
You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
1<br />
<strong>Dr</strong>. <strong>Dan</strong> <strong>Regev</strong><br />
Plastic Surgery Department<br />
Rabin Medical Center
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
2<br />
BACKGROUND<br />
•Forearm fractures- common limb fractures<br />
•Upper, middle, lower shaft<br />
MECHANISM OF INJURY<br />
•Direct blow: fall + hyperextension / flexion<br />
•Compression, shearing forces & avulsion<br />
EPIDEMIOLOGY (USA)<br />
•Upper limb fractures = 50% overall<br />
•Forearm fractures = 1/3 of upper limb (distal = 17%)<br />
2mm<br />
Radiio-ulnar<br />
inclination<br />
20%<br />
80%<br />
axial load<br />
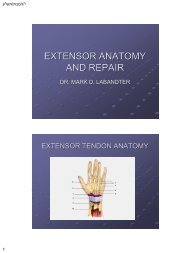
ANATOMY<br />
23º radial inclination<br />
11º (lateral view)<br />
anteversion<br />
Epiphysis with slits<br />
Metaphysis spongiotic<br />
Thin cortices<br />
BIARTICULAR<br />
Scaphoid<br />
fossa<br />
Lunate<br />
fossa<br />
BICONCAVE
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
3<br />
EPIDEMIOLOGY<br />
•Gender: Infants 2y boys<br />
Adults women (osteoporosis)<br />
•Race: less in blacks (less osteoporosis)<br />
CAUSES<br />
•Sports: skating, skateboarding, mountain<br />
biking and contact sports<br />
•Trauma: automobile collisions, blows with a<br />
blunt object and child abuse<br />
HISTORY<br />
•Direct blow usually<br />
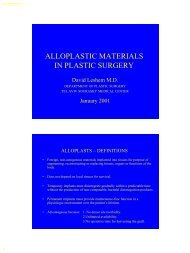
PHYSICAL EXAMINATION<br />
•Local pain, tenderness,<br />
swelling<br />
•Any wound over the<br />
fracture = open fracture<br />
(2 nd most common after<br />
open tibial fractures)<br />
Smith open fractures classification<br />
I<br />
II<br />
III<br />
IIIa<br />
IIIb<br />
Type Description<br />
Clean wound<br />
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
4<br />
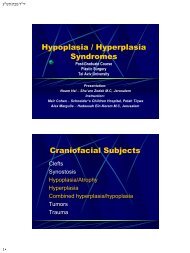
NEUROLOGICAL EVALUATION<br />
TPD / MTPD<br />
5mm - OK<br />
Ulnar<br />
sensory<br />
Radial<br />
sensory<br />
Median<br />
ensory<br />
*Misleading:<br />
muscle & tendon<br />
entrapment etc.<br />
Radial Ulnar Median<br />
VASCULAR EXAM<br />
Allen test Capillary refilling<br />
test
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
5<br />
PHYSICAL EXAM<br />
Radial head #<br />
Ulnar styloid #<br />
Dorsal ulnar prominence<br />
IMAGING<br />
A-P<br />
Lateral<br />
Oblique<br />
Post operatively<br />
Also (completion)<br />
3D: high velocity (young)<br />
2D: extra articular
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
6<br />
Descriptive (symptomes & Rx):<br />
Castaing, Frykman<br />
Extension-compression:<br />
Type Description<br />
I Colles: 4cm prox. To palm; dorsal<br />
fragmentation, angulation and<br />
displacement + Radius shortening<br />
II Partial = marginals<br />
III T (frontal, saggital)<br />
IV Composite = ex. articular<br />
CLASSIFICATION<br />
CASTAING CLASSIFICATION<br />
Therapeutic:<br />
Universal, Melone
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
7<br />
Flexion-compression:<br />
Type Description<br />
Smith I ex. art. ; palmar angulation<br />
II int. art. ; palmar prox. Displace.<br />
III ex. art. ; palmar displace.<br />
Marginals Palmar = as Smith II<br />
Dorsal = Barton’s<br />
Medial = Die punch<br />
Lateral = Backfire<br />
Extra-articular<br />
Radio-carpal<br />
CASTAING CLASSIFICATION<br />
FRYKMAN CLASSIFICATION<br />
Lunate load #<br />
Axial compression<br />
& Lunate dorsal depression<br />
Radio-ulnar<br />
Radio-carpal-ulnar
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
8<br />
* Die punch<br />
principle<br />
I<br />
II<br />
III<br />
IV<br />
UNIVERSAL CLASSIFICATION<br />
Type Description<br />
Ex. art. , stable, for ex. reduction<br />
Ex. art. , unstable, not for ex. reduct.<br />
Articular, stable<br />
IV a Artic. , stable, for ex. reduction<br />
IV b Artic. , unstable, not for ex. reduct.<br />
* Fracture reducibility<br />
I<br />
MELONE CLASSIFICATION<br />
Type Description<br />
Undisplaced = universal type III<br />
II II a Stable, for external reduction<br />
(50%)<br />
Involved<br />
lunate<br />
III<br />
(5%)<br />
IV<br />
V<br />
(dorsal / palmar compression)<br />
II b Unstable, 15% not for external reduction<br />
(double die punch; fragmented radius)<br />
Articular ant. displacement: neural &<br />
vascular compression, cortical tear<br />
180º rotation of articular fragments<br />
Complicated reduction<br />
Burst of diaphysis-metaphysis-epiphysis<br />
Conservative treatment
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
9<br />
SPECIAL FRACTURES<br />
Galeazzi fracture: # dist. 1/3rd Radius + Dislocation of RadioUlnar Joint<br />
(DRUJ) = “reversed Monteggia” (x3 common)<br />
When DRUJ overlooked – higher morbidity<br />
1) Radius shortening by 5mm<br />
2) # of ulnar styloid<br />
3) Widening DRUJ space by 2mm<br />
- or DRUJ subluxation<br />
* Compare to other wrist; keep exact position!<br />
Essex-Lopresti fracture: # dist. head of Radius + Radioulnar dislocation<br />
with partial / complete tear of radioulnal<br />
interosseous membrane<br />
TREATMENT<br />
Emergency: 1) Neurovascular compromise<br />
2) Severe displacement<br />
3) Tenting of the skin<br />
Principles: 1) Articular anatomy restoration<br />
2) Stability of wrist joint<br />
3) Early mobilization
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
10<br />
1) Closed reduction:<br />
- longitudinal traction<br />
- palmar flexion<br />
- ulnar inclination<br />
METHODS<br />
2) Direct nailing (ORIF):<br />
- lowering consolidation time<br />
and immobilization time (6-8w)<br />
- for radial styloid, posteromedial fragments<br />
and stbilizing the radio-ulna joint (pronosupination)<br />
METHODS<br />
3) Direct osteosynthesis (internal fixation):<br />
- includes special plates and screws<br />
- Anterior / posterior approach (if palmar large<br />
bone loss)<br />
- Can include bone graft (Radius, Iliac crest)<br />
to stabilize fragments<br />
4) External fixation:<br />
- nesscitates preliminar closed reduction<br />
- ligamentotaxis<br />
- duration of 3-8w; if consolidates enough- remove & cast 2w<br />
afterwards mobile cast<br />
- technique: reduction under Rx vision<br />
longitudinal traction -> neutralize articulation<br />
palmar flexion?<br />
mild extension (8º)<br />
Stable fractures<br />
No displacement<br />
CI to surgery<br />
Unstable<br />
Few large<br />
fragments<br />
Unstable<br />
Multiple fragments<br />
Melone V<br />
Unstable<br />
Multiple fragments
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
11<br />
BACKGROUND<br />
•Carpal fractures- only 25% of wrist fractures<br />
•10% of hand injuries<br />
MECHANISM OF INJURY<br />
•Axial compression + wrist hyperextension<br />
(fall with outstretched hand)<br />
EPIDEMIOLOGY<br />
•Common in adolescents<br />
BASIC FUNCTIONS<br />
1) Positioning<br />
2) Regulating forces<br />
3) Transmitting forces<br />
ANATOMY<br />
Metacarpals<br />
Dist. row<br />
Prox. row
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
12<br />
GREATER ARC:<br />
Perilunate carpal bones<br />
LESSER ARC:<br />
Disruption of ligaments<br />
* follows lunate contour<br />
TRADITIONAL<br />
CONCEPT<br />
Two rows<br />
(distal as one unit)<br />
Scaphoid bridging<br />
Between them<br />
VULNERABILITY ZONES<br />
BIOMECHANICAL MODELS<br />
NAVARRO<br />
TALEISNIK<br />
Central = flex.-extens.<br />
(radio-lunate, luno-capitate)<br />
Lateral = radial dev. = volar rot.<br />
ulnar dev. = neutral<br />
Medial = pronation - supination<br />
radial dev. = high pos.<br />
ulnar dev. = low pos.<br />
*Pisiform not included
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
13<br />
BIOMECHANICAL MODELS<br />
LICHTMAN’S OVAL<br />
RING CONCEPT<br />
Two rows = one ring<br />
Scapho-trapezial link<br />
Triquatrio-hamatum link<br />
Any disruption possible<br />
WRIST KINEMATICS<br />
•Wrist joint = three articular<br />
•Proximal row with intracarpal motion (scaphoid – lunate)<br />
•Distal row moves as one unit<br />
•Pisiform does not contribute and not included<br />
FLEXION / EXTENSION<br />
Radio-carpal & mid-carpal joints<br />
Rows angulate<br />
Lunate moves the list; scaphoid – the most<br />
RADIAL & ULNAR DEVIATION<br />
Proximal row rotates in the sggital plane<br />
Distal row angulates radial / ulnar<br />
PRONATION & SUPINATION<br />
Forearm bones function<br />
Pron. - palmar RadioScaphoCapitate Lig.<br />
Supin. - palmar UlnoLunate Lig.<br />
dorsal RadioTriquetral Lig.<br />
WEBER’S VIEW<br />
Radial column – force bearing<br />
Ulnar column – wrist control<br />
(lunate position vs stable capitate)<br />
PALMAR DORSAL<br />
Radial Ulnar deviation<br />
Prox. row – volar dorsiflex. flex.<br />
Dist. row – dorsal volar flex.
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
14<br />
A WORD ABOUT INSTABILITIES..<br />
•Static (per standard Rx) vs. dynamic (per stress views)<br />
•Lunate position: Dorsal / Volar Intercalated Segmental Instability (DISI / VISI)<br />
•Mayfield classification<br />
DISI: 1) scapho-lunate dissociation; most common instability.<br />
*In radial styloid #<br />
disruption of scapholunate, scaphotrapezoid ligs., FCR floor & radiocarpal lig.<br />
Pain & tenderness in snuffbox / dorsal scapholunate joint + clicks<br />
Watson’s test (+ pain)<br />
Rx: scapholunate space >+3mm (Terry-Thomas sign); scaphoid “cortical ring”<br />
*comparison to other wrist<br />
Tx: arthroscopic tear resection, K-wire pinning (3-4w), ligaments repair<br />
& capsulodesis<br />
2) Scaphoid non-union / mal-union: prox. & dist. Fragments move indipendently<br />
Rx: high resolution CT scan<br />
Tx: correct fusion<br />
A WORD ABOUT INSTABILITIES..<br />
VISI: 1) lunotriquetral dissociation; can lead to synovitis, arthrosis & wrist pain<br />
Rx: may be normal (ulnar sided instabilities?)<br />
*L-T lig. Disruption alone cannot produce VISI<br />
Ulnar sided wrist pain motiom limit<br />
Shear test (+ pain)<br />
Tx: immobilization 4-6w inc. elbow, lig. debridement by arthroscopy<br />
2) Radiocarpal dissociation; in rheumatoid arthritis<br />
Compromise of dorsal radiocarpal capsule (inc. radiotriquetral lig.)<br />
OTHERS: 1) Radiocarpal instabilities; dist. Radius # (DISI), arthritis (ulnar)<br />
*Volar subluxation is rare<br />
2) Perilunate fracture-dislocations: in the lesser arc; can include<br />
greater arc and even distal radiolunate joint
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
15<br />
•Most fractured<br />
•In young male adults<br />
•Mechanism: fall, sport injury, MVA<br />
•Isolated / combined with others<br />
•Wrist extension = distal #<br />
Blood supply: distal = distal pole (1/3)<br />
dorsal = proximal 2/3<br />
*prox. Pole – retrograde flow from<br />
vessels distal to waist<br />
(avascular necrosis – bad prognosis)<br />
SCAPHOID FRACTURES<br />
Trapezium<br />
Trapezoid<br />
articulation<br />
History: radial wrist pain post fall with outstretched hand<br />
Examine: pain in snuffbox, mild swelling<br />
Rx: may be without signs (2%); A-P, Lat., oblique x2<br />
compare to other scaphoid, repeat in 10-14d<br />
SCAPHOID FRACTURES CLASSIFICATIONS<br />
Horizontal<br />
oblique<br />
Russe<br />
Stable<br />
Transverse Vertical<br />
oblique<br />
Herbert<br />
&<br />
Fisher<br />
Base<br />
(tubercle)<br />
Waist<br />
Body<br />
Radius<br />
articulation
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
16<br />
Scaphoid fractures<br />
Nonunion: wide # zone, sclerosis (resorption); shortening,<br />
fragments discrepancy, angulation<br />
Delayed union: wide # zone, NO sclerosis (after 4m)<br />
Unstable: 1) displacement + any step-off v>=1mm<br />
2) angulation<br />
3) motion of fracture<br />
4) association with carpal instability<br />
Treatment: 1) Immobilization – stable & non-displaced<br />
* Thumb spica cast – long, for first 6w, short afterwards<br />
2) Internal fixation – unstable # & displaced<br />
3) Bone grafting: only if severe comminution<br />
Preiser’s disease: idiopathic avascular necrosis; ~40y old, steroid usage<br />
Tx: revascularization / resection + prox. Row carpectomy<br />
LUNATE FRACTURES<br />
Possible #: body, palmar / dorsal<br />
Tx: Cast immobilization (6w)<br />
KienbÖck’s disease: avascular necrosis<br />
From repeated trauma; male workers,<br />
18-40y; short ulna; fragmentation-collapse-<br />
-loss of carpal alignment-carpal arthrosis<br />
TRAPEZIUM FRACTURES<br />
Rare<br />
Direct blows<br />
Rx mostly enough<br />
Closed vs. open reduction<br />
TRAPEZOID FRACTURES<br />
The list frequently injured<br />
Dorsal dislocation by palmar<br />
forces on M2<br />
Anatomic reduction + stabilize.<br />
CAPITATE FRACTURES<br />
Rare<br />
Prox. 2/3 (perilunate injuries)<br />
Non-displaced # - immobilize<br />
fragments – open reduction<br />
TRIQUETRIUM FRACTURES<br />
Common<br />
With ligs. & bony damage<br />
Mostly dorsal cortex chip fractures<br />
Tx: immobilize for 4-6w.
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
17<br />
PISIFORM FRACTURES<br />
Rare<br />
Confines FCU<br />
Immobilize (if needed)<br />
HAMATE FRACTURES<br />
Body #; association with other wrist pathology<br />
Hamulus #; seen in golf, squash, tennis;<br />
Deep ulnar pain, aggrevated by activities<br />
Body exam: tenderness over hamate<br />
painful D5 abduction<br />
Internal fiixation<br />
Often progress to non-union<br />
BACKGROUND<br />
•Most common fractures (10% of all fractures)<br />
•In the US more than 16 million per year<br />
MECHANISM OF INJURY<br />
•Different trauma patterns: fist / open hand, with<br />
associated injuries (wounds, foreign bodies)<br />
EPIDEMIOLOGY<br />
•In all age groups<br />
•In small children – suspect abuse
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
18<br />
HISTORY<br />
Trauma pattern: occured in dirty / clean place<br />
associated crush injuries<br />
hand position at injury<br />
high preesure injection<br />
jewelry on fingers<br />
* fist / open hand<br />
* lacerations (over MCP?)<br />
* fist in mouth<br />
Domiant hand and hobbies<br />
Dist. phalanx<br />
Middle phalanx<br />
Prox. phalanx<br />
Metacarpals<br />
ANATOMY<br />
Thumb-Trapezium free articulation<br />
D4-5 with 20-25º of A-P movement<br />
D2-3 with minimal flex.-ex.
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
19<br />
FINGER FRACTURE<br />
Intra / extra articular, stable / unstable<br />
Very precise reduction (rotation error)<br />
Closed reduction if possible (tendons & ligs.)<br />
usually with k-wire<br />
For a cast: alignment ±10º<br />
no rotation error<br />
maintan flex.-ex. Balance<br />
no bone tissue loss<br />
normal finger gross appearance<br />
DISTAL PHALANX FRACTURES<br />
•Common d/t crush injury<br />
•Min. displacement – simple splint<br />
•Damage to fingernail : hematoma, laceration<br />
repair lacerations<br />
*clear fractured surface from nailbed tissue<br />
•In children may be through growth plate<br />
Wide epiphysis
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
20<br />
MIDDLE PHALANX FRACTURES<br />
•Condylar #: closed reduction + k-wire<br />
if open reduction: fine screw<br />
•Shaft #: unstable (FDS)<br />
closed reduction + k-wire + splint<br />
PIPJ #: most serious (volar plate)<br />
bad comminution<br />
closed fixation (trans art. Pins)<br />
early mobilization (after 3-4)<br />
PROXIMAL PHALANX FRACTURES<br />
•Unstable<br />
•Most accurate reduction (intra-articular)<br />
•Shaft # (transverse, oblique) - ant. angulation<br />
•MPJ #: nesscitates + stabilization
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
21<br />
METACARPAL FRACTURES<br />
•Shaft #: oblique shortens, trans. angulates & spiral - rotates<br />
•Goals for reduction:<br />
- No rotational error<br />
- less 3mm shortening<br />
- angulation up to 15º<br />
unstable<br />
- surface contact >50% of all bone fragments<br />
•Usually closed reduction<br />
•Neck #: most common D5 neck #<br />
- Reduction by k-wire<br />
•Head fracture: uncommon; Tx as discussed above.<br />
METACARPAL THUMB FRACTURES<br />
Neck #<br />
Bone loss<br />
•Head & shaft #: stable; k-wire debridement after long. traction<br />
•Angulation
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
22<br />
A WORD ABOUT JOINT DISLOCATIONS..<br />
PIPJ: dorsal dislocation; hyperex.+longitudinal compression<br />
Simplecomplex fracture-dislocation (most unstable)<br />
Simple & complex- immobilization 3-4w<br />
Fracture-dislocation (volar plate tear)- immobilization or<br />
K-wire or even open reduction (volar plate arthroplasty)<br />
Lateral dislocation; collat. Lig. rupture & volar plate tear<br />
small rupture – body taping 4-6w; major- surgical repair<br />
Volar dislocation; rare; unstable; extensive trauma, central slip disruption<br />
Central slip repair + immobilization;<br />
Boutonierre deformity sequela<br />
DIPJ: open dislocation is more common (cutaneous anchoring to bone<br />
Debridement, reduction, splinting. Antibiotics; if closed- reduced & stable<br />
A WORD ABOUT JOINT DISLOCATIONS..<br />
MCPJ: dorsal dislocation; forced hyperextension<br />
Simple- reduction by wrist flex. & MCPJ tract. + flex.<br />
Early active motion<br />
Complex- prominence in palm & skin dimpling<br />
Rx: intra articular sesamoid bone (volar plate)<br />
Open redcution (dorsal approach)<br />
Lateral dislocation; forceful adduction / abduction; may not be noticed<br />
Partial tear- buddy taping protection 3w<br />
Complete tear- surgical repair<br />
CMCJ: axial loading<br />
If acute – easy reduction; pinning to maitain reduction<br />
Failure – pain, weakness,degenerative arthritis
ע"<br />
שת/<br />
תבט/<br />
ג"<br />
י<br />
23<br />
A WORD ABOUT JOINT DISLOCATIONS..<br />
Thumb IPJ: dislocation is rare; lateral (collateral lig.) or dorsal (volar plate)<br />
Immobilization for 3-4w<br />
Thumb MCPJ: ulnar collateral lig. Injuries; common; forced palmar abduct.-ex. (ski)<br />
Swollen & tender MPJ; at dist. origin; examination under local anesthesia<br />
Deviation under stress 20º = severe tear repair / arthrodesis<br />
* Stener lesion- adductor policis between the torn parts<br />
* Gamekeeper thumb- chron. UCL stertching<br />
Radial collateral lig. Injuries; at prox. Origin<br />
immediate repair vs. late arthrodesis<br />
Dorsal dislocation; forced hyperex. + longitudinal compression<br />
Neuropraxia possible;<br />
If simple – closed reduction, immobilization (25º flex.) for 2-3w<br />
If complex tear- of collateral ligs. & volar plates<br />
Thumb CMCJ: rare; can lead to chronicsubluxation