How to Use Your Pharmacy Benefit - Tufts Health Plan
How to Use Your Pharmacy Benefit - Tufts Health Plan
How to Use Your Pharmacy Benefit - Tufts Health Plan

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
YOUR PHARMACY BENEFIT<br />
<strong>Your</strong> <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> benefits include coverage for prescription drugs.<br />
Here is a guide <strong>to</strong> help you make the most of your prescription drug benefit.<br />
As you may be aware, prescription drug prices vary–including drugs used <strong>to</strong> treat the same condition. We place<br />
prescription drugs in<strong>to</strong> three tiers (or levels) <strong>to</strong> help you and your doc<strong>to</strong>r choose the most cost-effective option for the<br />
medication you need. Each tier has a specific copay amount that you pay when you fill or order your prescription.
YOUR PHARMACY B<br />
Things that may affect the<br />
cost of your drugs:<br />
n If your doc<strong>to</strong>r prescribes a Tier-3 drug, you can<br />
work with him or her <strong>to</strong> determine if there is an<br />
appropriate drug available that will cost less.<br />
n If your plan has a deductible or a coinsurance<br />
requirement, you may have <strong>to</strong> pay all or part of<br />
the cost of your drug until your deductible or<br />
coinsurance amount is met.<br />
DEDUCTIBLE<br />
The amount of money you need <strong>to</strong> pay out-of-pocket<br />
before the health plan begins <strong>to</strong> pay eligible claims.<br />
COINSURANCE<br />
The percentage of cost members must pay for some<br />
covered services. The percentage you are required <strong>to</strong><br />
pay depends on your particular plan.<br />
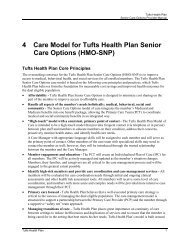
TIER LEVEL TIER COPAY TIER DESCRIPTION<br />
Tier 1 Lowest<br />
cost<br />
Tier 2 Middle<br />
cost<br />
Tier 3 Highest<br />
cost<br />
Includes most generic<br />
prescription drugs<br />
on our list of<br />
covered drugs<br />
Includes generics<br />
and brand-name<br />
prescription drugs<br />
on our list of<br />
covered drugs<br />
Includes the most costly<br />
covered generic and<br />
brand-name drugs not on<br />
Tier 1 or Tier 2<br />
What tier is my drug on?<br />
Finding out which tier your drug is on is easy.<br />
Go <strong>to</strong> tuftshealthplan.com and click on the<br />
I’m a member tab and click <strong>Pharmacy</strong>.<br />
On the <strong>Pharmacy</strong> screen, click on one of the following<br />
links depending on what plan you have:<br />
n Massachusetts employer-based plans<br />
n Massachusetts individuals and families<br />
n Rhode Island employer-based plans<br />
n Select Network and Connec<strong>to</strong>r Commonwealth<br />
Saver <strong>Plan</strong>s<br />
Search for the name of your drug. If it’s listed,<br />
you’ll see either the name of the drug or its generic<br />
equivalent, the tier that it is listed on, and any<br />
pharmacy programs, if applicable. Please note that<br />
a drug’s tier placement can change at any time<br />
throughout the year.<br />
Log in <strong>to</strong> mytuftshealthplan.com and click on<br />
View <strong>Benefit</strong>s and Coverage and then click<br />
on <strong>Pharmacy</strong> <strong>to</strong> check your drug coverage<br />
and cost.
ENEFIT<br />
Does my drug need special approval?<br />
Once you find your drug, you will know if it needs special approval if you see one of the following codes listed next<br />
<strong>to</strong> the drug name. If special approval is not required, you can go ahead and get your prescription filled.<br />
PA: Prior authorization<br />
NC: Non-covered<br />
If one of the above codes is listed next <strong>to</strong> your drug,<br />
please follow the instructions below in order <strong>to</strong> get<br />
approval before getting your prescription filled.<br />
PA (prior authorization):<br />
Some drugs must meet certain criteria before they<br />
are covered. Contact the provider who has written<br />
your prescription. If your provider believes a drug with<br />
a PA is necessary for your treatment, he or she may<br />
submit a request for coverage by faxing a Universal<br />
<strong>Pharmacy</strong> Medical Review Request Form–available<br />
at tuftshealthplan.com–<strong>to</strong> <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong>. We will<br />
cover the drug if it meets our medical necessity<br />
coverage guidelines. If the request is approved,<br />
you will be covered for your prescription. If it is<br />
not approved, you can appeal the decision.<br />
NC (non-covered):<br />
Certain drugs like those that are available over-the<br />
counter, are experimental, or have generic equivalents,<br />
may not be covered by <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong>. Contact the<br />
provider who has written your prescription. If your<br />
provider believes a non-covered drug is necessary for<br />
your treatment, he or she may submit a request for<br />
coverage by faxing a Universal <strong>Pharmacy</strong> Medical<br />
Review Request Form–available at tuftshealthplan.<br />
com–<strong>to</strong> <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong>. We will cover the drug if<br />
it meets our medical necessity coverage guidelines.<br />
If the request is approved, you will be covered for<br />
your prescription. If it is not approved, you can<br />
appeal the decision.<br />
QL: Quantity limitation<br />
ST PA : Step therapy<br />
SP: Designated specialty<br />
pharmacy<br />
QL (quantity limitation):<br />
There may be a limit on how much of a drug you can<br />
get for a specific time period. You are covered for up<br />
<strong>to</strong> the quantity posted in our list of covered drugs. If<br />
your provider believes it is necessary for you <strong>to</strong> take<br />
more than the quantity limit posted on the list, he or<br />
she may submit a Universal <strong>Pharmacy</strong> Medical Review<br />
Request Form <strong>to</strong> request coverage.<br />
ST PA (step therapy):<br />
You may be required <strong>to</strong> try a certain drug <strong>to</strong> treat a<br />
specific medical condition before <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong><br />
will approve the coverage of another drug <strong>to</strong> treat the<br />
same condition. Check the step therapy document in<br />
the <strong>Pharmacy</strong> section at tuftshealthplan.com/members<br />
<strong>to</strong> confirm the step your drug is on. If you have not<br />
previously taken the steps required by our pharmacy<br />
coverage guidelines, and your provider believes the<br />
drug prescribed for you is medically necessary, he<br />
or she may submit a Universal <strong>Pharmacy</strong> Medical<br />
Review Request Form <strong>to</strong> request coverage. New<br />
members–call us if you are currently taking<br />
a step therapy drug from another plan.<br />
SP (designated specialty pharmacy):<br />
Prescriptions for certain specialty drugs can be filled<br />
only at designated specialty pharmacies. Call the<br />
designated specialty pharmacy provider indicated in<br />
your search results of covered drugs or contact the<br />
<strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> Member Services Department at the<br />
number on your ID card <strong>to</strong> help ensure that you receive<br />
your drug without interruption.
The list of drugs covered by our pharmacy benefit<br />
is called our formulary. Most drugs are included<br />
in our formulary.<br />
We use a variety of approaches <strong>to</strong> manage your<br />
pharmacy benefit. Some of these approaches<br />
include the three-tier pharmacy copayment, prior<br />
authorization, step therapy, quantity limitation,<br />
and designated specialty pharmacy programs.<br />
QUICK TIPS TO SAVE MONEY<br />
* Get a prescription for a generic drug<br />
when possible<br />
* <strong>Use</strong> CVS Caremark Mail Service <strong>Pharmacy</strong><br />
for maintenance medications<br />
* Talk <strong>to</strong> your doc<strong>to</strong>r about less expensive<br />
alternatives for your medications<br />
What if my drug is not listed?<br />
If your drug is not listed, call our Member Services<br />
Department at the number printed on your ID card.
Where do I get my<br />
prescription filled?<br />
<strong>Use</strong> a Participating Retail <strong>Pharmacy</strong><br />
Go <strong>to</strong> any of the 63,000 participating retail pharmacies in the CVS Caremark network <strong>to</strong> obtain most covered<br />
drugs. The list of participating retail pharmacies includes most independent pharmacies as well as the major chain<br />
pharmacies, such as Walgreens and Rite Aid, in addition <strong>to</strong> CVS locations. Medications with quantity limitations<br />
should not be filled through CVS Caremark Mail Service <strong>Pharmacy</strong>.<br />
<strong>Use</strong> CVS Caremark Mail Service <strong>Pharmacy</strong><br />
Based on your benefits, you may be able <strong>to</strong> save money by using the CVS Caremark Mail Service <strong>Pharmacy</strong> for most<br />
covered maintenance medications. Maintenance medications are those that you refill every month for conditions like<br />
diabetes, high blood pressure, and asthma.<br />
Once you have all the necessary approvals (if required) for your drugs, you can start getting your prescriptions<br />
through CVS Caremark Mail Service <strong>Pharmacy</strong>–you may save time and money. You will need the following:<br />
n <strong>Your</strong> <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> ID card<br />
n Drug name<br />
n <strong>Your</strong> doc<strong>to</strong>r’s name and phone number<br />
n Shipping address<br />
n Credit card information<br />
Instructions:<br />
1. Call CVS Caremark at 888-424-6618, Monday through Friday, 8 a.m. <strong>to</strong> 8 p.m.<br />
2. Let the representative know that you want <strong>to</strong> start using the mail-order service.<br />
3. Once the representative has your information, he or she will contact your doc<strong>to</strong>r for a 90-day prescription of your<br />
current medicine.<br />
Once you begin receiving medications by mail, you can order refills easily online or by phone.<br />
For Massachusetts members, and in rare instances when the prescription is for a designated specialty drug, the<br />
prescription can be filled only through participating designated specialty pharmacies.<br />
<strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> and CVS Caremark<br />
As our pharmacy benefits manager, CVS Caremark reviews and processes your claims when you<br />
purchase prescription medications. Members covered by our pharmacy benefit may fill prescriptions<br />
at any of the more than 63,000 CVS Caremark-participating pharmacies, which include retail chain s<strong>to</strong>res,<br />
independent pharmacies, and designated specialty pharmacies, in addition <strong>to</strong> CVS/pharmacy locations.<br />
The CVS Caremark Mail Service <strong>Pharmacy</strong> is required for HMO Select Network members who take<br />
maintenance medications.<br />
FOR MORE INFORMATION<br />
<strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong> Member Services: 800-462-0224<br />
tuftshealthplan.com
TIER 1 COPAYMENT<br />
ACETAMINOPHEN-CODEINE<br />
ACYCLOVIR<br />
ALBUTEROL SULFATE QL<br />
ALENDRONATE SODIUM<br />
ALLOPURINOL<br />
ALPRAZOLAM<br />
AMITRIPTYLINE HCL<br />
AMLODIPINE BESYLATE<br />
AMLODIPINE BESYLATE-BENAZEP<br />
AMOX TR-POTASSIUM CLAVULANA<br />
AMOXICILLIN<br />
AMPHETAMINE SALT COMBO<br />
APRI*<br />
ATENOLOL<br />
AVIANE*<br />
AZITHROMYCIN<br />
BENZONATATE<br />
BETAMETHASONE DIPROPIONATE<br />
BUPROPION HCL<br />
BUPROPION HCL SR<br />
BUPROPION XL<br />
BUSPIRONE HCL<br />
BUTALBITAL-ACETAMINOPHEN-CA<br />
CAMILA*<br />
CARVEDILOL<br />
CEPHALEXIN<br />
CHERATUSSIN AC<br />
CHLORHEXIDINE GLUCONATE<br />
CHLORTHALIDONE<br />
CIPROFLOXACIN HCL<br />
CITALOPRAM HBR<br />
CLINDAMYCIN HCL<br />
CLINDAMYCIN PHOSPHATE<br />
CLOBETASOL PROPIONATE<br />
CLONAZEPAM<br />
CLONIDINE HCL<br />
CLOTRIMAZOLE-BETAMETHASONE<br />
CRYSELLE*<br />
CYCLOBENZAPRINE HCL<br />
TIER 2 COPAYMENT<br />
ADVAIR DISKUS QL<br />
ANDROGEL<br />
ATORVASTATIN CALCIUM<br />
BENICAR<br />
CLOPIDOGREL<br />
COLCRYS QL<br />
DIOVAN<br />
ENBREL SP;PA;QL<br />
QL;STPA<br />
ABILIFY<br />
CELEBREXPA CIALIS QL<br />
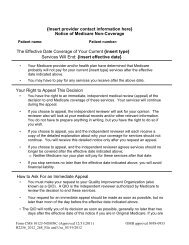
CYMBALTAQL;STPA Top 200 Covered Drugs<br />
This is a list of the 200 medications most used by <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong><br />
members. This is not a complete list of drugs covered by the <strong>Tufts</strong> <strong>Health</strong> <strong>Plan</strong><br />
pharmacy benefit. For a complete list, visit tuftshealthplan.com. For more detailed<br />
benefit information, please review your benefit<br />
TIER 3 COPAYMENT<br />
DESONIDE<br />
DEXTROAMPHETAMINE-AMPHETAMI<br />
DIAZEPAM<br />
DICLOFENAC SODIUM<br />
DILTIAZEM 24HR ER<br />
DIVALPROEX SODIUM<br />
DOXAZOSIN MESYLATE<br />
DOXYCYCLINE HYCLATE<br />
ENALAPRIL MALEATE<br />
ENPRESSE*<br />
ERYTHROMYCIN<br />
ESTRADIOL<br />
FENOFIBRATE<br />
FINASTERIDE<br />
FLUCONAZOLE<br />
FLUOCINONIDE<br />
FLUORIDE<br />
FLUOXETINE HCL<br />
FLUTICASONE PROPIONATE<br />
FOLIC ACID<br />
FUROSEMIDE<br />
GABAPENTIN<br />
GEMFIBROZIL<br />
GIANVI*<br />
GLIMEPIRIDE<br />
GLIPIZIDE<br />
GLIPIZIDE ER<br />
GLYBURIDE<br />
HYDROCHLOROTHIAZIDE<br />
HYDROCODONE-ACETAMINOPHEN<br />
HYDROCORTISONE<br />
HYDROMORPHONE HCL<br />
HYDROXYCHLOROQUINE SULFATE<br />
HYDROXYZINE HCL<br />
IBUPROFEN<br />
INDOMETHACIN<br />
IOPHEN-C NR<br />
JUNEL*<br />
JUNEL FE*<br />
EPIPEN 2-PAK QL<br />
ESCITALOPRAM OXALATE<br />
FLOVENT HFA QL<br />
HUMALOG<br />
HUMIRA SP;PA;QL<br />
JANUVIA<br />
LANTUS<br />
LANTUS SOLOSTAR<br />
DIOVAN HCT<br />
LEXAPRO STPA<br />
PANTOPRAZOLE SODIUM STPA<br />
PREMARIN<br />
Please note: A drug’s tier placement may change at any time during the year.<br />
The list of Top 200 Covered Drugs is current as of January 2013.<br />
*Generic product covered without copayment under Women’s <strong>Health</strong> Preventive<br />
Services Initiative.<br />
KARIVA*<br />
KETOCONAZOLE<br />
LABETALOL HCL<br />
LAMOTRIGINE<br />
LATANOPROST<br />
LEVETIRACETAM<br />
LEVOFLOXACIN<br />
LEVOTHYROXINE SODIUM<br />
LEVOXYL<br />
LISINOPRIL<br />
LISINOPRIL-HYDROCHLOROTHIAZ<br />
LITHIUM CARBONATE<br />
LORAZEPAM<br />
LOSARTAN POTASSIUM<br />
LOSARTAN-HYDROCHLOROTHIAZID<br />
LOVASTATIN<br />
LUTERA*<br />
MELOXICAM<br />
METFORMIN HCL<br />
METFORMIN HCL ER<br />
METHOTREXATE<br />
METHYLPHENIDATE HCL<br />
METHYLPREDNISOLONE<br />
METOPROLOL SUCCINATE<br />
METOPROLOL TARTRATE<br />
METRONIDAZOLE<br />
MICROGESTIN FE*<br />
MINOCYCLINE HCL<br />
MIRTAZAPINE<br />
MUPIROCIN<br />
NAPROXEN<br />
NECON*<br />
NIFEDIPINE ER<br />
NITROFURANTOIN MONO-MACRO<br />
NORTREL*<br />
NORTRIPTYLINE HCL<br />
NYSTATIN<br />
OCELLA*<br />
OMEPRAZOLE QL<br />
METHYLPHENIDATE ER<br />
MONTELUKAST SODIUM<br />
NASONEX QL<br />
NOVOLOG<br />
NUVARING<br />
ONE TOUCH ULTRA TEST STRIPS<br />
OXYCONTIN QL<br />
PROAIR HFA QL<br />
PA; QL<br />
SUBOXONE<br />
SYNTHROID<br />
VENTOLIN HFAQL VIAGRAQL ONDANSETRON HCL QL<br />
ONDANSETRON ODT QL<br />
OXCARBAZEPINE<br />
OXYCODONE HCL<br />
OXYCODONE-ACETAMINOPHEN<br />
PAROXETINE HCL<br />
PENICILLIN V POTASSIUM<br />
PRAVASTATIN SODIUM<br />
PREDNISOLONE ACETATE<br />
PREDNISOLONE SODIUM PHOSPHA<br />
PREDNISONE<br />
PROPRANOLOL HCL<br />
QUINAPRIL HCL<br />
RANITIDINE HCL<br />
RECLIPSEN*<br />
RISPERIDONE<br />
SERTRALINE HCL<br />
SIMVASTATIN<br />
SPIRONOLACTONE<br />
SPRINTEC*<br />
SULFAMETHOXAZOLE-TRIMETHOPR<br />
SUMATRIPTAN SUCCINATE QL<br />
TAMOXIFEN CITRATE<br />
TAMSULOSIN HCL<br />
TOPIRAMATE<br />
TRAMADOL HCL<br />
TRAZODONE HCL<br />
TRETINOIN PA<br />
TRI-SPRINTEC*<br />
TRIAMCINOLONE ACETONIDE<br />
TRIAMTERENE-HCTZ<br />
VALACYCLOVIR<br />
VENLAFAXINE HCL<br />
VENLAFAXINE HCL ER<br />
VERAPAMIL ER<br />
VITAMIN D2<br />
WARFARIN SODIUM<br />
ZOLPIDEM TARTRATE QL<br />
ZOVIA 1-35E*<br />
QUETIAPINE FUMARATE STPA<br />
SPIRIVA QL<br />
STRATTERA QL<br />
SYMBICORT QL<br />
VAGIFEM<br />
VYVANSE STPA<br />
ZETIA<br />
2/13 - 19380