

Anatomy and histology of the denture bearing area - Dentistry ...
Anatomy and histology of the denture bearing area - Dentistry ...
Anatomy and histology of the denture bearing area - Dentistry ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Anatomy</strong> <strong>and</strong> <strong>histology</strong><br />
<strong>of</strong> <strong>the</strong> <strong>denture</strong> <strong>bearing</strong> <strong>area</strong><br />
Dr. Aylin BAYSAN<br />
The University <strong>of</strong> Birmingham<br />
School <strong>of</strong> <strong>Dentistry</strong><br />
<strong>Anatomy</strong> <strong>of</strong> <strong>the</strong> edentulous <strong>area</strong><br />
O<strong>the</strong>r structures should also be identified to<br />
establish <strong>the</strong>ir precise relation to <strong>denture</strong><br />
base. These are as follows:<br />
• Ligaments<br />
• Frenulum<br />
• Gl<strong>and</strong>ular tissues<br />
Lower jaw<br />
• Labial frenulum<br />
It is a fold <strong>of</strong> fibrous tissue in <strong>the</strong> midline between<br />
lip <strong>and</strong> alveolus.<br />
• Mentalis muscle<br />
This muscle arises from <strong>the</strong> symphysis menti <strong>and</strong><br />
is inserted downward into skin <strong>of</strong> <strong>the</strong> chin.<br />
It elevates <strong>the</strong> lower lip <strong>and</strong> may lift up <strong>the</strong> lower<br />
<strong>denture</strong>.<br />
<strong>Anatomy</strong> <strong>of</strong> <strong>the</strong> edentulous <strong>area</strong><br />
In <strong>the</strong> mouth, complete or partial <strong>denture</strong>s are<br />
surrounded by muscles.<br />
Muscles tend to distabilise <strong>the</strong> <strong>denture</strong> if <strong>the</strong>y<br />
are encroached upon during contraction.<br />
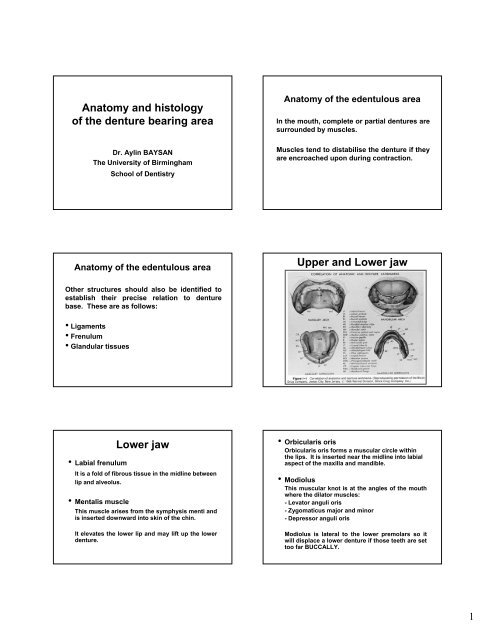
Upper <strong>and</strong> Lower jaw<br />
• Orbicularis oris<br />
Orbicularis oris forms a muscular circle within<br />
<strong>the</strong> lips. It is inserted near <strong>the</strong> midline into labial<br />
aspect <strong>of</strong> <strong>the</strong> maxilla <strong>and</strong> m<strong>and</strong>ible.<br />
• Modiolus<br />
This muscular knot is at <strong>the</strong> angles <strong>of</strong> <strong>the</strong> mouth<br />
where <strong>the</strong> dilator muscles:<br />
- Levator anguli oris<br />
- Zygomaticus major <strong>and</strong> minor<br />
- Depressor anguli oris<br />
Modiolus is lateral to <strong>the</strong> lower premolars so it<br />
will displace a lower <strong>denture</strong> if those teeth are set<br />
too far BUCCALLY.<br />
1
Muscles <strong>of</strong> facial expression which form modiolus<br />
• Buccinator muscle<br />
It arises from both jaws opposite <strong>the</strong> molar<br />
alveolar <strong>area</strong> <strong>and</strong> posteriorly from <strong>the</strong><br />
pterygom<strong>and</strong>ibular raphé.<br />
As <strong>the</strong> buccinator fibres run almost parallel to <strong>the</strong><br />
<strong>denture</strong> border, <strong>the</strong>y can slightly be displaced for<br />
additional retention.<br />
In this respect, it is <strong>the</strong> UNIQUE <strong>and</strong> ONLY<br />
muscle that can be used this way.<br />
Denture <strong>bearing</strong> <strong>area</strong><br />
• Mental nerve<br />
This nerve emerges from <strong>the</strong> mental foramen near<br />
<strong>the</strong> apices <strong>of</strong> <strong>the</strong> lower premolars.<br />
In patients with extreme alveolar resorption, <strong>the</strong><br />
nerve may lie on or near <strong>the</strong> crest <strong>of</strong> <strong>the</strong> alveolar<br />
ridge.<br />
Pain or paraes<strong>the</strong>sia may be experienced if <strong>the</strong><br />
nerve is trapped by a <strong>denture</strong> base, usually by <strong>the</strong><br />
fitting surface.<br />
• Massater muscle<br />
This muscle is <strong>the</strong> MOST powerful <strong>of</strong> <strong>the</strong><br />
muscles which close <strong>the</strong> MANDIBLE.<br />
The lower <strong>denture</strong> periphery related to it<br />
should be shaped according to its<br />
structure so that displacement <strong>of</strong> <strong>the</strong><br />
<strong>denture</strong> can be avoided when <strong>the</strong> muscle<br />
contracts.<br />
• Anterior fibres <strong>of</strong> temporalis<br />
These fibres are sometimes attached low<br />
down on <strong>the</strong> anterior border <strong>of</strong> <strong>the</strong> ramus<br />
as far as <strong>the</strong> attachment <strong>of</strong> <strong>the</strong> buccinator<br />
in <strong>the</strong> retromolar fossa.<br />
The contraction <strong>of</strong> <strong>the</strong>se fibres may<br />
sometimes displace a lower <strong>denture</strong>.<br />
2
• Retromolar pad<br />
Retromolar pad lies distal to <strong>the</strong> lower third molar<br />
<strong>and</strong> is composed <strong>of</strong> fibrous tissue <strong>and</strong> mucous<br />
gl<strong>and</strong>s.<br />
• Superior constrictor muscle<br />
This muscle originates from <strong>the</strong> pterygom<strong>and</strong>ibular<br />
raphé with a small extension continuing on <strong>the</strong><br />
lingual surface <strong>of</strong> <strong>the</strong> m<strong>and</strong>ible to <strong>the</strong> posterior end<br />
<strong>of</strong> <strong>the</strong> mylohyoid line.<br />
• Genioglossus muscle <strong>and</strong> genial tubercle<br />
The genioglossus arises from <strong>the</strong> superior genial<br />
tubercles on <strong>the</strong> lingual surface <strong>of</strong> <strong>the</strong> m<strong>and</strong>ible.<br />
When <strong>the</strong> tongue is protruded, this muscle may lift<br />
<strong>the</strong> lower <strong>denture</strong>.<br />
When <strong>the</strong> edentulous m<strong>and</strong>ible is severely<br />
resorbed, <strong>the</strong> superior genial tubercle may project<br />
above <strong>the</strong> level <strong>of</strong> <strong>the</strong> alveolar ridge <strong>and</strong> <strong>the</strong><br />
mucosa may become traumatised by a lower<br />
<strong>denture</strong>.<br />
Muscles limiting <strong>the</strong> extension <strong>of</strong><br />
a lower <strong>denture</strong><br />
• Lingually<br />
The posterior extension is limited by fibers<br />
from <strong>the</strong> superior constrictor muscle.<br />
Fibres from <strong>the</strong> palatoglossus also form a<br />
posterior limit.<br />
The depth <strong>of</strong> <strong>the</strong> lingual flange is governed<br />
by <strong>the</strong> mylohyoid.<br />
• Mylohyoid muscle<br />
It is a thin sheet <strong>of</strong> muscle <strong>and</strong> forms <strong>the</strong> floor <strong>of</strong><br />
<strong>the</strong> mouth. Its linear origin from <strong>the</strong> mylohyoid line<br />
<strong>of</strong> <strong>the</strong> m<strong>and</strong>ible continues posteriorly to <strong>the</strong> level <strong>of</strong><br />
<strong>the</strong> third molar.<br />
• Sublingual salivary gl<strong>and</strong><br />
This gl<strong>and</strong> rests on <strong>the</strong> mylohyoid muscle medial to<br />
<strong>the</strong> m<strong>and</strong>ible. It is usually adjacent to <strong>the</strong> lower<br />
canine region.<br />
Its indentation is <strong>of</strong>ten seen on lower impressions<br />
Muscles limiting <strong>the</strong> extension <strong>of</strong><br />
a lower <strong>denture</strong><br />
• Anterior labial flange<br />
Orbicularis oris as far as <strong>the</strong> first premolar<br />
region.<br />
• Buccally<br />
Buccinator muscle<br />
• Retromolar pad<br />
Buccinator <strong>and</strong> its insertion into <strong>the</strong><br />
pterygom<strong>and</strong>ibular raphé.<br />
Upper jaw<br />
• Coronoid process<br />
Coronoid process lies lateral to <strong>the</strong> maxillary<br />
tuberosity.<br />
It may sometimes impinge on <strong>the</strong> buccal flange <strong>of</strong><br />
a <strong>denture</strong> <strong>and</strong> cause pain or instability.<br />
• Hamular notch<br />
This notch is <strong>the</strong> junction <strong>of</strong> <strong>the</strong> maxillary<br />
tuberosity <strong>and</strong> hamular process.<br />
The periphery <strong>of</strong> a correctly extended <strong>denture</strong><br />
should extend through <strong>the</strong>se notches via <strong>the</strong> <strong>area</strong><br />
<strong>of</strong> <strong>the</strong> fovea palatinae.<br />
3
• Fovea palatinae<br />
These are a pair <strong>of</strong> mucous gl<strong>and</strong> duct orifices<br />
near <strong>the</strong> midline at <strong>the</strong> junction <strong>of</strong> <strong>the</strong> hard <strong>and</strong><br />
s<strong>of</strong>t palate.<br />
These l<strong>and</strong>marks provide a guide to <strong>the</strong> position<br />
<strong>of</strong> <strong>the</strong> posterior palatal border <strong>of</strong> a <strong>denture</strong>.<br />
• Incisive papilla<br />
Incisive papilla is a mass <strong>of</strong> fibrous tissue about 1<br />
cm behind <strong>the</strong> upper incisors.<br />
Its position in <strong>the</strong> edentulous mouth indicates<br />
where <strong>the</strong> incisors <strong>and</strong> canines should be set.<br />
Facial curtain<br />
The orbicularis oris <strong>and</strong> buccinator muscles<br />
are draped around <strong>the</strong> mouth to form a<br />
curtain, which is supported by teeth <strong>and</strong><br />
alveoli.<br />
In edentulous patients, this curtain collapses<br />
to give <strong>the</strong> characteristic toothless look.<br />
Maxilla <strong>and</strong> m<strong>and</strong>ible<br />
There is difference in resorption pattern for<br />
maxilla <strong>and</strong> m<strong>and</strong>ible.<br />
This leads to <strong>the</strong> appearance <strong>of</strong> prognatism<br />
<strong>and</strong> gross positional discrepancies between<br />
opposing residual ridges.<br />
Muscles limiting <strong>the</strong> extension <strong>of</strong><br />
a upper <strong>denture</strong><br />
• Anterior labial flange<br />
Anterior labial flange is limited by <strong>the</strong><br />
orbicularis oris as far as <strong>the</strong> first premolar<br />
region.<br />
• Buccally<br />
From <strong>the</strong> second premolar region<br />
posteriorly, <strong>the</strong> buccal flange is limited by<br />
<strong>the</strong> buccinator.<br />
Collapse <strong>of</strong> elevator <strong>and</strong> depressor muscles<br />
<strong>and</strong> modiolus following loss <strong>of</strong> teeth<br />
Edentulous face<br />
4
Muscles attachment changes with<br />
progressive bone loss<br />
The varying thickness <strong>of</strong> <strong>the</strong> mucosa<br />
covering <strong>the</strong> oral cavity<br />
Tongue<br />
The tongue is highly mobile muscular organ<br />
that needs careful attention during <strong>the</strong><br />
construction <strong>of</strong> complete <strong>denture</strong>s.<br />
In coordination with lips, cheek, palate <strong>and</strong><br />
pharynx, <strong>the</strong> tongue functions in speech,<br />
mastication <strong>and</strong> swallowing.<br />
Oral mucous membrane<br />
• Oral cavity<br />
Stratified squamous type <strong>and</strong> shows differences in<br />
degree <strong>of</strong> development, which correlates with <strong>the</strong><br />
functions <strong>of</strong> a particular <strong>area</strong>.<br />
Apart from systemic that affect <strong>the</strong> integrity <strong>of</strong> <strong>the</strong><br />
oral mucous membrane, it should be noted that <strong>the</strong>re<br />
are age changes that are frequently seen in <strong>the</strong><br />
elderly edentulous patient including tendency to<br />
dryness <strong>and</strong> general atrophy <strong>of</strong> <strong>the</strong> mucous<br />
membrane.<br />
Oral mucosa<br />
Tongue<br />
The tongue is in intimate contact with a<br />
complete lower <strong>denture</strong> <strong>and</strong> its position in<br />
relation to an edentulous ridge varies widely.<br />
This relationship must be considered very<br />
carefully in each particular patient.<br />
5
Salivary gl<strong>and</strong>s<br />
Saliva is derived from <strong>the</strong> major <strong>and</strong> minor<br />
salivary gl<strong>and</strong>s. The major salivary gl<strong>and</strong>s<br />
consist <strong>of</strong> three pairs <strong>of</strong> gl<strong>and</strong>s:<br />
• Parotid Gl<strong>and</strong><br />
• Subm<strong>and</strong>ibular Gl<strong>and</strong><br />
• Sublingual Gl<strong>and</strong><br />
The outline <strong>of</strong> <strong>the</strong> lingual flange <strong>of</strong> <strong>the</strong> lower<br />
<strong>denture</strong> in relation to subm<strong>and</strong>ibular gl<strong>and</strong><br />
• Subm<strong>and</strong>ibular Gl<strong>and</strong><br />
Extension <strong>of</strong> <strong>the</strong> lingual flange <strong>of</strong> a <strong>denture</strong> in<br />
this region can lead to obstruction <strong>of</strong> <strong>the</strong><br />
subm<strong>and</strong>ibular gl<strong>and</strong>.<br />
Patients may complain <strong>of</strong> developing<br />
swellings under <strong>the</strong> jaws when eating.<br />
6
