Preoperative Cardiac Evaluation for Noncardiac Surgery: A Critical ...
Preoperative Cardiac Evaluation for Noncardiac Surgery: A Critical ...
Preoperative Cardiac Evaluation for Noncardiac Surgery: A Critical ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
abstract<br />
• Objective: To review preoperative cardiac risk stratification<br />
and management in patients undergoing<br />
noncardiac surgery.<br />
• Methods: Review of the literature, with a focus on<br />
the 2007 American College of Cardiology/American<br />
Heart Association guidelines and landmark papers.<br />
• Results: The updated guidelines emphasize preoperative<br />
clinical risk stratification and deemphasize<br />
routine preoperative cardiac testing in patients with<br />
known or suspected coronary disease. Most patients<br />
without active cardiovascular conditions who are<br />
not at very high risk can proceed to surgery without<br />
further testing. Use of preoperative noninvasive testing<br />
is warranted in selected very high-risk patients<br />
and/or if the results will change patient management.<br />
β-Blocker therapy is reasonable in higher-risk patients.<br />
However, the updated guidelines do not include<br />
data from the POISE trial, the results of which<br />
call into question the routine initiation of prophylactic<br />
preoperative β blockade. There is ongoing research<br />
concerning preoperative statin therapy, which appears<br />
to be beneficial, especially in vascular surgery<br />
patients. A notable change in the guidelines reflects<br />
recent evidence that intermediate-risk patients might<br />
not benefit from prophylactic preoperative revascularization.<br />
• Conclusion: An individualized multidisciplinary approach<br />
and risk-benefit discussion with each patient<br />
is the most prudent path to ensuring success.<br />
Each year, 100 million adults worldwide undergo noncardiac<br />
surgery, with approximately 30 million of<br />
these surgeries per<strong>for</strong>med in the United States [1–3].<br />
An increasing proportion of surgical patients are elderly<br />
and have concomitant cardiac disease. Despite advances<br />
in medical therapy and subsequent improvements in event<br />
rates, cardiovascular complications remain a major area<br />
of surgical morbidity and mortality. As a result, innumerable<br />
studies have addressed the topic of cardiovascular risk<br />
stratification and management.<br />
clinical review<br />
<strong>Preoperative</strong> <strong>Cardiac</strong> <strong>Evaluation</strong> <strong>for</strong> <strong>Noncardiac</strong><br />
<strong>Surgery</strong>: A <strong>Critical</strong> Review<br />
Bizath S. Taqui, MD, Keith McNellis, MD, Kathleen Coppola, MD, Himani Shishodia, MD, Brian Wolfe, MD,<br />
Guiliana DeFrancesch, MD, Mary G. van den Berg-Wolf, MD, Lawrence I. Kaplan, MD, and Darilyn V. Moyer, MD<br />
Since 1996, several organizations have convened expert<br />
panels to develop evidencebased guidelines. However, gaps<br />
and inconsistencies in the available data have led to differing<br />
recommendations. The 2 most commonly cited guidelines,<br />
from the American College of Physicians [4] and the American<br />
College of Cardiology/American Heart Association<br />
(ACC/AHA) [5], differed considerably when originally published<br />
in the late 1990s. Most recently, the ACC/AHA published<br />
a revised version of their guidelines [6]. Although the<br />
2007 ACC/AHA update is currently the reference standard,<br />
it has been and continues to be an impetus <strong>for</strong> debate. Thus,<br />
more than half a century after perioperative myocardial<br />
infarction (MI) was first identified as an entity, the optimal<br />
strategy <strong>for</strong> predicting and preventing surgeryassociated<br />
cardiovascular complications remains controversial.<br />
This paper will examine current areas of consensus and<br />
controversy within the field of perioperative cardiovascular<br />
evaluation with a focus on the updated ACC/AHA guidelines<br />
and a review of landmark papers.<br />
incidence and Pathophysiology of cardiac<br />
complications<br />
The incidence of perioperative MI depends on patient risk<br />
factors as well as the risk associated with surgery. It also depends<br />
on the universal definition of MI, which has recently<br />
been broadened [7]. Based on the available literature, the<br />
incidence of perioperative MI in lowrisk patients undergoing<br />
noncardiac surgery is 1% to 3% [8], but the incidence in<br />
higherrisk patients is up to 38% in some studies [9]. The<br />
variability is also related to the intensity of perioperative<br />
medical management as well as the sensitivity and specificity<br />
of the diagnostic modalities. At this time, there are no<br />
standard diagnostic criteria <strong>for</strong> perioperative MI [10]. Furthermore,<br />
since most perioperative MI are silent, the true incidence<br />
may be underestimated. Finally, incidence estimates<br />
may include data that are outdated due to the continuous<br />
advances in management of cardiac patients.<br />
From the Department of Medicine, Temple University School of Medicine, Philadelphia,<br />
PA.<br />
www.turner-white.com Vol. 16, No. 6 June 2009 JCOM 271
PreoPerative cardiac evaluation<br />
Table 1. Revised <strong>Cardiac</strong> Risk Index<br />
Lee Variables<br />
1 High-risk type of surgery<br />
2 Ischemic heart disease (includes any of the following: history<br />
of myocardial infarction; history of positive exercise test;<br />
current complaint of chest pain that is considered to be<br />
secondary to myocardial ischemia; use of nitrate therapy;<br />
electrocardiography with pathologic Q waves)<br />
3 Congestive heart failure<br />
4 History of cerebrovascular disease<br />
5 <strong>Preoperative</strong> treatment with insulin<br />
6 <strong>Preoperative</strong> serum creatinine > 2.0 mg/dL<br />
No. of<br />
Variables<br />
Risk of Major Postoperative<br />
<strong>Cardiac</strong> Complication<br />
0 0.4%<br />
1 0.9%<br />
2 7.0%<br />
≥ 3 11.0% High risk<br />
Adapted from reference 19.<br />
Most perioperative MIs fall into the non–STsegment<br />
elevation MI category [11]. Risk is highest during the first<br />
3 postoperative days. Perioperative MIs are caused by<br />
prolonged myocardial ischemia or plaque rupture and coronary<br />
thrombosis. Myocardial ischemia is caused by supply/<br />
demand mismatches. Increased demand may result from<br />
catecholamine surges that are triggered by the stress and<br />
pain associated with surgery. Hypoxia and decreased supply<br />
may occur in association with anesthesia, hypotension,<br />
and bleeding. Furthermore, surgery is a proinflammatory,<br />
hypercoagulable state, which may lead to plaque fissure and<br />
thrombosis, respectively. The precise mechanisms of perioperative<br />
ischemia and infarction are still unclear and being<br />
investigated. However, perioperative MI has been shown to<br />
be an independent risk factor <strong>for</strong> cardiovascular death and<br />
nonfatal MI during the 6 months following surgery [12].<br />
clinical risk Stratification: Patient risk Factors<br />
Since the publication of Goldman’s cardiac risk index [13],<br />
several authors have attempted to modify the original model<br />
[14–18]. In a prospective study of 4315 patients older than<br />
50 years undergoing elective surgery, Lee et al [19] developed<br />
the Revised <strong>Cardiac</strong> Risk Index (RCRI) (Table 1), which uses<br />
6 independent variables to predict risk of a major cardiac<br />
complication. Rates of major cardiac complications with 0, 1,<br />
2, and 3 or more of these factors were 0.5%, 1.3%, 4%, and 9%,<br />
respectively, in the derivation cohort and 0.4%, 0.9%, 7%, and<br />
11% in the validation cohort. Lee et al [19] noted that the model<br />
might not be as useful in patients at very low risk (length of<br />
stay < 2 days) or in those undergoing emergency surgeries.<br />
Table 2. Active <strong>Cardiac</strong> Conditions <strong>for</strong> Which the Patient<br />
Should Undergo <strong>Evaluation</strong> and Treatment Be<strong>for</strong>e<br />
<strong>Noncardiac</strong> <strong>Surgery</strong><br />
Condition Examples<br />
Unstable coronary<br />
syndromes<br />
Decompensated HF<br />
(NYHA functional<br />
class IV; worsening<br />
or new-onset HF)<br />
Unstable or severe angina*<br />
Recent MI<br />
Significant arrhythmias High-grade atrioventricular block<br />
Mobitz II atrioventricular block<br />
3rd-degree atrioventricular heart block<br />
Symptomatic ventricular arrhythmias<br />
Supraventricular arrhythmias (including<br />
atrial fibrillation) with uncontrolled ventricular<br />
rate (HR > 100 bpm at rest)<br />
Symptomatic bradycardia<br />
Newly recognized ventricular tachycardia<br />
Severe valvular<br />
disease<br />
Severe aortic stenosis<br />
Symptomatic mitral stenosis<br />
HF = heart failure; HR = heart rate; MI = myocardial infarction;<br />
NYHA = New York Heart Association. (Adapted from reference 6.)<br />
*May include “stable” angina in patients who are unusually sedentary.<br />
The Lee model is the only index to be derived during modern<br />
times and has the major advantage of reflecting current practices<br />
in anesthesia, medicine, and surgery. The Lee index was<br />
validated by Boersma et al [20] in their retrospective analysis<br />
of over 100,000 patients and is currently the preferred tool <strong>for</strong><br />
preoperative cardiac risk stratification.<br />
The current ACC/AHA guideline have designated the<br />
variables from the Lee index (all but highrisk surgery) as<br />
“clinical risk factors;” these replace the old “intermediate risk<br />
factors” category. Also in the current guidelines, patients in<br />
the “highest” clinical risk category are now designated as<br />
those with “active cardiac conditions” (Table 2). These active<br />
cardiac conditions include unstable coronary conditions, decompensated<br />
heart failure, significant arrhythmias, and severe<br />
valvular disease. Their presence precludes the per<strong>for</strong>mance<br />
of nonemergent surgery until the conditions are stabilized.<br />
The “lowest” risk category of clinical predictors do not independently<br />
predict adverse cardiac outcomes, and these minor<br />
predictors remain unchanged from the earlier guidelines.<br />
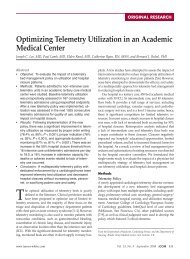
The ACC/AHA committee also identifies functional status<br />
as an important predictor of cardiac risk. This is based on<br />
evidence that suggests a correlation between an individual’s<br />
ability to per<strong>for</strong>m certain tasks and maximal oxygen uptake<br />
by treadmill testing. There are also a few observational<br />
studies linking functional capacity with perioperative outcomes.<br />
However, the incorporation of functional status into<br />
the ACC/AHA evaluation and care algorithm (Figure 1) has<br />
272 JCOM June 2009 Vol. 16, No. 6 www.turner-white.com
Step 1<br />
Step 2<br />
Step 3<br />
Step 4<br />
Vascular<br />
surgery<br />
Step 5<br />
Need <strong>for</strong> emergency<br />
noncardiac surgery?<br />
NO<br />
Active cardiac<br />
conditions<br />
NO<br />
Low-risk surgery<br />
NO<br />
Functional capacity ≥ 4<br />
METs without symptoms<br />
3 or more clinical<br />
risk factors<br />
Consider testing if it will<br />
change management †<br />
No or unknown<br />
Intermediaterisk<br />
surgery<br />
YES<br />
YES<br />
YES<br />
sparked controversy. Critics of this strategy cite that people<br />
with poor functional status are a heterogeneous group and<br />
that there are insufficient prospective data that further testing<br />
in such a group would improve perioperative outcomes.<br />
Critics also doubt if functional status adds any incremental<br />
predictive power to the RCRI.<br />
Finally, the ACC/AHA committee comments on diseasespecific<br />
risk, such as that associated with coronary artery<br />
disease (CAD), congestive heart failure (CHF), hypertension,<br />
valvular heart disease, arrhythmias, cardiomyopathy, pulmonary<br />
vascular disease, and congenital heart disease. CAD<br />
and CHF have been identified as independent predictors of<br />
perioperative cardiac complications in several studies and<br />
are topics we focus on herein. There is little in<strong>for</strong>mation regarding<br />
the impact of cardiomyopathy, pulmonary vascular<br />
disease, and congenital heart disease on perioperative outcomes.<br />
Hypertension with emphasis on risks and benefits<br />
Operating room<br />
Evaluate and treat per<br />
ACC/AHA guidelines<br />
Vascular<br />
surgery<br />
Proceed with<br />
planned surgery<br />
Proceed with planned surgery with HR control †<br />
or consider noninvasive testing if it will change management<br />
clinical review<br />
Perioperative surveillance<br />
and postoperative risk<br />
stratification and risk factor<br />
management<br />
Consider operating room<br />
Proceed with<br />
planned surgery*<br />
Proceed with<br />
planned surgery<br />
Figure 1. <strong>Cardiac</strong> evaluation and care algorithm <strong>for</strong> noncardiac surgery based on active clinical conditions, known cardiovascular<br />
disease, or cardiac risk factors <strong>for</strong> patients aged 50 years or older. HR = heart rate. *Noninvasive testing may be considered<br />
be<strong>for</strong>e surgery in specific patients with risk factors if it will change management. † Consider perioperative β blockade <strong>for</strong> populations<br />
in which this has been shown to reduce cardiac morbidity/mortality. (Adapted from reference 6.)<br />
of β and angiotensin blockade, valvular heart disease with<br />
emphasis on aortic stenosis, and arrhythmias with emphasis<br />
on atrial fibrillation are important topics in perioperative<br />
management. However, an extensive review of the literature<br />
concerning these areas is beyond the scope of this article.<br />
clinical risk Stratification: <strong>Surgery</strong>-Specific risk<br />
In his work with the Multicenter Study of Perioperative<br />
Ischemia Research Group (www.iref.org), Mangano [21]<br />
determined that cardiac complications were 2 to 5 times<br />
more likely to occur with emergency surgery procedures<br />
than with elective operations. Goldman and Detsky [13,16]<br />
also identified emergency surgery as high risk. Detsky et<br />
al also looked at surgeryspecific risk. At their institution,<br />
intraperitoneal, intrathoracic, and vascular surgeries had the<br />
highest probability of being associated with a cardiac event;<br />
these are the “highrisk” surgeries Lee et al [19] incorporated<br />
www.turner-white.com Vol. 16, No. 6 June 2009 JCOM 273<br />
YES<br />
1 or 2 clinical<br />
risk factors<br />
Intermediaterisk<br />
surgery<br />
No clinical<br />
risk factors
PreoPerative cardiac evaluation<br />
Table 3. <strong>Cardiac</strong> Risk* Stratification <strong>for</strong> <strong>Noncardiac</strong><br />
Surgical Procedures<br />
Risk Stratification Procedure Examples<br />
Vascular (reported cardiac<br />
risk often > 5%)<br />
Intermediate (reported<br />
cardiac risk generally<br />
1%–5%)<br />
Low (reported cardiac<br />
risk generally < 1%)<br />
Adapted from reference 6.<br />
Aortic and other major vascular surgery<br />
Peripheral vascular surgery<br />
Intraperitoneal and intrathoracic surgery<br />
Carotid endarterectomy<br />
Head and neck surgery<br />
Orthopedic surgery<br />
Prostate surgery<br />
Endoscopic procedures<br />
Superficial procedure<br />
Cataract surgery<br />
Breast surgery<br />
Ambulatory surgery<br />
*Risk of cardiac death and nonfatal myocardial infarction.<br />
into their index. These data, confirmed in other studies,<br />
reflect the duration and large fluid shifts associated with<br />
these procedures. Furthermore, cardiac complication rates<br />
<strong>for</strong> vascular surgery may be due to the high concurrence of<br />
CAD. Thus, the highestrisk noncardiac operation is aortic<br />
aneurysm repair, which incorporates all of these problems.<br />
The ACC/AHA committee per<strong>for</strong>med an extensive review<br />
of surgeryspecific risk and identified 3 categories of<br />
procedures (Table 3). The lowrisk group (< 1% cardiac risk)<br />
includes endoscopic and superficial procedures as well as cataract,<br />
breast, and ambulatory surgeries. The intermediaterisk<br />
group (1%–5% risk) includes a heterogeneous group of procedures<br />
(prostate, orthopedic, head and neck, intraperitoneal<br />
and intrathoracic surgeries, endovascular abdominal aortic<br />
aneurysm repair, and carotid endarterectomy). The highestrisk<br />
group (> 5% risk) is reserved <strong>for</strong> aortic, peripheral vascular,<br />
and other major vascular surgery. Unlike the Lee index,<br />
the ACC/AHA guidelines assigned highestrisk status only<br />
to certain vascular surgeries. This interpretation of the data is<br />
corroborated by most other studies, including data from the<br />
National Surgical Quality Improvement Project registry data<br />
[22]. One area of controversy surrounding the ACC/AHA review<br />
was the lack of in<strong>for</strong>mation provided about laparoscopic<br />
procedures compared with open approaches.<br />
<strong>Preoperative</strong> noninvasive testing<br />
The ACC/AHA guideline recommends use of noninvasive<br />
testing in select patients (Figure 1). Assessment of left ventricular<br />
(LV) function has not been shown to independently<br />
predict perioperative ischemic events. Furthermore, in a<br />
metaanalysis of 8 studies, resting LV ejection fraction less<br />
than 35% had only 50% sensitivity and 91% specificity in<br />
predicting postoperative heart failure. Thus, the ACC/AHA<br />
guidelines do not routinely recommend preoperative evaluation<br />
of LV function.<br />
Exercise stress testing has a limited role in preoperative<br />
risk stratification because more than 50% of patients fail to<br />
reach heart rates greater than 75% of their age predicted<br />
maximum. Also, many patients have disease that limits<br />
their ability to walk effectively. Exercise stress testing is also<br />
of limited utility in patients with baseline electrocardiogram<br />
abnormalities such as left bundle branch block, left<br />
ventricular hypertrophy with strain patterns, or ST segment<br />
deviations. Thus, pharmacologic stress testing has become<br />
the primary modality <strong>for</strong> patients requiring preoperative<br />
risk stratification. Pharmacologic stress testing can be done<br />
using nuclear imaging (dipyridamole or adenosine thallium)<br />
or echocardiography (dobutamine echocardiography).<br />
Dipyridamole and adenosine are relatively contraindicated<br />
in patients with bronchospasm or critical carotid occlusive<br />
disease. Dobutamine should be avoided in patients with<br />
serious arrhythmias, severe hypertension or hypotension,<br />
and critical aortic stenosis.<br />
A few conclusions can be made regarding the data on<br />
noninvasive testing <strong>for</strong> preoperative coronary risk stratification.<br />
First, the data should be interpreted with caution<br />
<strong>for</strong> several reasons. The majority of the studies used weak<br />
methods (retrospective design, lack of blinding, selection<br />
bias, confounding). Most studies reported low perioperative<br />
event rates. Metaanalyses of the different studies were limited<br />
by significant betweenstudy heterogeneity. The majority<br />
of the studies involved vascular surgery patients.<br />
Second, in pooled analyses comparing different diagnostic<br />
modalities [23], all of the tests demonstrated very high negative<br />
predictive values (at least 95%). However, the positive<br />
predictive values of the tests were much lower (at most 20%).<br />
Overall, there was comparable accuracy between myocardial<br />
perfusion imaging and dobutamine echocardiography [24].<br />
Perfusion imaging may be more sensitive <strong>for</strong> detecting ischemia,<br />
but dobutamine echocardiography tended to have a<br />
higher specificity and positive predictive value [25,26].<br />
Third, preoperative stress testing may be more useful<br />
if cardiac risk is quantified to severity of disease using<br />
either number and size of reversible perfusion defects (<strong>for</strong><br />
perfusion imaging) or inducible regional wall motion abnormalities<br />
(<strong>for</strong> stress echocardiography) [27,28]. Some studies<br />
suggested that the heart rate at which ischemia is induced<br />
(ischemic threshold) may also be predictive of adverse perioperative<br />
events [6].<br />
Finally, studies combining clinical risk indexes and noninvasive<br />
testing showed lack of utility of such testing in lowrisk<br />
patients. Furthermore, as new data have emerged about preoperative<br />
medical therapy and coronary revascularization,<br />
authorities are advocating against preoperative noninvasive<br />
testing <strong>for</strong> intermediaterisk patients. Two trials demonstrated<br />
274 JCOM June 2009 Vol. 16, No. 6 www.turner-white.com
that in patients at intermediate risk who were treated with optimal<br />
medical therapy (β blockers), preoperative noninvasive<br />
testing, and/or coronary revascularization provided no additional<br />
benefit [29,30]. However, data are lacking <strong>for</strong> patients at<br />
very high risk <strong>for</strong> perioperative cardiac complications because<br />
most studies included very few of these patients.<br />
Boersma et al [20] retrospectively evaluated the endpoints<br />
of perioperative cardiac death or nonfatal MI in<br />
vascular surgery patients on βblocker therapy who had undergone<br />
preoperative dobutamine echocardiography. The<br />
researchers found that lowrisk patients had the lowest rate<br />
of cardiac complications (< 1%), regardless of findings on<br />
dobutamine echocardiography. Patients at intermediate or<br />
higher risk had a low rate of complications (< 1.2%) if they<br />
had fewer than 4 segments with new wall motion abnormalities<br />
on dobutamine echocardiography. However, the rate of<br />
cardiac complications was significant (> 5%) in patients with<br />
profoundly abnormal echocardiography, despite being on<br />
β blockade. Pretest clinical probability was calculated using<br />
a score similar to the RCRI.<br />
The ACC/AHA guidelines position on preoperative noninvasive<br />
testing represented a major paradigm shift, with preoperative<br />
noninvasive testing recommended in intermediate<br />
to higherrisk patients only if “it will change management.”<br />
The strongest recommendation <strong>for</strong> consideration of testing<br />
is <strong>for</strong> vascular surgery patients who have poor or unknown<br />
functional capacity and 3 or more clinical risk factors. Patients<br />
who have good functional capacity or no clinical risk factors<br />
can proceed to surgery. For the remaining patients, there is a<br />
choice between medical management and further testing.<br />
Perioperative Medical therapy<br />
β Blockers<br />
Perioperative use of β blockers is another area of controversy.<br />
The evidence supporting the efficacy of perioperative<br />
βblocker therapy is largely based on 2 randomized controlled<br />
trials (RCTs) published in the late 1990s [31,32]. The trials<br />
were based on the theory that β blockade would improve<br />
supplydemand mismatch associated with surgery. In their<br />
landmark trial, Mangano et al [31] assigned 200 patients undergoing<br />
noncardiac surgery to atenolol (given intravenously<br />
be<strong>for</strong>e and immediately after surgery, then orally <strong>for</strong> the<br />
duration of hospitalization) or placebo. The enrolled patients<br />
had CAD or at least 2 risk factors <strong>for</strong> CAD (age > 65 years,<br />
hypertension, smoking, serum cholesterol > 6.2 mmol/L, or<br />
diabetes). Although there was no difference in perioperative<br />
MI or death, the atenolol group had significantly fewer<br />
episodes of ischemia detected on Holter monitoring and significantly<br />
lower mortality at 2 years. The principal effect was<br />
demonstrated 6 to 8 months after surgery and maintained<br />
over the entirety of the 2 years. In a major limitation of the<br />
study, the researchers did not control <strong>for</strong> pre or postoperative<br />
clinical review<br />
use of medications. More patients in the atenolol group were<br />
using angiotensinconverting enzyme inhibitors and β blockers<br />
when they were discharged.<br />
The second major RCT (DECREASE), reported by Poldermans<br />
et al [32], randomized 112 patients undergoing<br />
vascular surgery to bisoprolol versus placebo. These patients<br />
had been selected from a larger cohort due to their high<br />
clinical risk and abnormal dobutamine echocardiography<br />
findings. Bisoprolol was started at least 7 days prior to surgery<br />
and continued <strong>for</strong> 30 days postoperatively. There was a<br />
significantly lower incidence of cardiac death and nonfatal<br />
MI in the bisoprolol group. Of note, the study protocol was<br />
unblinded. Another weakness of the DECREASE study was<br />
its selective inclusion criteria, which may limit generalizability<br />
to a larger cohort of patients.<br />
This issue of inclusion criteria was addressed in 2001<br />
when Boersma et al used regression analysis to identify 7<br />
clinical risk factors that predicted adverse cardiac events<br />
(angina, prior MI, CHF, prior stroke, diabetes, renal failure,<br />
and age > 70 years) and used these criteria to analyze the<br />
1351 consecutive patients initially considered <strong>for</strong> enrollment<br />
in the Poldermans study. In patients without any risk factors,<br />
there was no benefit from β blockade. In intermediaterisk<br />
patients with up to 3 risk factors, the β blocker group had a<br />
lower risk of cardiac complications regardless of stress test<br />
findings. The same benefit occurred in higherrisk patients<br />
with at least 3 risk factors who had 4 or fewer wall motion<br />
abnormalities on dobutamine echocardiography. However,<br />
β blockers did not protect the small group of highestrisk patients<br />
with the most extensive ischemia (≥ 5 wall motion abnormalities).<br />
It should be noted that the study had problems<br />
with respect to randomization techniques and blinding.<br />
In a similar 2005 study, Lindenauer et al [33] used the<br />
RCRI to analyze an administrative database of more than<br />
780,000 patients who had undergone noncardiac surgery.<br />
Again, intermediate to higherrisk patients benefited from<br />
perioperative β blockade. However, lowrisk patients or those<br />
with diabetes actually seemed to do worse with β blockade.<br />
Limitations of the study include retrospective design, potential<br />
incorrect estimation of the number of patients who actually<br />
received β blockade, lack of data on concomitant medications,<br />
exclusion of patients with CHF and chronic obstructive<br />
pulmonary disease, and inclusion of patients undergoing<br />
urgent or emergent surgery (even though the revised cardiac<br />
index was not derived from this population).<br />
Additional studies of patients undergoing noncardiac surgery<br />
have been less favorable toward β blockers. The POBBLE<br />
[34] and MaVS [35] trials failed to show benefit of β blockade<br />
in low or intermediaterisk patients undergoing vascular<br />
surgery. Similarly, in DIPOM [36] there was no benefit from<br />
β blockade <strong>for</strong> diabetic patients undergoing noncardiac surgery.<br />
In the DIPOM study, patients given β blockade had<br />
www.turner-white.com Vol. 16, No. 6 June 2009 JCOM 275
PreoPerative cardiac evaluation<br />
Table 4. Recommendations <strong>for</strong> Perioperative β-Blocker Therapy Based on Published Randomized Clinical Trials<br />
<strong>Surgery</strong><br />
No Clinical<br />
Risk Factors<br />
significantly higher rates of hypotension and bradycardia.<br />
Of note, none of these studies used the protocol suggested<br />
by DECREASE trial. Also, these trials all used metoprolol,<br />
suggesting the possibility of class effect. Class effect was also<br />
suggested by a large database, which favored the use of longacting<br />
over shorteracting β blockers [37].<br />
The conflicting results between studies resulted in the publication<br />
of several overviews on the topic [38–41]. However, the<br />
reviews used different inclusion criteria and differed in their<br />
conclusions. In addition, the reviews were limited by the small<br />
size and heterogeneous nature of the individual trials. In the<br />
first large RCT of perioperative β blockade, the POISE investigators<br />
[42] randomized 8351 patients, most of whom were at<br />
intermediate risk, to extendedrelease metoprolol or placebo.<br />
Patients who were already on β blockers were excluded from<br />
the trial. Although the primary composite endpoint (cardiovascular<br />
death, nonfatal MI, and nonfatal cardiac arrest) was<br />
lower at 30 days in the metoprolol group, the benefits were at<br />
a cost. The metoprolol group had a higher mortality rate (most<br />
likely due to sepsis) and higher risk of stroke (possibly due to<br />
increased rates of hypotension and bradycardia). The nature<br />
of the association of sepsis with βblocker use, and whether<br />
there was causality was unclear. To further support their cautious<br />
attitude toward β blockers, the authors reflected on the<br />
relatively benign outcome in the patients with nonfatal cardiac<br />
events as opposed to the disability that was associated with<br />
nonfatal strokes. Finally, the authors were unable to identify<br />
differences in primary outcome between subgroups that had<br />
been prespecified using the RCRI.<br />
Rather than resolving the controversy surrounding perioperative<br />
beta blockade, the POISE trial may have contributed<br />
to it. The study population included patients with a<br />
high rate of cerebrovascular disease and high rates of urgent<br />
and emergent surgeries. The major criticisms of the study,<br />
however, concern dosing regimen and timing of initiation.<br />
In the POISE study, the starting dose of metoprolol was 2 to<br />
8 times the commonly prescribed dose. Also, the study drug<br />
was started only a few hours prior to surgery. This initiation<br />
time not only interferes with proper titration but may also<br />
underutilize the antiinflammatory effect of β blockade.<br />
1 or More Clinical<br />
Risk Factors CHD or High <strong>Cardiac</strong> Risk<br />
Patients Currently<br />
Taking β Blockers<br />
Vascular May be considered Reasonable Patients found to have myocardial ischemia<br />
on preoperative testing: recommended<br />
Patients without ischemia or no previous<br />
test: reasonable<br />
Recommended<br />
Intermediate risk ID May be considered Reasonable Recommended<br />
Low risk ID ID ID Recommended<br />
CHD = coronary heart disease; ID = insufficient data. (Adapted from reference 6.)<br />
This additional mechanism was first proposed to explain<br />
the longterm benefit of perioperative β blockade months<br />
after surgery, which has been demonstrated by several studies,<br />
including the original study by Mangano et al.<br />
Finally, class effect may be important because perioperative<br />
cardioprotection is regulated mainly by B1 adrenoreceptor<br />
blockade. Blocking both B1 and B2 receptors in the presence<br />
of increased adrenaline levels may lead to increased<br />
alpha stimulation and a rise in blood pressure. Bisoprolol has<br />
higher B1 selectivity compared with atenolol and metoprolol,<br />
which might explain why it has per<strong>for</strong>med better in trials.<br />
In summary, there are still several issues that require<br />
clarification regarding the use of perioperative β blockade.<br />
These include choice of β blocker as well as optimal dosage<br />
and timing of initiation and withdrawal. There does appear<br />
to be consensus in optimal heart rate, with most authorities<br />
citing targets of 55 to 65 bpm. Finally, a critical aspect remains<br />
the identification of ideal candidates <strong>for</strong> perioperative<br />
β blockers based on clinical risk. The revised cardiac risk<br />
index seemed to address this issue until the POISE trial.<br />
Additional risk indices might need to be developed to further<br />
clarify the ideal candidate. The ACC/AHA guidelines<br />
published prior to POISE recommended starting β blockers<br />
in higherrisk patients who also have ischemia on stress<br />
testing (Table 4). However, the only group who received a<br />
class 1A (high level of evidence) indication <strong>for</strong> perioperative<br />
β blockade was patients already taking β blockers.<br />
Statins<br />
Perioperative use of statins is an emerging area of study.<br />
There is a growing body of evidence that statins improve<br />
endothelial function, decrease vascular inflammation, and<br />
stabilize atherosclerotic plaques. Most data are based on<br />
observational studies [43,44]. In one of the few prospective<br />
trials to date, Durazzo et al [45] assigned 100 patients undergoing<br />
vascular surgery to atorvastatin versus placebo, with<br />
surgery scheduled an average of 30 days after randomization.<br />
There was a significantly lower incidence of cardiac<br />
complications at 6month followup in the statin group. Two<br />
large retrospective studies [46,47] of patients undergoing<br />
276 JCOM June 2009 Vol. 16, No. 6 www.turner-white.com
noncardiac surgery demonstrated significant reductions in<br />
mortality associated with perioperative statin use.<br />
Metaanalyses have also shown an overall benefit from<br />
statin use. Hindler et al [48] reported a 44% reduction in<br />
mortality associated with statin use during noncardiac<br />
surgery. The risk reduction was even higher <strong>for</strong> patients<br />
undergoing vascular surgery. In a recent review of 18 studies,<br />
Kapoor et al [49] also reported a reduction in mortality<br />
in patients receiving perioperative statin therapy. These data<br />
are limited by the retrospective nature of most of the studies<br />
as well as betweenstudy heterogeneity in patient risk as<br />
well as type, dose, and duration of the statins. Further study<br />
is required on potential side effects, including myopathy<br />
and rhabdomyolysis.<br />
<strong>Preoperative</strong> revascularization<br />
Most of the data regarding benefits of preoperative coronary<br />
revascularization are from retrospective studies. The largest<br />
retrospective review of preoperative coronary artery<br />
bypass grafting (CABG) was conducted by Eagle et al [3].<br />
In this study, patients undergoing lowerrisk surgery (urologic,<br />
orthopedic, breast, and skin), had low mortality rates<br />
regardless of whether or not they had preoperative CABG.<br />
However, among patients undergoing thoracic, abdominal,<br />
head/neck, and vascular surgeries, patients who had prior<br />
CABG had lower risk of death and MI in the 30 days after the<br />
noncardiac surgery. The benefit of preoperative CABG was<br />
greatest in patients who had multivessel disease and more<br />
severe angina. Similar benefits of preoperative revascularization<br />
were also demonstrated in the BARI [50] trial as well as<br />
an analysis of Medicare patients conducted by Fleisher et al<br />
[51]. However, a major limitation of these studies is their failure<br />
to incorporate risks of CABG and/or delaying noncardiac<br />
surgery into the equation. As a result, decision analyses were<br />
published to address these risks as well as longterm benefits<br />
of CABG. Most authors recommend that preoperative CABG<br />
should only be per<strong>for</strong>med if it is necessary based on indications<br />
independent of the noncardiac surgery [52,53].<br />
Early studies of preoperative percutaneous coronary intervention<br />
(PCI) were limited by small sample size, retrospective<br />
analysis, lack of adequate comparison groups, and variable<br />
timing between PCI and noncardiac surgery [54–59]. Posner<br />
et al [60] found a benefit from preoperative balloon angioplasty<br />
only if it was per<strong>for</strong>med more than 90 days prior to<br />
noncardiac surgery. After balloon angioplasty, delaying noncardiac<br />
surgery <strong>for</strong> more than 8 weeks increases the chance of<br />
restenosis. However, at least 2 weeks is required to allow <strong>for</strong><br />
vessel healing after angioplasty.<br />
The CARP trial [29] was the first multicenter RCT addressing<br />
the issue of preoperative revascularization. Using<br />
a cohort of 5859 VA patients, McFalls et al [29] randomly assigned<br />
510 vascular surgery patients with stable CAD to ei<br />
clinical review<br />
ther revascularization or medical therapy. Of note, researchers<br />
excluded patients requiring emergent/urgent surgery as<br />
well as patients with unstable coronary syndromes, at least<br />
50% left main stenosis, LV ejection fraction less than 20%,<br />
or severe aortic stenosis. There was no difference between<br />
groups in death or nonfatal MI at 30 days and 2.7 years<br />
after noncardiac surgery. The CARP trial was criticized <strong>for</strong><br />
excluding highestrisk patients.<br />
The DECREASE V pilot study [61] attempted to address<br />
the highestrisk group of patients, who were underrepresented<br />
in the CARP trial. This study randomized 101 highrisk<br />
vascular surgery patients who had extensive ischemia<br />
on noninvasive testing. Most patients had 3vessel CAD and<br />
nearly half had ejection fractions less than 35%. At 1 month<br />
and 1 year after noncardiac surgery, there was no evidence<br />
of improved outcomes in patients that been randomized to<br />
preoperative revascularization. It should be noted that both<br />
trials were underpowered and will require further confirmation.<br />
In addition, most patients were on β blockade.<br />
Based on the available evidence, the ACC/AHA guideline<br />
position is that routine prophylactic preoperative revascularization<br />
is not indicated in patients with stable CAD.<br />
Management of surgical patients with prior stents is of<br />
particular concern, especially with the advent of drugeluting<br />
stents. Stenting causes the denudation of arterial endothelial<br />
surface and subsequent risk of thrombosis. This risk of<br />
thrombosis is particularly high <strong>for</strong> the first several weeks<br />
after the intervention. Although oral antiplatelet therapy<br />
counteracts the risk of thrombosis, perioperative bleeding<br />
associated with these agents has led to postponement of noncardiac<br />
procedures until therapy is completed. Drugeluting<br />
stents, compared with baremetal stents, may prolong the reendothelialization<br />
process, causing an even longer delay.<br />
Early retrospective studies of patients with baremetal<br />
stents [62,63] showed that perioperative complications occur<br />
mainly when the noncardiac surgery occurs within 6 weeks<br />
of the PCI. In these studies, thrombosis increased when antiplatelet<br />
agents were prematurely discontinued. Conversely,<br />
bleeding rates were higher if antiplatelet agents were continued<br />
through surgery. Subsequent studies that included<br />
patients with drugeluting stents [64,65] revealed higher<br />
rates of cardiac complications in patients that underwent<br />
noncardiac surgery within the time recommended <strong>for</strong> antiplatelet<br />
therapy compared with those in whom surgery was<br />
delayed. The risk of thrombosis was high even if antiplatelet<br />
therapy was not interrupted.<br />
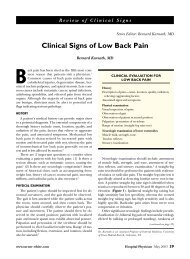
The optimum time required between PCI with stents<br />
and noncardiac surgery is unknown. Recommendations are<br />
oulined in Figure 2. The ACC/AHA [66] currently recommends<br />
that antiplatelet therapy be continued <strong>for</strong> 2 weeks<br />
<strong>for</strong> balloon angioplasty, 4 to 6 weeks <strong>for</strong> baremetal stents,<br />
and 1 year <strong>for</strong> drugeluting stents but recognizes that this<br />
www.turner-white.com Vol. 16, No. 6 June 2009 JCOM 277
PreoPerative cardiac evaluation<br />
Time<br />
since<br />
PCI<br />
< 14 days<br />
Delay <strong>for</strong> elective or<br />
nonurgent surgery<br />
Balloon<br />
angioplasty<br />
> 14 days<br />
Proceed to the operating<br />
room with aspirin<br />
Figure 2. Management of patients with previous percutaneous coronary intervention (PCI). (Adapted from reference 6.)<br />
is arbitrary due to lack of highquality evidence. There is<br />
no evidence that anticoagulants will reduce risk of stent<br />
thrombosis after discontinuation of antiplatelet therapy.<br />
Additional risk factors <strong>for</strong> thrombosis need to be balanced<br />
against risk of bleeding [67]. If a nonsurgical procedure is<br />
planned prior to PCI, balloon angioplasty and baremetal<br />
stents should be used instead of drugeluting stents. However,<br />
at a time where prophylactic preoperative revascularization<br />
is no longer favored, the more common scenario<br />
occurs when the recently stented patients find out that they<br />
need noncardiac surgery.<br />
conclusion<br />
Despite advances in clinical outcomes research over the past<br />
few decades, preoperative cardiac risk assessment and reduction<br />
remains an area of controversy. The most recent update<br />
of the ACC/AHA guidelines places emphasis on modern risk<br />
assessment and medical management techniques rather than<br />
routine and universal noninvasive testing. A notable change<br />
in the guidelines reflects recent evidence that intermediaterisk<br />
patients might not benefit from prophylactic preoperative<br />
revascularization. However, the current studies lack sufficient<br />
power, especially with respect to the highestrisk patients.<br />
Also, the updated guidelines do not include data from the<br />
POISE trial, the results of which call into question the routine<br />
initiation of prophylactic preoperative β blockers. POISE also<br />
questioned whether the RCRI is sufficient <strong>for</strong> risk stratification.<br />
Future research is needed to identify subgroups of<br />
patients who will benefit from preoperative revascularization<br />
and/or β blockade. The type, dose, and timing of β blockade<br />
need to be clarified, and further trials concerning preoperative<br />
statins are needed. Until then, the ACC/AHA guidelines<br />
should be used as a framework rather than an algorithm. An<br />
individualized multidisciplinary approach and riskbenefit<br />
discussion with each patient is the most prudent path to ensuring<br />
success.<br />
Previous PCI<br />
Bare-metal<br />
stent<br />
Delay <strong>for</strong> elective or<br />
nonurgent surgery<br />
Corresponding author: Bizath S. Taqui, MD, Section of General Internal<br />
Medicine, Temple University School of Medicine, Jones Hall, 1316 W.<br />
Ontario St., Philadelphia, PA 19140.<br />
Financial disclosures: None.<br />
Drug-eluting<br />
stent<br />
> 30–45 days < 30–45 days < 365 days<br />
> 365 days<br />
Proceed to the operating<br />
room with aspirin<br />
references<br />
1. Becker RC, Underwood DA. Myocardial infarction in patients<br />
undergoing noncardiac surgery. Cleve Clin J Med 1987;54:25–8.<br />
2. Ashton CM, Petersen NJ, Wray NP, et al The incidence of<br />
perioperative myocardial infarction in men undergoing noncardiac<br />
surgery. Ann Intern Med 1993;118:504–10.<br />
3. Eagle KA, Rihal CS, Mickel MC, et al <strong>Cardiac</strong> risk of noncardiac<br />
surgery: influence of coronary disease and type of<br />
surgery in 3368 operations. CASS Investigators and University<br />
of Michigan Heart Care Program. Coronary Artery <strong>Surgery</strong><br />
Study. Circulation 1997;96:1882–7.<br />
4. Guidelines <strong>for</strong> assessing and managing the perioperative risk<br />
from coronary artery disease associated with major noncardiac<br />
surgery. American College of Physicians. Ann Intern Med<br />
1997;127:309–12.<br />
5. Eagle KA, Berger PB, Calkins H, et al; American College of<br />
Cardiology; American Heart Association. ACC/AHA guideline<br />
update <strong>for</strong> perioperative cardiovascular evaluation <strong>for</strong><br />
noncardiac surgeryexecutive summary: a report of the American<br />
College of Cardiology/American Heart Association Task<br />
Force on Practice Guidelines (Committee to Update the 1996<br />
Guidelines on Perioperative Cardiovascular <strong>Evaluation</strong> <strong>for</strong><br />
<strong>Noncardiac</strong> <strong>Surgery</strong>). J Am Coll Cardiol 2002;39:542–53.<br />
6. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA guidelines<br />
on perioperative cardiac evaluation and care <strong>for</strong> noncardiac<br />
surgery: a report of the ACC/AHA Task Force on Practice<br />
Guidelines. Developed in collaboration with the American<br />
Society of Echocardiography, American Society of Nuclear<br />
Cardiology, Heart Rhythm Society, Society of Cardiovascular<br />
Anesthesiologists, Society <strong>for</strong> Cardiovascular Angiography<br />
and Interventions, Society <strong>for</strong> Vascular Medicine and Biology,<br />
and Society <strong>for</strong> Vascular <strong>Surgery</strong> [published errata appear in<br />
J Am Coll Cardiol 2007;50:e242 and 2008;52:793–4]. J Am Coll<br />
278 JCOM June 2009 Vol. 16, No. 6 www.turner-white.com
Cardiol 2007;50:1707–32.<br />
7. Thygesen K, Alpert JS, White HD; the Joint ESC/ACCF/<br />
AHA/WHF Task Force <strong>for</strong> the Redefinition of Myocardial<br />
Infarction. Universal definition of myocardial infarction. Circulation<br />
2007;116:2634–53.<br />
8. Adesanya AO, de Lemos JA, Greilich NB, Whitten CW. Management<br />
of perioperative myocardial infarction in noncardiac<br />
surgery patients. Chest 2006;130:584–96.<br />
9. Landesberg G, Mosseri M, Zahger D, et al. Myocardial infarction<br />
following vascular surgery: the role of prolonged, stressinduced,<br />
ST depression–type ischemia. J Am Coll Cardiol 2001;<br />
37:1839–45.<br />
10. Devereaux PJ, Goldman L, Yusuf S, et al. Surveillance and<br />
prevention of major perioperative ischemic cardiac events in<br />
patients undergoing noncardiac surgery: a review. CMAJ 2005;<br />
173:779–88.<br />
11. Mangano DT, Browner WS, Hollenberg M, et al. Association<br />
of perioperative myocardial ischemia with cardiac morbidity<br />
and mortality in men undergoing noncardiac surgery. The<br />
Study of Perioperative Ischemia Research Group. N Engl J Med<br />
1990;323:1781–8.<br />
12. Mangano DT, Browner WS, Hollenberg M, et al. Longterm cardiac<br />
prognosis following noncardiac surgery. The Study of Perioperative<br />
Ischemia Research Group. JAMA 1992;268:233–9.<br />
13. Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial<br />
index of cardiac risk in noncardiac surgical procedures. N Engl<br />
J Med 1977;297:845–50.<br />
14. Zeldin RA. Assessing cardiac risk in patients who undergo<br />
noncardiac surgery procedures. Can J Surg 1984;27:402–4.<br />
15. Jeffrey C, Kunsman J, Cullen DJ, Brewster DC. A prospective<br />
evaluation of cardiac risk index. Anesthesiology 1983;58:<br />
462–4.<br />
16. Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting<br />
cardiac complications in patients undergoing noncardiac<br />
surgery. J Gen Intern Med 1986;1:211–9.<br />
17. Eagle KA, Coley CM, Newell JB, et al. Combining clinical<br />
and thallium data optimizes preoperative assessment of cardiac<br />
risk be<strong>for</strong>e major vascular surgery. Ann Intern Med 1989;<br />
110:859–66.<br />
18. Vanzetto G, Machecourt J, Blendea D, et al. Additive value<br />
of thallium singlephoton emission computed tomography<br />
myocardial imaging <strong>for</strong> prediction of perioperative events in<br />
clinically selected high cardiac risk patients having abdominal<br />
aortic surgery. Am J Cardiol 1996;77:143–8.<br />
19. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation<br />
and prospective validation of a simple index <strong>for</strong> prediction<br />
of cardiac risk of major noncardiac surgery. Circulation 1999;<br />
100:1043–9.<br />
20. Boersma E, Poldermans D, Bax JJ, et al; DECREASE Study<br />
Group (Dutch Echocardiographic <strong>Cardiac</strong> Risk <strong>Evaluation</strong><br />
Applying Stress Echocardiography). Predictors of cardiac<br />
events after major vascular surgery: role of clinical characteristics,<br />
dobutamine echocardiography, and betablocker therapy.<br />
JAMA 2001;285:1865–73.<br />
21. Mangano DT, Goldman L. <strong>Preoperative</strong> assessment of patients<br />
with known or suspected coronary disease. N Engl J Med 1995;<br />
333:1750–6.<br />
clinical review<br />
22. Khuri SF, Daley J, Henderson W, et al. The Department of<br />
Veterans Affairs’ NSQIP: the first national, validated, outcomebased,<br />
riskadjusted, and peercontrolled program <strong>for</strong> the<br />
measurement and enhancement of the quality of surgical care.<br />
National VA Surgical Quality Improvement Program. Ann<br />
Surg 1998;228:491–507<br />
23. Kertai MD, Boersma E, Bax JJ, et al. A metaanalysis comparing<br />
the prognostic accuracy of six diagnostic tests <strong>for</strong> predicting<br />
perioperative cardiac risk in patients undergoing major vascular<br />
surgery. Heart 2003;89:1327–34.<br />
24. Mondillo S, Ballo P, Agricola E, et al. Noninvasive tests <strong>for</strong> risk<br />
stratification in major vascular surgery. Vasa 2002;31:195–201.<br />
25. Cohn SL, Goldman L. <strong>Preoperative</strong> risk evaluation and perioperative<br />
management of patients with coronary artery disease.<br />
Med Clin North Am 2003;87:111–36.<br />
26. Beattie WS, Abdelnaem E, Wijeysundera DN, Buckley DN.<br />
A metaanalytic comparison of preoperative stress echocardiography<br />
and nuclear scintigraphy imaging. Anesth Analg<br />
2006;102:8–16.<br />
27. Shaw LJ, Eagle KA, Gersh BJ, Miller DD. Metaanalysis of intravenous<br />
dipyridamolethallium201 imaging (1985 to 1994) and<br />
dobutamine echocardiography (1991 to 1994) <strong>for</strong> risk stratification<br />
be<strong>for</strong>e vascular surgery. J Am Coll Cardiol 1996;27:787–98.<br />
28. Etchells E, Meade M, Tomlinson G, Cook D. Semiquantitative<br />
dipyridamole myocardial stress perfusion imaging <strong>for</strong> cardiac<br />
risk assessment be<strong>for</strong>e noncardiac vascular surgery: a metaanalysis.<br />
J Vasc Surg 2002;36:534–40.<br />
29. McFalls EO, Ward HB, Moritz TE, et al. Coronaryartery revascularization<br />
be<strong>for</strong>e elective major vascular surgery. N Engl<br />
J Med 2004;351:2795–804.<br />
30. Poldermans D, Bax JJ, Schouten O, et al; Dutch Echocardiographic<br />
<strong>Cardiac</strong> Risk <strong>Evaluation</strong> Applying Stress Echo Study<br />
Group. Should major vascular surgery be delayed because<br />
of preoperative cardiac testing in intermediaterisk patients<br />
receiving betablocker therapy with tight heart rate control?<br />
J Am Coll Cardiol 2006;48:964–9.<br />
31. Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol<br />
on mortality and cardiovascular morbidity after noncardiac<br />
surgery. Multicenter Study of Perioperative Ischemia Research<br />
Group [published correction appears in N Engl J Med 1997;<br />
336:1039]. N Engl J Med 1996;335:1713–20.<br />
32. Poldermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol<br />
on perioperative mortality and myocardial infarction in highrisk<br />
patients undergoing vascular surgery. Dutch Echocardiographic<br />
<strong>Cardiac</strong> Risk <strong>Evaluation</strong> Applying Stress Echocardiography<br />
Study Group. N Engl J Med 1999;341:1789–94.<br />
33. Lindenauer PK, Pekow P, Wang K, et al. Perioperative betablocker<br />
therapy and mortality after major noncardiac surgery.<br />
N Engl J Med 2005;353:349–61.<br />
34. Brady AR, Gibbs JS, Greenhalgh RM, et al; POBBLE trial investigators.<br />
Perioperative betablockade (POBBLE) <strong>for</strong> patients<br />
undergoing infrarenal vascular surgery: results of a randomized<br />
doubleblind controlled trial. J Vasc Surg 2005;41:602–9.<br />
35. Yang H, Raymer K, Butler R, et al. The effects of perioperative<br />
betablockade: results of the Metoprolol after Vascular <strong>Surgery</strong><br />
(MaVS) study, a randomized controlled trial. Am Heart J 2006;<br />
152:983–90.<br />
www.turner-white.com Vol. 16, No. 6 June 2009 JCOM 279
PreoPerative cardiac evaluation<br />
36. Juul AB, Wetterslev J, Gluud C, et al; DIPOM Trial Group.<br />
Effect of perioperative beta blockade in patients with diabetes<br />
undergoing major noncardiac surgery: randomised placebo<br />
controlled, blinded multicentre trial. BMJ 2006;332:1482.<br />
37. Redelmeier D, Scales D, Kopp A. Beta blockers <strong>for</strong> elective<br />
surgery in elderly patients: population based, retrospective<br />
cohort study. BMJ 2005;331:932.<br />
38. Auerbach AD, Goldman L. Beta blockers and reduction of<br />
cardiac events in noncardiac surgery: scientific review. JAMA<br />
2002;287:1435–44.<br />
39. Stevens RD, Burri H, Tramer MR. Pharmacologic myocardial<br />
protection in patients undergoing noncardiac surgery: a quantitative<br />
systematic review. Anesth Analg 2003;97:623–33.<br />
40. Devereaux PJ, Beattie WS, Choi PT, et al. How strong is the evidence<br />
<strong>for</strong> the use of perioperative beta blockers in noncardiac<br />
surgery? Systematic review and metaanalysis of randomised<br />
controlled trials. BMJ 2005;331:313–21.<br />
41. McGory ML, Maggard MA, Ko CY. A metaanalysis of perioperative<br />
beta blockade: what is the actual risk reduction?<br />
<strong>Surgery</strong> 2005;138:171–9.<br />
42. POISE Study Group, Devereaux PJ, Yang H, Yusuf H, et al.<br />
Effects of extendedrelease metoprolol succinate in patients<br />
undergoing noncardiac surgery (POISE trial): a randomized<br />
controlled trial. Lancet 2008;371:1839–47.<br />
43. O’NeilCallahan K, Katsimaglis G, Tepper MR, et al. Statins decrease<br />
perioperative cardiac complications in patients undergoing<br />
noncardiac vascular surgery: the Statins <strong>for</strong> Risk Reduction<br />
in <strong>Surgery</strong> (StaRRS) study. J Am Coll Cardiol 2005;45:336–42.<br />
44. McGirt MJ, Perler BA, Brooke BS, et al. 3hydroxy3methylglutaryl<br />
coenzyme A reductase inhibitors reduce the risk of<br />
perioperative stroke and mortality after carotid endarterectomy.<br />
J Vasc Surg 2005;42:829–36.<br />
45. Durazzo AE, Machado FS, Ikeoka DT, et al. Reduction in cardiovascular<br />
events after vascular surgery with atorvastatin: a<br />
randomized trial. J Vasc Surg 2004;39:967–75.<br />
46. Poldermans D, Bax JJ, Kertai MD, et al. Statins are associated<br />
with a reduced incidence of perioperative mortality in patients<br />
undergoing major noncardiac vascular surgery. Circulation<br />
2003;107:1848–51.<br />
47. Lindenauer PK, Pekow P, Wang K, et al. Lipidlowering<br />
therapy and inhospital mortality following major noncardiac<br />
surgery. JAMA 2004;291:2092–9.<br />
48. Hindler K, Shaw AD, Samuels J, et al. Improved postoperative<br />
outcomes associated with preoperative statin therapy. Anesthesiology<br />
2006;105:1260–72.<br />
49. Kapoor AS, Kanji H, Buckingham J, et al. Strength of evidence<br />
<strong>for</strong> perioperative use of statins to reduce cardiovascular risk:<br />
systematic review of controlled studies. BMJ 2006;333:1149.<br />
50. Hassan SA, Hlatky MA, Boothroyd DB, et al. Outcomes of<br />
noncardiac surgery after coronary bypass surgery or coronary<br />
angioplasty in the Bypass Angioplasty Revascularization Investigation<br />
(BARI). Am J Med 2001;110:260–6.<br />
51. Fleisher LA, Eagle KA, Shaffer T, Anderson GF. Perioperative<br />
and longterm mortality rates after major vascular surgery: the<br />
relationship to preoperative testing in the Medicare population.<br />
Anesth Analg 1999;89:849–55.<br />
52. Fleisher LA, Skolnick ED, Holroyd KJ, Lehmann HP. Coronary<br />
artery revascularization be<strong>for</strong>e abdominal aortic aneurysm surgery:<br />
a decision analytic approach. Anesth Analg 1994;79:661–9.<br />
53. Mason JJ, Owens DK, Harris RA, et al. The role of coronary angiography<br />
and coronary revascularization be<strong>for</strong>e noncardiac<br />
vascular surgery. JAMA 1995;273:1919–25.<br />
54. Allen JR, Helling TS, Hartzler GO. Operative procedures not<br />
involving the heart after percutaneous transluminal coronary<br />
angioplasty. Surg Gynecol Obstet 1991;173:285–8.<br />
55. Huber KC, Evans MA, Bresnahan JF, et al. Outcome of noncardiac<br />
operations in patients with severe coronary artery disease<br />
successfully treated preoperatively with coronary angioplasty.<br />
Mayo Clin Proc 1992;67:15–21.<br />
56. Elmore JR, Hallett JW Jr, Gibbons RJ, et al. Myocardial revascularization<br />
be<strong>for</strong>e abdominal aortic aneurysmorrhaphy: effect<br />
of coronary angioplasty. Mayo Clin Proc 1993;68:637–41.<br />
57. Gottlieb A, Banoub M, Sprung J, et al. Perioperative cardiovascular<br />
morbidity in patients with coronary artery disease undergoing<br />
vascular surgery after percutaneous transluminal coronary<br />
angioplasty. J Cardiothorac Vasc Anesth 1998;12:501–6.<br />
58. Brilakis ES, Or<strong>for</strong>d JL, Fasseas P, et al. Outcome of patients<br />
undergoing balloon angioplasty in the two months prior to<br />
noncardiac surgery. Am J Cardiol 2005;96:512–4.<br />
59. Leibowitz D, Cohen M, Planer D, et al. Comparison of cardiovascular<br />
risk of noncardiac surgery following coronary angioplasty<br />
with versus without stenting. Am J Cardiol 2006;97:<br />
1188–91.<br />
60. Posner KL, Van Norman GA, Chan V. Adverse cardiac outcomes<br />
after noncardiac surgery in patients with prior percutaneous<br />
transluminal coronary angioplasty. Anesth Analg 1999;<br />
89:553–60.<br />
61. Poldermans D, Schouten O, Vidakovic R, et al. A clinical randomized<br />
trial to evaluate the safety of a noninvasive approach<br />
in highrisk patients undergoing major vascular surgery: the<br />
DECREASEV Pilot Study. J Am Coll Cardiol 2007;49:1763–9.<br />
62. Kaluza GL, Joseph J, Lee JR, et al. Catastrophic outcomes of<br />
noncardiac surgery soon after coronary stenting. J Am Coll<br />
Cardiol 2000;35:1288–94.<br />
63. Wilson SH, Fasseas P, Or<strong>for</strong>d JL, et al. Clinical outcome of patients<br />
undergoing noncardiac surgery in the two months following<br />
coronary stenting. J Am Coll Cardiol 2003;42:234–40.<br />
64. Vicenzi MN, Meislitzer T, Heitzinger B, et al. Coronary artery<br />
stenting and noncardiac surgery: a prospective outcome study.<br />
Br J Anaesth 2006;96:686–93.<br />
65. Schouten O, van Domburg RT, Bax JJ, et al. <strong>Noncardiac</strong> surgery<br />
after coronary stenting: early surgery and interruption of<br />
antiplatelet therapy are associated with an increase in major<br />
adverse cardiac events. J Am Coll Cardiol 2007;49:122–4.<br />
66. Grines CL, Bonow RO, Casey DE Jr, et al. Prevention of premature<br />
discontinuation of dual antiplatelet therapy in patients<br />
with coronary artery stents: a science advisory from the<br />
American Heart Association, American College of Cardiology,<br />
Society <strong>for</strong> Cardiovascular Angiography and Interventions,<br />
American College of Surgeons, and American Dental Association,<br />
with representation from the American College of Physicians.<br />
Circulation 2007;115:813–8.<br />
67. Riddell JW, Chiche L, Plaud B et al. Coronary stents and noncardiac<br />
surgery. Circulation 2007;116:e378–82.<br />
Copyright 2009 by Turner White Communications Inc., Wayne, PA. All rights reserved.<br />
280 JCOM June 2009 Vol. 16, No. 6 www.turner-white.com