Transcortical anesthesia as a first-line treatment for children: - Rident
Transcortical anesthesia as a first-line treatment for children: - Rident
Transcortical anesthesia as a first-line treatment for children: - Rident

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Paediatric Odontology<br />
Professional training<br />
E. MOULIS 1 , O. CHABADEL 2 , N. ESCUDERO-PAPOT 2 , M.C. GOLDSMITH 3<br />
<strong>Transcortical</strong> <strong>anesthesia</strong><br />
<strong>as</strong> a <strong>first</strong>-<strong>line</strong> <strong>treatment</strong><br />
<strong>for</strong> <strong>children</strong>:<br />
Minimal doses <strong>for</strong> maximum<br />
effectiveness?<br />
Intraosseous <strong>anesthesia</strong> <strong>for</strong> a child is an effective<br />
technique, able to be used <strong>as</strong> <strong>first</strong>-<strong>line</strong> <strong>treatment</strong> or <strong>as</strong> a<br />
complement <strong>for</strong> a local or local-regional <strong>anesthesia</strong>. As a<br />
<strong>first</strong>-<strong>line</strong> <strong>treatment</strong>, intraosseous <strong>anesthesia</strong> allows an<br />
immediate, painless <strong>anesthesia</strong>, and by limiting the<br />
<strong>anesthesia</strong> of the soft tissues it considerably reduces the<br />
risk of post-operative bites, in particular of the lower lip.<br />
However, the use of this technique and in particular<br />
Quick-Sleeper <strong>for</strong> a child requires carrying out a<br />
preoperative radiographic x-ray, in order to accurately<br />
locate the cortical per<strong>for</strong>ation site, allowing a rigorous<br />
training to optimise the results and to adapt the procedure<br />
to the various clinical situations. Beside these undeniable<br />
clinical advantages <strong>for</strong> a child, the intradiploic injection of<br />
the anesthetic solution also makes it possible to both<br />
decre<strong>as</strong>e the anesthetic quantity of solution injected, and<br />
to limit the toxicity.<br />
Key words<br />
Anesthesia, <strong>children</strong>, intradiploic<br />
The improvement of the conditions of local <strong>anesthesia</strong> <strong>for</strong> a child<br />
is a permanent research <strong>for</strong> the pediatric odontologists, and<br />
correctly translates their conception to work in greatest com<strong>for</strong>t,<br />
without pains and adverse effects. Thus the ideal <strong>anesthesia</strong><br />
would be painless, immediate, without failures, without<br />
after-effects (bites, inflammations or necroses) and per<strong>for</strong>med<br />
completely safely. The m<strong>as</strong>tery of the different techniques, the<br />
knowledge of the anatomy and pharmacology on local<br />
anaesthetics and on v<strong>as</strong>oconstrictors are a prerequisite to the<br />
<strong>anesthesia</strong>’s success. Moreover, the use of<br />
electronically-controlled injection systems and the realisation of<br />
transcortical or intraosseous injections make it possible today to<br />
still improve the conditions of local <strong>anesthesia</strong>, avoiding the<br />
failures in more delicate situations of the mandibular molars<br />
and/or in inflammatory stages. In this local <strong>anesthesia</strong><br />
optimisation view, the use of Quick-Sleeper represents <strong>for</strong> the<br />
child or the teenager an undeniable contribution and constitutes<br />
an additional instrument to improve the effectiveness of our<br />
<strong>anesthesia</strong>, while limiting their toxicity by reducing the quantity of<br />
anesthetic solution injected.<br />
1. University conference lecturer, hospital practitioner, pediatric<br />
odontology, Department of Research and Training in<br />
odontology, Montpellier I, France.<br />
2. Hospital-university <strong>as</strong>sistant, pediatric odontology, Department of<br />
Research and Training in odontology, Montpellier I, France.<br />
3. University Professor, hospital practitioner, pediatric odontology, Department<br />
of Research and Training in odontology, Montpellier I, France.<br />
LE CHIRURGIEN-DENTISTE DE FRANCE I N° 1321 18 OCTOBE R 2007
The pressure allows to the needle to penetrate in the intr<strong>as</strong>eptal<br />
spongy bone. Intraosseous <strong>anesthesia</strong> in temporary teeth is done<br />
in intr<strong>as</strong>eptal, in mesial or in distal of the tooth to be treated, with<br />
or without needle rotation. Preoperative radiography<br />
examination is imperative in order to visualize the structures<br />
present (Fig. 5 and 6).<br />
In young permanent teeth<br />
The periodontium acquires its maturity and sees its incre<strong>as</strong>ing<br />
degree of mineralization, the intradiploic injection then requires<br />
the per<strong>for</strong>ation of cortical by a rotation movement set to the<br />
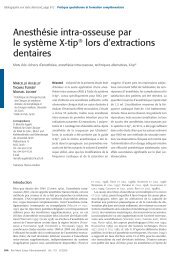
needle. The choice of injection point meets several criteria, the<br />
<strong>first</strong> relates to the needle position and orientation. The needle<br />
shall be positioned in order to remain perpendicularly to the<br />
osseous cortical exactly in the tooth middle space, following a<br />
vertical <strong>line</strong> p<strong>as</strong>sing by the papilla (Fig. 7): between 3 and 5 mm<br />
above the collar <strong>line</strong> at the jawbone and between 2 and 3 mm<br />
under the collar <strong>line</strong> at the mandible. In order to still improve the<br />
ergonomic conditions, new sites of injection are currently<br />
proposed by the originators of Quick-Sleeper.<br />
Fig. 7: Cortical per<strong>for</strong>ation sites in the upper jaw and mandible. Note the axis<br />
of the needle to the mandible which is rectified into posterior in order to<br />
remain perpendicular to the external oblique <strong>line</strong>.<br />
The per<strong>for</strong>ation of the cortical bone is per<strong>for</strong>med by a<br />
discontinuous rotation setting of the needle by foot control. The<br />
number of rotations necessary to per<strong>for</strong>ate varies according to<br />
the thickness and osseous mineralization; the number of<br />
rotations at the mandible is higher [22]. Once the per<strong>for</strong>ation is<br />
per<strong>for</strong>med, the operator h<strong>as</strong> the perception, of a low resistance of<br />
the spongy bone. The osseous per<strong>for</strong>ation is atraumatic and<br />
painless, the cortical tissue being non-innervated [7]. The<br />
LE CHIRURGIEN-DENTISTE DE FRANCE I N° 1321 18 OCTOBE R 2007<br />
needle penetration must be from 3 to 4 mm maximum. The<br />
per<strong>for</strong>ation being per<strong>for</strong>med by the needle, it is not possible to<br />
drill a dental root, in the c<strong>as</strong>e of a poor evaluation of the injection<br />
point. The recommended needles by the manufacturer are<br />
40/100 th 12 mm and 30/100 th 12 mm needles <strong>for</strong> temporary teeth,<br />
and the specific Transcort-S needles have an <strong>as</strong>ymmetrical bevel<br />
in order to facilitate the osseous per<strong>for</strong>ation. The installation of a<br />
protective sleeve around the sheath of the needle makes it<br />
possible to avoid the labial or gingival wounds related to the<br />
needle rotation setting.<br />
Intradiploic injection<br />
The intradiploic injection is the l<strong>as</strong>t stage, and it is per<strong>for</strong>med<br />
after the per<strong>for</strong>ation of the cortical bone, still by foot control.<br />
The electronically-controlled injection makes it possible to<br />
control the injection speed, and the anesthetic quantity injected.<br />
Particularly in temporary teeth, it is recommended to keep the<br />
speed injection slow in order to avoid any pain. A lighting<br />
indicator and an aural signal make it possible to visualize the<br />
injection of each quarter cartridge.<br />
Finally, a second indicator on the control box gives the<br />
possibility to me<strong>as</strong>ure injection resistance, and if resistance is<br />
too great (blocked needle, cortical not per<strong>for</strong>ated or needle in<br />
contact with a dental root), the injection automatically then stops.<br />
Thus, it is appropriate to determine the cause; purge the needle,<br />
repeat the incomplete per<strong>for</strong>ation, or change the per<strong>for</strong>ation site.<br />
The use of Quick-Sleeper, in order to give effective results,<br />
requires training and a regular practice e<strong>as</strong>ily making possible to<br />
exceed the few difficulties encountered in its initial uses.<br />
Ergonomics:<br />
The position of the handpiece, in particular in the posterior<br />
sectors is delicate sometimes, because of the need to respect the<br />
perpendicular position of the needle relative to the osseous<br />
cortical. However, the new sites of osseous per<strong>for</strong>ation have a<br />
largely improved accessibility [26].<br />
Perception of the per<strong>for</strong>ation:<br />
The perception of a less osseous resistance <strong>as</strong>sociated with the<br />
needle penetration in the spongy bone is sometimes very subtle,<br />
and can go unperceived.<br />
Blocked needle:<br />
During the per<strong>for</strong>ation by the needle rotation, the operator must<br />
imperatively not exert any pressure, with the risk to see the<br />
needle blocked by a cortical stopper and to thereafter prevent the<br />
injection
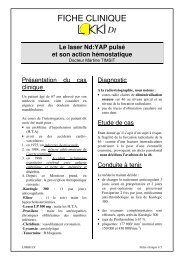
Table 1: <strong>Transcortical</strong> <strong>anesthesia</strong> results obtained with Quick-Sleeper 2 according to the <strong>treatment</strong> per<strong>for</strong>med.<br />
Teeth Dental care Success Failures Context<br />
Conservative care 8 0<br />
Temporary Pulpotomy 41 3 2 <strong>treatment</strong>s that are too long. 1 fearful child<br />
Avulsion 13 2 2 periodontal impairments (parulis)<br />
Total 61 5<br />
Conservative care 28 3 NAD<br />
Permanent Endodontics 6 1 Extended duration <strong>treatment</strong>, <strong>anesthesia</strong> too short<br />
Avulsion 8 2 2 Insufficient lingual <strong>anesthesia</strong><br />
Total 41 6<br />
Likewise, after several successive rotations, in the c<strong>as</strong>e of thick<br />
cortical bones, the needle can be clogged. In this c<strong>as</strong>e, it is<br />
possible to directly purge the needle in the oral cavity of the<br />
patient by a f<strong>as</strong>t speed injection after having retracted the needle<br />
from the bone.<br />
Duration of <strong>anesthesia</strong>:<br />
The injection of a small quantity of anesthetic (1/2 cartridge) can<br />
limit the duration of the <strong>anesthesia</strong>. But the injection of a greater<br />
quantity or the use of cartridges containing a 1/100,000 th or<br />
1/80,000 th concentration of v<strong>as</strong>oconstrictor according to<br />
pathology, make it possible to compensate <strong>for</strong> this drawback,<br />
and the choice must depend on the supposed duration of the<br />
operational procedure and the local conditions (infection,<br />
inflammation) [15, 22, 23]. The <strong>anesthesia</strong> obtained by<br />
transcortical injection is immediate, only one injection allowing<br />
the pulpal, vestibular and lingual periodontal <strong>anesthesia</strong>. The<br />
major advantage <strong>for</strong> <strong>children</strong> and in particular the very young, is<br />
the absence of labial mucosa analgesia which sometimes<br />
prevents severe bites. Operational consequences are very few;<br />
however it is necessary to note some episodes of transitory<br />
tachycardia without consequences <strong>for</strong> the general patient’s state,<br />
because the <strong>anesthesia</strong> cartridge contains a v<strong>as</strong>oconstrictor [4, 10,<br />
21, 25].<br />
L<strong>as</strong>tly, it is necessary to note possible deferred inflammation at<br />
the per<strong>for</strong>ation site, <strong>as</strong>sociated with light pains, more frequent at<br />
mandible (3.55% at the mandible against 2.83% at the jawbone)<br />
[22]. The rare contra-indications of the transcortical <strong>anesthesia</strong><br />
must be listed: significant alveolus, radicular proximity, or acute<br />
alveolar abscess, infection and inflammation decre<strong>as</strong>ing the<br />
effectiveness of the <strong>anesthesia</strong> [5, 15].<br />
RETROSPECTIVE STUDY CONDUCTED AT THE<br />
MONTPELLIER UNIVERSITY HOSPITAL<br />
Equipment and methods<br />
The objective of this study w<strong>as</strong> to evaluate the average quantity<br />
of anesthetic solution used to per<strong>for</strong>m transcortical <strong>anesthesia</strong> by<br />
Quick-Sleeper, <strong>for</strong> the realization of conventional <strong>treatment</strong>:<br />
LE CHIRURGIEN-DENTISTE DE FRANCE I N° 1321 18 OCTOBE R 2007<br />
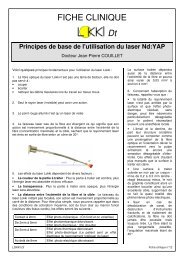
Table 2: <strong>Transcortical</strong> <strong>anesthesia</strong> results obtained with Quick-Sleeper 2 according to the <strong>treatment</strong><br />
per<strong>for</strong>med presented in the <strong>for</strong>m of percentages.<br />
Teeth Dental care Success Failures<br />
Temporary Conservative care 100% 0%<br />
Pulpotomy 93,2% 6,8%<br />
Avulsion 86,7% 13,3%<br />
Conservative care 90,3% 9,7%<br />
Permanent Endodontics 85,7% 14,3%<br />
Avulsion 80% 20%<br />
conservative care, pulpotomies, pulpectomies or avulsions.<br />
This study involved 97 <strong>children</strong>, including 54 girls and 43 boys,<br />
ages 4 to 14, treated in the pediatric odontology functional unit<br />
of Montpellier University Hospital, by D3 and Tl students (5th<br />
and 6th years).<br />
113 teeth were concerned, including 66 temporary teeth and 47<br />
permanent teeth. The <strong>anesthesia</strong> w<strong>as</strong> per<strong>for</strong>med by the same<br />
operator having attended one day of training on transcortical<br />
<strong>anesthesia</strong> and on the use of Quick-Sleeper. Children affected<br />
with general pathologies or presenting co-operation difficulties<br />
did not participate in the study. The anesthetic solution used w<strong>as</strong><br />
articaine hydrochloride 4%, with adrena<strong>line</strong> at 1/100,000 th . The<br />
average quantities of injected anesthetic solution were 0.67<br />
cartridge <strong>for</strong> temporary teeth, i.e. about 2/3 of a cartridge, and<br />
0.93 cartridge <strong>for</strong> permanent teeth. The number of rotations<br />
allowing the per<strong>for</strong>ation of cortical in temporary teeth w<strong>as</strong> 0 or 1,<br />
and in permanent teeth it varied between 1 and 4 according to the<br />
thickness of the cortical bone.<br />
Results<br />
The results are presented in tables 1, 2 and 3. The success rate <strong>for</strong><br />
temporary teeth is 92.4%, 87.2% <strong>for</strong> permanent teeth, i.e., a 90.2%<br />
success rate, and no labial bites were observed.
Table 3: Maximum number of 1.8 ml cartridges with v<strong>as</strong>oconstrictor <strong>for</strong> a normal<br />
child [18].<br />
0 to 2 years 1 cartridge<br />
3 to 4 years 2 cartridges<br />
5 to 12 years 3 cartridges<br />
> 12 years 4 cartridges<br />
Two permanent teeth (36, 46) could be extracted in an<br />
inflammatory and/or infectious situation (refractory cellulites<br />
after one week of anti-biotherapy), with the injection of only one<br />
cartridge of anesthetic solution, which confirms the power of<br />
this type of <strong>anesthesia</strong>.<br />
Finally, the failure analysis highlighted various factors:<br />
- On the one hand the difficulty <strong>for</strong> certain <strong>children</strong> to<br />
differentiate feeling and pain, the presence of a symptomatology<br />
(pulpitis or infection, parulis), which would have required a<br />
higher v<strong>as</strong>oconstrictor concentration (1/80,000 th ).<br />
- On the other hand, certain failures are related to insufficient<br />
duration of the <strong>anesthesia</strong> correlated with a relatively long<br />
duration of the <strong>treatment</strong> session, those being per<strong>for</strong>med by<br />
inexperienced student practitioners.<br />
Discussion<br />
To decre<strong>as</strong>e the toxicity of local <strong>anesthesia</strong>s and to limit their<br />
complications remain priorities <strong>for</strong> pediatric odontologists.<br />
However, the toxicity of the anesthetic solutions is not higher <strong>for</strong><br />
a child, because after 2 years, their capacity to eliminate<br />
anesthetic is incre<strong>as</strong>ed. In contr<strong>as</strong>t, the most current harmful<br />
effect remains the bite <strong>as</strong>sociated with the absence of sensitivity<br />
of the soft tissues (lower lip or tongue) [12]. Thus, "small<br />
patient" does not mean "small <strong>anesthesia</strong>", but there is a<br />
maximum number of 1.8 ml per kilo-weight anesthetic<br />
cartridges that is not to be exceeded [16-18]. The toxicity risks<br />
related to anesthetic overdose can be decre<strong>as</strong>ed using<br />
v<strong>as</strong>oconstrictors. Indeed, they make it possible to decre<strong>as</strong>e the<br />
intrav<strong>as</strong>cular p<strong>as</strong>sage of the anesthetic solution and ensure the<br />
incre<strong>as</strong>e in the duration and depth of the <strong>anesthesia</strong> by reducing<br />
its systemic effects [14,17].<br />
Thus, the Francophone Society of Oral Medicine and Oral<br />
Surgery recommends the use of v<strong>as</strong>oconstrictors in <strong>children</strong><br />
after 6 months, outside contra-indications, while respecting the<br />
maximum tolerated amounts (table 1). The real<br />
contra-indications of v<strong>as</strong>oconstrictors: an irradiated bone (40<br />
Gy dose), a pheochromocytoma (adrenal tumour), a cardiac<br />
arrhythmia and an unstable arterial hypertension, are very rare in<br />
<strong>children</strong>.<br />
LE CHIRURGIEN-DENTISTE DE FRANCE I N° 1321 18 OCTOBE R 2007<br />
The contribution of the cartridges (9 µg of v<strong>as</strong>oconstrictor in a<br />
cartridge at 1/200,000 th ) is very weak compared to the<br />
endogenous catecholamine rele<strong>as</strong>e among patients, in the event<br />
of pain, stress or anxiety [14,17]. However, the use of<br />
Quick-Sleeper <strong>as</strong> a <strong>first</strong>-<strong>line</strong> <strong>treatment</strong> enabled us to per<strong>for</strong>m<br />
care by limiting the maximum number of cartridges of<br />
<strong>anesthesia</strong> to 0.67 <strong>for</strong> temporary teeth and 0.93 <strong>for</strong> permanent<br />
teeth.<br />
These primary results should still be able to be improved by a<br />
broadened clinical practice. In terms of effectiveness, they are<br />
comparable with those of the study undertaken on <strong>children</strong> from<br />
4 to 16 years old at Rennes University Hospital showing a<br />
transcortical <strong>anesthesia</strong> success rate higher than 90%, with a<br />
quantity of anesthetic solution injected of 0.45 cartridge on<br />
average (anesthetic solution with adrena<strong>line</strong> at 1/200,000 th ) [20].<br />
These are results also comparable with the results obtained by<br />
transcortical <strong>anesthesia</strong> during previous clinical studies<br />
conducted on adult patients [20].<br />
The results can approach 100% success if we correctly choose<br />
the concentration of v<strong>as</strong>oconstrictor. However, the practice of<br />
the transcortical <strong>anesthesia</strong>s is still restricted, remaining <strong>for</strong><br />
some a complementary technique, used only <strong>as</strong> a second-<strong>line</strong><br />
<strong>treatment</strong> to improve and rein<strong>for</strong>ce an insufficient mandibular<br />
<strong>anesthesia</strong> in the posterior sectors [3, 9, 11, 19].<br />
CONCLUSION<br />
<strong>Transcortical</strong> <strong>anesthesia</strong> can be used <strong>as</strong> a <strong>first</strong>-<strong>line</strong> <strong>treatment</strong> <strong>for</strong><br />
<strong>children</strong> and teenagers, <strong>for</strong> preservation <strong>treatment</strong>, endodontic<br />
<strong>treatment</strong>, and <strong>for</strong> the avulsions, of temporary or permanent<br />
teeth. It can be used <strong>for</strong> <strong>as</strong>ymptomatic teeth but also <strong>for</strong><br />
symptomatic teeth (pulpitis, infections). In the same way,<br />
transcortical <strong>anesthesia</strong> can be used <strong>as</strong> a second-<strong>line</strong> <strong>treatment</strong>,<br />
in situations where the loco-regional (mandibular nerve block)<br />
<strong>anesthesia</strong> is insufficient. The use of this technique <strong>for</strong> a child,<br />
e<strong>as</strong>ily accepted and relatively simple, after a training period, is<br />
incontestably a new tool in the pediatric odontology therapeutic<br />
arsenal. It makes it possible to limit the amounts of injected<br />
anesthetic solution and the complications of local and regional<br />
<strong>anesthesia</strong>, in particular labial self-bites in the youngest <strong>children</strong>.<br />
Forthcoming studies will make it possible to still improve the<br />
effectiveness, the choice and the management of the quantities<br />
of anesthetic solution injected, b<strong>as</strong>ed on the different clinical<br />
situations.
BIBLIOGRAPHY<br />
1 - Artaud C.. Naulin-lfi C. L'anesthésie locale en dentisterie pédiatrique, approche<br />
clinique, Real Clin 2006:17,2:201-214.<br />
2- Bailleul-Foreslier I. Naulin-lfi C. Le parodonte de l'enfant. Encycl Med Chir,<br />
Elsevier Paris, Odontologie, 23-415-C-10, 2001, 9p.<br />
3- Bigby J., Reader A., Nusstein J., Beck M., Weaver J. Articaine <strong>for</strong> supplemenlal<br />
intraosseous <strong>anesthesia</strong> in patients with irreversible pulpitis. J Endod 2006; 32.11:<br />
1044-1047.<br />
4- Blanton P., Jeske A. Dental local anesthetics, alternative delivery methods. J Am<br />
Dent Assoc 2003; 134.2:228-234.<br />
5- Bronnec F. L'anesthésie en endodontie. Réal Clin 2006; 17,2:177-188.<br />
6- Brown R. Intraosseous <strong>anesthesia</strong>: a review. J Calif Dent Assoc 1999;<br />
27.10:785-792.<br />
7- Coggins R., Reader A,. Nist R,. Beck M., Meyers WJ. Anesthelic efticacy of the<br />
intraosseous injection in maxillary and mandibular teeth. Oral Surg Oral Med Oral<br />
Pathol Oral Radial Endod 1996; 81, 6: 634-641.<br />
8- Collier T. L'anesthésie transcorticale technique de première intention, Inf Dent<br />
2006 ;4:125-128.<br />
9- Coury K. Achieving profound <strong>anesthesia</strong> using the intraosseous technique. Text<br />
Dent J 19S7: 114, 10:34-39.<br />
10- Gallatin J., Stabile P., Reader A., Nist R., BeckM. Anesthetic efficacy and heart rate<br />
effects of the intraosseous injection of 3% mepivacaine after an inferior alveolar nerve<br />
block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 89,1: 83-87.<br />
11-Gallatin J., Reader A., Nusstein J., Beck M., Weaver J. A comparison of two<br />
intraosseous techniques in mandibular posterior teeth. JADA 2003; 134:1476-1484.<br />
12- Gaudy JF., Arreto CD. et al. Manuel d'analgésie en Odontostomatologie. M<strong>as</strong>son<br />
2nd Ed, Paris 2005, pp205.<br />
13- Kleber C. Intraosseous <strong>anesthesia</strong> implications, instrumentation and techniques.<br />
JADA 2003; 134:487-491.<br />
LE CHIRURGIEN-DENTISTE DE FRANCE I N° 1321 16 O CTOBER 2007<br />
14- Madrid C., Courtois B., Vironneau M. et al. Emploi des v<strong>as</strong>oconstricteurs en<br />
Odontostomatologie. Recommandations. Med Bucc Chir Bucc 2003 ; 9: 65-94.<br />
15- Malamed SF. Handbook of local <strong>anesthesia</strong>. Fith Ed. Elsevier Mosby, St Louis<br />
2004, pp409.<br />
16-Meechan J. How to avoid local <strong>anesthesia</strong> toxicity. Br Dent J 1998:184:334-335.<br />
17- Mortier E., Droz D., Gerdolle D. L'anesthésie locale et régionale. Réal Clin 2001 ;<br />
12, 1 : 35-46.<br />
18- Naulin-Ifi C. Anesthésie locale in Le traitement de la douleur et de l'anxiété chez<br />
l'enfant. Quintessence Internationale Paris 2007, pp125.<br />
19- Reitz J., Reader A., Nist R., Beck M., Meyers WJ. Anesthetic efficacy of the<br />
intraosseous injection of 0.9 mL ol lidocaine (1/100,000 epinephrine) to augment an<br />
inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod<br />
1998; 86.5:516-523.<br />
20- Sixou JL., Barbosa-Rogier ME. Apport de l'anesthésie transcorticale chez l'enfant<br />
et l'adolescent. Chir Dent Fr 2006; 1252: 41-46.<br />
21 - Stabile P., Reader A., Gallatin E., Beck M., Weaver J. Anesthetic efficacy and heart<br />
rate effect of the intraosseous injection of 1,5% etidocaine (1/200,000 epinephrine)<br />
after an inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol<br />
Endod 2000; 89.4:407-411.<br />
22- Villette A. Bilan de 500 Anesthésies transcorticales réalisée en première<br />
intention. J Dent Québec 2004 ;41: 239-247.<br />
23- Villette A. L'anesthésie intra-osseuse : une étape obligée vers l'anesthésie idéale.<br />
J Dent Québec 1998; 35:477-484.<br />
24- Wong JK. Adjuncts to local <strong>anesthesia</strong>: separating fact from fiction. J Can Dent<br />
Assoc 2001;67:391-397.<br />
25- Wood M., Reader A., Nusstein S., Beck M., Padgett D., Weaver J. Comparison of<br />
inlraosseous and infiltration injections <strong>for</strong> venous lidocaine blood concentrations<br />
and heart rate changes after injection of 2% lidocaine with 1/100,000 epinephrine. J<br />
Endod 2005;31, 6: 435-438.<br />
26- www.dentalhitec.com