Term Owner and Policy Change Form - Fidelity
Term Owner and Policy Change Form - Fidelity
Term Owner and Policy Change Form - Fidelity

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
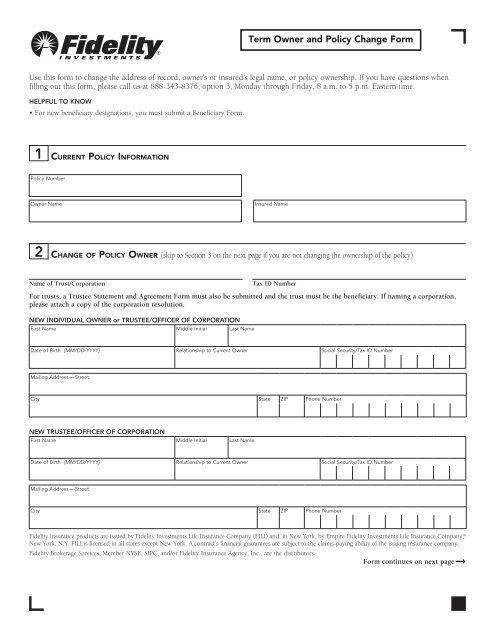
<strong>Term</strong> <strong>Owner</strong> <strong>and</strong> <strong>Policy</strong> <strong>Change</strong> <strong>Form</strong><br />
Use this form to change the address of record, owner’s or insured’s legal name, or policy ownership. If you have questions when<br />
filling out this form, please call us at 888-343-8376, option 3, Monday through Friday, 8 a.m. to 5 p.m. Eastern time.<br />
HELPFUL TO KNOW<br />
• For new beneficiary designations, you must submit a Beneficiary <strong>Form</strong>.<br />
1 CURRENT POLICY INFORMATION<br />
<strong>Policy</strong> Number<br />
<strong>Owner</strong> Name Insured Name<br />
2 CHANGE OF POLICY OWNER (skip to Section 3 on the next page if you are not changing the ownership of the policy)<br />
Name of Trust/Corporation Tax ID Number<br />
For trusts, a Trustee Statement <strong>and</strong> Agreement <strong>Form</strong> must also be submitted <strong>and</strong> the trust must be the beneficiary. If naming a corporation,<br />
please attach a copy of the corporation resolution.<br />
NEW INDIVIDUAL OWNER or TRUSTEE/OFFICER OF CORPORATION<br />
First Name Middle Initial Last Name<br />
Date of Birth (MM/DD/YYYY) Relationship to Current <strong>Owner</strong> Social Security/Tax ID Number<br />
Mailing Address — Street<br />
City State ZIP Phone Number<br />
NEW TRUSTEE/OFFICER OF CORPORATION<br />
First Name Middle Initial Last Name<br />
Date of Birth (MM/DD/YYYY) Relationship to Current <strong>Owner</strong> Social Security/Tax ID Number<br />
Mailing Address — Street<br />
City State ZIP Phone Number<br />
<strong>Fidelity</strong> insurance products are issued by <strong>Fidelity</strong> Investments Life Insurance Company (FILI) <strong>and</strong>, in New York, by Empire <strong>Fidelity</strong> Investments Life Insurance Company, ®<br />
New York, N.Y. FILI is licensed in all states except New York. A contract’s financial guarantees are subject to the claims-paying ability of the issuing insurance company.<br />
<strong>Fidelity</strong> Brokerage Services, Member NYSE, SIPC, <strong>and</strong>/or <strong>Fidelity</strong> Insurance Agency, Inc., are the distributors.<br />
<strong>Form</strong> continues on next page ➞
3 CHANGE OWNER/INSURED ADDRESS OR NAME<br />
If changing name, attach a photocopy of a marriage certifi cate, divorce decree, or other court document showing the new name.<br />
4 AUTHORIZED SIGNATURES (This section must be completed for any changes.)<br />
• I (We) authorize the preceding changes to the above-referenced policy.<br />
• I (We) have read my (our) policy <strong>and</strong> underst<strong>and</strong> the effects of these changes.<br />
• <strong>Owner</strong>ship of this policy will be transferred when this form is signed, received, <strong>and</strong> recorded at the Life Insurance Service Center.<br />
4a CURRENT OWNER SIGNATURE (ALL Current <strong>Owner</strong>s must sign.)<br />
X<br />
SIGNATURE OF CURRENT OWNER/TRUSTEE DATE SIGNATURE OF CURRENT OWNER/TRUSTEE DATE<br />
X<br />
<strong>Change</strong> your name <strong>Owner</strong> Insured<br />
<strong>Form</strong>er Name<br />
Name M.I. Last Name Social Security or Taxpayer ID Number<br />
New Name<br />
Name M.I. Last Name<br />
<strong>Change</strong> your address <strong>Owner</strong> Insured<br />
Mailing Address — Street<br />
City State ZIP Phone Number<br />
SIGNATURE OF WITNESS DATE SIGNATURE OF WITNESS DATE<br />
4b NEW OWNER/TRUSTEE/CORPORATE OFFICER SIGNATURE (ALL New <strong>Owner</strong>s must sign. Required only for changes in policy<br />
ownership in Section 2.)<br />
• You must sign for income tax identification. I certify under penalties of perjury that (1) the Social Security number or tax identification number<br />
provided is correct, <strong>and</strong> (2) the IRS has not notified me that I am subject to 20% backup withholding or has notified me that I am no longer<br />
subject to such backup withholding. (Note: If any or all of item (2) is not true, please cross out this part before signing.)<br />
X<br />
SIGNATURE OF NEW OWNER/TRUSTEE/OFFICER DATE SIGNATURE OF NEW OWNER/TRUSTEE/OFFICER DATE<br />
617501.2.0<br />
1.943930.101<br />
Please mail this form to: Life Insurance Service Center, P.O. Box 724507, Atlanta, GA 31139-2049<br />
Overnight mail: <strong>Fidelity</strong> Investments, Suite 300 3rd Floor, 6425 Powers Ferry Road, Atlanta, GA 30339<br />
X<br />
X<br />
X