea Harbor Dr, Orlando, FL 32887, or call 800-654-2452 or 407-345-4000 for information on availability<br />
<strong>of</strong> particular issues and prices. If unavailable from the publisher, photocopies <strong>of</strong> complete issues<br />
may be purchased from Bell & Howell Information and Learning, 300 N Zeeb Rd, <strong>An</strong>n Arbor, MI 48106,<br />
(313)761-4700.
1. c<br />
2. e<br />
3. b<br />
4. e<br />
5. a<br />
6. e<br />
7. a<br />
8. d<br />
9. d<br />
10. b<br />
11. b<br />
12. c<br />
13. a<br />
14. e<br />
15. a<br />
16. b<br />
436<br />
<strong>An</strong>swers to CME examination<br />
Identification No. 800-109<br />
September 2000 issue <strong>of</strong> the Journal <strong>of</strong> the American Academy <strong>of</strong> <strong>Dermatology</strong><br />
Questions 1-31, Czelusta A, Yen-Moore A, Tyring SK. J Am Acad Dermatol 2000;43:409-32.<br />
17. d<br />
18. a<br />
19. b<br />
20. c<br />
21. e<br />
22. d<br />
23. d<br />
24. c<br />
25. a<br />
26. b<br />
27. e<br />
28. b<br />
29. e<br />
30. c<br />
31. b<br />
RECEIVE TABLES OF CONTENTS BY E-MAIL<br />
To receive the tables <strong>of</strong> contents by e-mail, sign up through our Web site at:<br />
http://www.mosby.com/jaad<br />
Choose E-mail Notification.<br />
Simply type your e-mail address in the box and click the Subscribe button.<br />
Alternatively, you may send an e-mail message to<br />
majordomo@mosby.com.<br />
Leave the subject line blank and type the following as the body <strong>of</strong> your message:<br />
subscribe jaad_toc<br />
You will receive an e-mail message confirming that you have been added to the mailing<br />
list. Note that table <strong>of</strong> contents e-mails will be sent out when a new issue is posted to<br />
the Web site.