Principles of Microvascular Surgery.
Principles of Microvascular Surgery.
Principles of Microvascular Surgery.

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Principles</strong> <strong>of</strong><br />
<strong>Microvascular</strong> <strong>Surgery</strong>.<br />
Arik Zaretski M.D.<br />
Department <strong>of</strong> Plastic <strong>Surgery</strong><br />
Tel-Aviv Sourasky Medical Center.<br />
History<br />
• In the late 1890’s and early 1900’s -<br />
» surgeons began approximating blood vessels.<br />
» Laboratory animals and humans.<br />
» No magnification.<br />
• Hallowell, 1759 - repair <strong>of</strong> the brachial artery by<br />
hand suture.<br />
• J.B. Murphy, 1897 - described the first vascular<br />
anastomosis.<br />
• Alexis Carrel, 1902 - the triangulation method in<br />
end-to-end anastomosis in animals.<br />
1
History<br />
• Zachariah Janssen, 1590 -<br />
invention <strong>of</strong> the compound<br />
microscope.<br />
• Nylen, 1921 - first clinical<br />
application <strong>of</strong> monocular<br />
operating microscope - for<br />
human eardrum surgery.<br />
• Halmgren, 1921 -<br />
stereoscopical microscope<br />
for otolaryngological<br />
procedures.<br />
History<br />
• Perritt, 1950 - microsurgery in clinical<br />
ophthalmology.<br />
• Kurze, 1957 - microsurgery in neurosurgery.<br />
• Jacobson & Suarez, 1960 - microsurgical<br />
anastomosis in carotid arteries (1.4mm) <strong>of</strong><br />
laboratory animals with 100% patency rate.<br />
• Jacobson, 1965 - vessels 1mm in diameter with<br />
100% patency.<br />
• Green, 1966 - used 9-0 nylon suture on rat aortas<br />
(1.3mm) & vena cavas (2.7mm) with patency <strong>of</strong> 37<br />
out <strong>of</strong> 40 animals at 21 days.<br />
2
History<br />
• Malt & McKhann, 1962 - the first successful<br />
clinical replantation - 2 patients with arm<br />
amputations.<br />
• Chinese surgeons, 1963 - successful replantation<br />
<strong>of</strong> a hand amputated at the wrist.<br />
• kleinert & kasdan, 1963 - revascularized near<br />
amputated digits.<br />
» Loupe magnification.<br />
» Vain grafts.<br />
History<br />
• Nakayama, <strong>Surgery</strong> 1964 - The first clinical series<br />
<strong>of</strong> free tissue microsurgical transfers - cervical<br />
esophageal reconstruction with vascularized<br />
intestinal segments in 21 patients.<br />
• Buncke & Schulz, PRS 1965 - experimental<br />
replantation <strong>of</strong> rabbit ears and monkey digits.<br />
3
History<br />
• Komatsu & Tamai, PRS 1968 - first successful<br />
replantation <strong>of</strong> completely amputated digit.<br />
» Used surgical microscope.<br />
History<br />
• Krizek, PRS 1968 - first successful series <strong>of</strong> free<br />
flap transfers in a dog model.<br />
• Cobbett, J Bone Joint Surg 1968 - transferred a<br />
great toe to the hand.<br />
• Antia & Buch, Br J Plast Surg 1971 - superficial<br />
epigastric artery free flap (skin and fat) to fill a<br />
s<strong>of</strong>t-tissue defect in the cheek.<br />
• McLean & Bunke, PRS 1971 - omental free flap for<br />
large scalp defect.<br />
4
History<br />
• Danil & Taylor + O’brien, PRS 1973 - free groin<br />
flaps for lower extremity reconstruction.<br />
• Since the early 1970’s:<br />
» More donor sites.<br />
History<br />
» Refinement in microvascular tools and techniques.<br />
» Microsurgery became more prevalent.<br />
» Rapid gain <strong>of</strong> clinical experience.<br />
Improved results - better than 90% in most<br />
series.<br />
5
History<br />
• Khouri, 1992 - review <strong>of</strong> the clinical experience <strong>of</strong><br />
9 microsurgens.<br />
• Khouri found that:<br />
History<br />
» “Operative experience is the single most critical<br />
factor related to improved success rates…”<br />
6
Basic Science Concepts in<br />
Microsurgery<br />
• Vessel injury, repair and regeneration.<br />
• Process <strong>of</strong> vasospasm and thrombosis.<br />
» Pharmacological control.<br />
• Effects ischemia and hypoxia on revscularized<br />
tissue.<br />
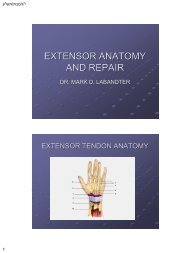
• Three basic layers:<br />
Vessel Anatomy<br />
» Intima - endothelial lining.<br />
» Media - smooth muscle.<br />
» Adventitia - outer connective tissue.<br />
7
Artery<br />
and vein<br />
Vein<br />
Vessel Injury and Regeneration<br />
• The beginning steps in the formation <strong>of</strong> a<br />
thrombotic plug:<br />
» Exposure <strong>of</strong> the subendothelium to the bloodstream.<br />
» Platelet aggregation.<br />
• The collagen (media and adventitia) stimulates<br />
platelet clumping.<br />
• <strong>Microvascular</strong> anastomoses can disturbs the<br />
endothelium and subendothelium.<br />
8
Vessel Injury and Regeneration<br />
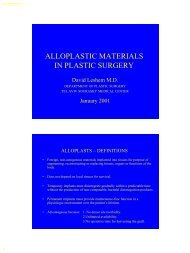
• Weinstein, 1979 - full thickness sutures:<br />
» <strong>of</strong>fer intimal continuity.<br />
» Less amount <strong>of</strong> anastomotic bleeding.<br />
» Less platelet aggregation.<br />
• Harashima, PRS 1976 - no difference in patency<br />
(94%) between adventitial or full thickness<br />
sutures.<br />
First day<br />
Group A Group B<br />
X100 X100<br />
9
Group B<br />
5th day 7th day<br />
Group A<br />
X300<br />
Two weeks<br />
X300<br />
Group B<br />
X100<br />
X100<br />
10
Vessel Wall Healing<br />
• At the time <strong>of</strong> the anastomosis - a layer <strong>of</strong> platelet<br />
covers the denuded endothelium.<br />
• Next 24-72 h - platelets gradually disappear.<br />
• Pseudointima forms within 5 days.<br />
• After 1 - 2 weeks - new endothelium covers the<br />
anastomotic site.<br />
• The elastic and muscular layers rarely return to<br />
their preinjury state.<br />
The critical period <strong>of</strong> thrombus formation<br />
is the first 3-5 days.<br />
Vessel Regeneration<br />
• Only the endothelial layer is damaged -<br />
reconstituted from surrounding cells, 7-10 days.<br />
• Damage to subendothelial structures -<br />
regeneration <strong>of</strong> epithelium by migration and<br />
differentiation <strong>of</strong> myoendothelial cells from the<br />
cut vessel ends.<br />
• Regeneration <strong>of</strong> other layers - proliferation <strong>of</strong><br />
fibroblasts, collagen and myointimal thickening at<br />
the anastomotic site.<br />
11
Endothelial Damage<br />
• Margic, PRS 1985 - dissection and exposure <strong>of</strong><br />
vessels from their beds.<br />
• Bipolar coagulation too close to the branch<br />
origin.<br />
• Dryness - exposed vessels should be kept in<br />
moist environment.<br />
• Prolonged vasospasm, more then 2h.<br />
• Injury from microvascular clips.<br />
• Needles and suture penetration + technique <strong>of</strong><br />
placement.<br />
Injury from microvascular clips<br />
• Directly related to clip pressure.<br />
• Curved or angled clip cause more damage than<br />
flat clip.<br />
• Closing pressures should remain below 30<br />
gr/mm 2 .<br />
Balloons<br />
Granulocyte<br />
Crater-like defect<br />
12
Damage from needles, sutures and technique<br />
• Large needles, obliquely placed sutured -<br />
» Endothelial lacerations.<br />
» Exposing subendothelium.<br />
» Platelet aggregation.<br />
• Repeat needle puncture -<br />
» Bleeding.<br />
» Large platelet plugs.<br />
• Unequal distances between sutures -<br />
» Endothelial gaps, distortion, constriction.<br />
» Exposure <strong>of</strong> intimal flaps.<br />
Damage from needles, sutures and technique<br />
• Loosely tied sutures -<br />
» Exposure <strong>of</strong> sub endothelial elements.<br />
» Excessive anastomotic bleeding.<br />
» Platelet plug formation.<br />
• Too many sutures or sutures tied too tightly -<br />
» Endothelial slough.<br />
• Excessive trauma to vessel walls, tension and<br />
loosely approximation -<br />
» Medial discontinuity.<br />
» Pseudoaneurysms.<br />
13
Damage from needles, sutures and technique<br />
• Chow, Br J plast surg 1982 - found greater<br />
tolerance for microanastomotic tension.<br />
• Acland & Trachtenberg, PRS 1977 - used SEM to<br />
evaluate microanastomoses, found 100% patency<br />
rate despite:<br />
» Intimal loss below the site <strong>of</strong> clamp pressure.<br />
» Medial necrosis at the site <strong>of</strong> the anastomosis.<br />
Some tissue damage is tolerated.<br />
Local factors<br />
• Lidman & Daniel, Ann Plast Surg 1981-<br />
» Anastomoses preformed in the zone <strong>of</strong> injury.<br />
» External compression <strong>of</strong> the anastomosis by<br />
hematoma, tight wound closure, swelling.<br />
14
The clotting mechanism<br />
• Platelets do not adhere to undamaged, healthy<br />
intimal surfaces.<br />
• Intimal injury - exposed collagen - platelet<br />
adhesion to the vessel surfaces.<br />
• Platelet activation.<br />
• Release <strong>of</strong> platelet granules.<br />
• Attract more platelet = aggregation.<br />
1<br />
The clotting mechanism<br />
• The activated platelet stimulates receptor site to<br />
which fibrinogen adheres.<br />
• Fibrinogen forms proteinaceous bridges between<br />
platelets.<br />
• Activated platelet - promote<br />
the change <strong>of</strong> fibrinogen to<br />
fibrin.<br />
• Fibrin promotes the “red clot”<br />
formation.<br />
2<br />
15
The clotting mechanism<br />
• Platelet contain 2 types <strong>of</strong> granules, contribute to<br />
platelet recruitment:<br />
» Alpha granules -<br />
• Von Willebrand factor.<br />
• Fibrinogen.<br />
» Dense granules -<br />
• ADP.<br />
• Calcium ions.<br />
• Serotonin.<br />
• When platelet aggregation reach a critical mass<br />
that causes thrombus formation by:<br />
» occluding the vessel, or-<br />
» Initiation <strong>of</strong> the classic extrinsic pathway <strong>of</strong> coagulation<br />
Antithrombotic therapy<br />
Heparin<br />
• Increases the action <strong>of</strong> antithrombin3 -inactivates<br />
thrombin.<br />
• Decrease platelet adhesion.<br />
• Decrease the conversion <strong>of</strong> fibrinogen to fibrin.<br />
» Greenberg, Masem and May, PRS 1988 - in a rabbit<br />
model, low dose heparin infusion significantly<br />
prevented anastomotic occlusion for 72 hours.<br />
» Khouri, PRS 1990 - single bolus <strong>of</strong> heparin given<br />
before blood flow was reestablished inhibited thrombus<br />
formation - preventing the conversion <strong>of</strong> fibrinogen to<br />
fibrin.<br />
16
Antithrombotic therapy<br />
Heparin (cont.)<br />
• Complications - hematoma formation, in animals<br />
12.5% (3 <strong>of</strong> 24).<br />
• Clinically - heparin is given to save free flaps.<br />
• Others - Johnson PC, PRS 1990 - heparin dose<br />
not improve the patency in uncomplicated repairs<br />
and increases the risk <strong>of</strong> bleeding.<br />
Antithrombotic therapy<br />
• Khouri, PRS 1998 -<br />
Heparin (cont.)<br />
» total <strong>of</strong> 493 free flaps preformed by 23 members <strong>of</strong> the<br />
International <strong>Microvascular</strong> Research Group in a<br />
prospective study.<br />
» The use <strong>of</strong> heparin solution for luminal irrigation had no<br />
apparent effect on thrombosis or failure.<br />
» Only subcutaneous heparin given post operatively had<br />
a significant effect - lower occurrence <strong>of</strong> postoperative<br />
thrombosis.<br />
17
Antithrombotic therapy<br />
Aspirin<br />
• Administered in low doses - 0.1 mM (325mg - PO).<br />
• Inhibits initial platelet aggregation at the<br />
anastomotic site.<br />
• Inhibits cyclooxygenase - blockage <strong>of</strong><br />
thromboxane A2.<br />
• Even at low doses - some inhibition <strong>of</strong> the release<br />
<strong>of</strong> prostacyclin (a potent vasodilator and platelet<br />
inhibitor).<br />
Antithrombotic therapy<br />
• Polysaccharide, molecular weights <strong>of</strong>: 40,000 or<br />
70,000.<br />
• Volume expander.<br />
• Antiplatelet.<br />
• Antifibrin.<br />
» Explanations:<br />
Dextran<br />
• raising <strong>of</strong> negative electrical charge on platelets.<br />
• Inactivation <strong>of</strong> von Willebrand factor.<br />
• Rothkopf, PRS 93 - patency <strong>of</strong> 85% in the dextran<br />
group and 48% in controls.<br />
18
Antithrombotic therapy<br />
Low molecular weight heparin<br />
• Ritter, J Reconstr Microsurg 1998 -<br />
» Anti factor 10a.<br />
» 66 epigastric free flap in rats.<br />
» Anastomotic patency was significantly improved .<br />
» Total tissue survival area was improved.<br />
» LMWH - improved anastomotic patency while<br />
minimizing hemorrhage.<br />
Antithrombotic therapy<br />
Proteolytic enzymes - Streptokinase & Urokinase<br />
• Streptokinase - produced by group C beta<br />
hemolytic streptococci.<br />
• Urokinase - produced by human kidney cells.<br />
• Both convert plasminogen into plasmin, a highly<br />
specific fibrinolytic enzyme.<br />
• Goldberg, J Reconst Microsurg 1989 - salvage <strong>of</strong><br />
6 <strong>of</strong> 7 thrombosed free flaps vessels ( subflap<br />
hematoma in 1 case).<br />
19
Antithrombotic therapy<br />
Tissue plasminogen activator (tPA)<br />
• Produced by human vascular endothelium.<br />
• Activates plasminogen (inactive precursor to<br />
plasmin).<br />
• Levy, J Reconst Microsurg 1991 - no difference<br />
between tPA and urokinase in the rat model.<br />
• Others report cases <strong>of</strong> free flap salvage with tPA<br />
infusion - Fedem & Walton, J Reconst Microsurg<br />
1989. Arnljots, PRS 1992. Romano, 1991.<br />
• Reports on selective tPA infusion.<br />
Antithrombotic therapy<br />
• Davies, Br J Plast Surg 1982 - surveyed the use <strong>of</strong><br />
anticoagulation in clinical microsurgery.<br />
» 73 centers in 22 countries.<br />
» Found equal success rates (89%) for free flaps with<br />
anticoagulation (n=691) and flaps without<br />
anticoagulation (n=134).<br />
» For limb replantation - success rat was lower with<br />
anticoagulation (76%) than without (89%).<br />
20
Antithrombotic therapy<br />
conclusions:<br />
• No definite indications when mechanical and<br />
vascular factors are optimal.<br />
• When there is thrombosis in the post operative<br />
period - flap reexploration and treatment with<br />
fibrinolytic and/or anticoagulation therapy.<br />
• Anticoagulation or fibrinolytic therapy may be<br />
indicated where mechanical or metabolic factors<br />
are not favorable and cannot be improved.<br />
Tissue response to ischemia and hypoxia<br />
• Free tissue transfer requires a period <strong>of</strong> tolerance<br />
to ischemia by the donor tissue.<br />
• Skin and subcutis are relatively resistant to<br />
anoxia -<br />
» Intracellular pH changes - reversible up to 24h.<br />
• Mammalian skeletal muscle -<br />
» much less tolerance to ischemia.<br />
» Irreversible damage to energy metabolism - 4h.<br />
» Irreversible damage starts at 6 hours.<br />
• Connective tissue (fibroblast, chondroblast,<br />
osteoblast) relatively resistant to hypoxia.<br />
21
Tissue response to ischemia and hypoxia<br />
• Cooling prolongs tolerance to ischemia in all<br />
types <strong>of</strong> tissues.<br />
» Donski, Br J Plast Surg 1980 - effect <strong>of</strong> cooling on<br />
groin flaps in rabbit - 86% survival after cooling for 1-3<br />
days.<br />
» Anderl, 1977 - stored a human groin flap for 24h.<br />
» Cooley, J Microsurg 1981 - in rats, max ischemia 6h at<br />
body temp and 48h if cooled.<br />
» Walkinshaw, PRS 1988 - proximal bowel segments<br />
are more resistant to warm ischemia at 2h.<br />
Tissue response to ischemia and hypoxia<br />
Tissue Warm Cold<br />
Skin & subcutaneous t. 4-6h Up to 12h<br />
Muscle
The no-reflow effect<br />
• Ames, Am J Pathol 1968 - studied the effect <strong>of</strong><br />
ischemia on rabbit brains.<br />
» Some ischemic organs failed to reperfuse after their<br />
blood supply was reestablished.<br />
» Called this - the no-reflow phenomenon.<br />
• Mechanism -<br />
» Cellular swelling in the vascular endothelium.<br />
» Intravascular platelet aggregation.<br />
» Leakage <strong>of</strong> intravascular fluid to the interstitial space.<br />
• Clinical observations -<br />
The no-reflow effect<br />
» Excellent blood flow immediately after anastomosis.<br />
» Decrease in blood flow shortly after.<br />
» The low flow state triggers intravascular thrombosis.<br />
» Flap ischemia.<br />
• May, PRS 1978 - no-reflow in groin flap in rabbits-<br />
» Mild obstruction to blood flow 1h post ischemia.<br />
» Increasing severity at 8 and 12h.<br />
» Histologic changes reversible at 4 and 8h.<br />
23
The no-reflow effect<br />
• Zdeblick, J Hand Surg 1985 - no-reflow in rat hind<br />
limbs.<br />
» Predictors -<br />
• RBC aggregates 5min after replantation.<br />
• Tissue pH change persisting for 1h or more<br />
postreplantation.<br />
» Mechanism -<br />
• Ongoing arterial obstruction.<br />
• AV shunting.<br />
• Altered thrombogenic / fibrinolitic system.<br />
• Jacobs, PRS 1981 -<br />
The no-reflow effect<br />
» relationship between warm ischemia time and<br />
fibrinolitic activity.<br />
» Greatest drop in fibrinolysis - 0-6h <strong>of</strong> warm ischemia.<br />
• Suval, J Surg Res 1987 -<br />
» Changes in microvascular permeability in reperfusion<br />
after 30min or 2h <strong>of</strong> ischemia.<br />
» First manifestation <strong>of</strong> tissue damage in reperfusion<br />
injury - d/t leukocytic and endothelial cell interaction.<br />
» The no-reflow - in 30% <strong>of</strong> muscle tissue regardless <strong>of</strong><br />
ischemia time.<br />
24
• Treatment -<br />
The no-reflow effect<br />
» Reports <strong>of</strong> flaps salvage with thrombolytic drugs.<br />
» Nonsteroidal antiinflamatory agents - inhibit<br />
cyclooxygenase - blocks thromboxane A2<br />
(vasoconstriction and thrombus formation).<br />
• Douglas, PRS 1987 - ibupr<strong>of</strong>en treated flaps survive<br />
longer periods <strong>of</strong> ischemia.<br />
• Accelerated fluorescein uptake - reversal <strong>of</strong> thrombosis<br />
and vasoconstriction.<br />
Flap failure - summary<br />
• Endothelial disruption.<br />
• Exposure <strong>of</strong> subendothelial collagen.<br />
• Platelet adherence and aggregation.<br />
• When critical mass - trigger <strong>of</strong> fibrin deposition.<br />
• Vasospasm.<br />
• Stenosis.<br />
• Thrombosis <strong>of</strong> the vessel.<br />
• Blood flow falls.<br />
• When critical level - flap failure.<br />
25
• Instruments.<br />
• Sutures.<br />
TECHNICAL FACTORS<br />
• Type <strong>of</strong> anastomoses.<br />
• Technique <strong>of</strong> anastomosis.<br />
Instruments and sutures<br />
• Loupes or operating microscope?<br />
• Loupes -<br />
» Shenaq, Klebuc and Vargo, PRS 1995 - 8 year<br />
experience. 251 free flaps with 5.5X loupes -<br />
• 97.2% successful.<br />
• Partial flap necrosis - 1.2%.<br />
• Revision 8.3%.<br />
• Free flap 98.5%, toe-to-hand 96.4%, digital replantation<br />
79.2%.<br />
• Good for vessels > 1mm.<br />
• Cost effective, portable, operator freedom.<br />
26
• Loupes…<br />
• Or microscope?<br />
Microsugical instruments<br />
• “few in number and high in quality”.<br />
27
• The number is critical!!!<br />
Number <strong>of</strong> sutures<br />
» Too few - excessive bleeding and thrombus formation.<br />
» Too many - increased damage to the endothelium.<br />
• The goal - well approximated, sealed,<br />
nonbleeding union with a minimum number <strong>of</strong><br />
sutures.<br />
• Cohen, PRS - 1979 - in rat femoral vessels 8-<br />
suture anastomosis is optimal.<br />
Type <strong>of</strong> sutures<br />
• Absorbable and nonabsorbale.<br />
• Mii, J Microsurg 1980 - smoother endothelial<br />
regeneration with polyglycolic acid sutures than<br />
with nonabsorbale material.<br />
• Thiede, J Microsurg 1979 - no increased<br />
aneurysm or pseudoaneurysm formation and no<br />
vascular raptures d/t decreased mechanical<br />
endurance with polyglycolic acid or polyglactin<br />
sutures.<br />
• Most surgeons use nonabsorable sutures - nylon<br />
or prolene.<br />
28
• Key sutures -<br />
Anastomotic technique<br />
» Carrel’s triangulation method- 120°.<br />
» 180° halving sutures.<br />
Interrupted or continuous sutures?<br />
• Simple interrupted full thickness<br />
sutures are preferred and are the<br />
standard to which all techniques<br />
are compared.<br />
• Continuous sutures -<br />
» Same patency rate.<br />
» Faster.<br />
» May narrow the caliber <strong>of</strong> the<br />
vessel lumen.<br />
» Cordeiro, Ann Plast Surg 1998<br />
- continuous suture<br />
anastomosis in 200 consecutive<br />
free flap - similar success rate.<br />
29
Interrupted or continuous sutures?<br />
• The sleeve technique -<br />
» Originally described by Lauritzen,<br />
Scan PRS 1980 -<br />
» Said to be:<br />
• faster, Simpler.<br />
• Suture cause less trauma to the<br />
vessels.<br />
• Less intraluminal suture exposure.<br />
• Lauritzen: “ endothelialization in<br />
haft the time”.<br />
» Clinically:<br />
• Difficult in veins.<br />
• Reports <strong>of</strong> stenosis, thrombus and<br />
aneurysm formation.<br />
• Sully, PRS 1982 - lower patency<br />
rate - 84% (normal - 98%).<br />
• O’Brien - “not superior in clinical<br />
situation”.<br />
End-to-end, end-to-side anastomosis<br />
• End-to-end anastomosis -<br />
» The most common type.<br />
» Size discrepancy up to 2:1.<br />
• End-to-side anastomosis -<br />
» when size discrepancy more then 2:1.<br />
» When limb or organ depends on a<br />
single vessel for perfusion.<br />
30
End-to-end, end-to-side and end-in-end<br />
• End-to-side anastomosis -<br />
» Godina, PRS 1979 -<br />
• higher failure rate with end-toend<br />
anastomosis.<br />
• End-to-side - choice for lower<br />
extremity free flaps.<br />
» Samaha, PRS 1997 -<br />
• no differences in patency rates<br />
in 1051 free flaps.<br />
» Animal experiments -<br />
• No difference in patency.<br />
• When different size - end-toside<br />
is better.<br />
• Flow dynamics in end-to-side<br />
are favorable.<br />
Stapling technique - anastomotic<br />
coupling systems<br />
• Nakayama, <strong>Surgery</strong> 1962 - the first ring device.<br />
• Ostrup & Berggren, Ann Plast Surg 1986 -<br />
modification, evolved into 3M microvascular<br />
anastomotic coupler.<br />
31
Stapling technique - anastomotic<br />
coupling systems<br />
• Clinical series -<br />
» Equal or greater patency<br />
rates.<br />
» Considerably faster.<br />
» Blair, Microsurgery 1989 -<br />
Histology - similar healing<br />
process.<br />
» Gilbert, Microsurgery 1989 -<br />
At 16 weeks postrepair<br />
coupled anastomoses are<br />
50% stronger.<br />
Nonpenetrating microvascular stapling device<br />
• Yamamoto, Ann Plast Surg 1999 -<br />
32
Laser anastomosis<br />
• Various experimental models and few clinical<br />
series.<br />
» Patency rate favorable.<br />
» Shorter operating time.<br />
» Limited endothelial trauma.<br />
» No suture material to induce foreign body reaction.<br />
Laser anastomosis<br />
• Wide rang <strong>of</strong> laser wavelengths -<br />
CO2, argon, neodymium:YAG, KPT<br />
and diode lasers.<br />
• Mechanism - still undefined.<br />
• Initial strength - physical factors<br />
(collagen coiling, crosslinking) not<br />
biological processes (inflammation<br />
and healing).<br />
33
Laser anastomosis<br />
• Tissue welding may be d/t simply heat generated<br />
by the laser energy or wavelength dependent.<br />
• The us <strong>of</strong> photosensitizing dyes makes low<br />
energy discharges possible - minimal collateral<br />
tissue damage.<br />
• To date - still investigational -<br />
» Aneurysm formation.<br />
» Low breaking and tensile<br />
strength in the early post<br />
operative period.<br />
» Cost.<br />
Monitoring perfusion<br />
• Free flap success is enhanced by the rapid<br />
identification and salvage <strong>of</strong> failing flaps.<br />
• Clinical assessment -<br />
» Skin color.<br />
» Temperature.<br />
» Capillary refill<br />
» Pinprick testing.<br />
• Devices to monitor blood flow should be -<br />
» highly reliable.<br />
» Simple to operate and interpret.<br />
» Inexpensive.<br />
34
Monitoring perfusion<br />
• Doppler ultrasound flowmeter -<br />
» The most common.<br />
» Arterial + venous flow.<br />
• Laser Doppler -<br />
Monitoring perfusion<br />
» Helium neon laser, penetrate 1.5mm,<br />
some light will be reflected by RBC<br />
moving in the capillaries in 1mm 3 <strong>of</strong><br />
tissue.<br />
» Continuously record the microcirculatory<br />
flow in all type <strong>of</strong> cutaneous and<br />
musculocutaneous free flaps.<br />
» Walkinshaw, Ann Plast Surg 1987 -<br />
• Unable to predict future clinical events.<br />
• No more accurate than clinical<br />
assessment in pointing the need for<br />
intervention.<br />
35
Monitoring perfusion<br />
• Temperature monitoring -<br />
» First described by Baudet, PRS 1976.<br />
» Good for skin or skin island flaps.<br />
» Unreliable in free muscle flaps.<br />
» Khouri & Shaw, PRS 1992 -<br />
• Series <strong>of</strong> 600 consecutive free flaps.<br />
• Monitored the temp difference between the flap and a<br />
control site.<br />
• Detected 52 thrombosed flaps - 45 salvaged.<br />
» Jones, PRS 1992 -<br />
• Pulse oxymeter is better for replanted digit.<br />
• Good only for skin that can be monitored more easily by<br />
capillary refill and Doppler probes.<br />
Monitoring perfusion<br />
• Implantable ultrasonic Doppler -<br />
» Direct monitoring.<br />
» Distinguish between arterial and<br />
venous occlusion.<br />
» More reliable than thermocouple<br />
probe.<br />
» Disa, Cordiero & Hidalgo, PRS<br />
1999 -<br />
• 750 free flaps, 673 nonburied.<br />
• Flap loss - 2.3%.<br />
• Buried flap loss - 6.5%, non were<br />
salvaged in reexploration.<br />
• The use <strong>of</strong> Implantable Doppler is<br />
recommended in buried flaps.<br />
36
The influence <strong>of</strong> patient factors<br />
• Tobacco use -<br />
» Cigarette smoking affect -<br />
• Cutaneous blood flow.<br />
• Wound healing.<br />
• Survival <strong>of</strong> pedicaled flaps.<br />
» Byproducts <strong>of</strong> cigarette smoke produce a<br />
thrombogenic state and vasoconstricting effect.<br />
» Large clinical series failed to show any damaging effect<br />
<strong>of</strong> cigarette smoking on free tissue transfer.<br />
» Reus, PRS 1992 - no difference in patency in 162 free<br />
flaps.<br />
» Buncke, J Reconstr Microsurgery 1996 -<br />
• 963 free flaps.<br />
• No survival or patency difference.<br />
• In smokers - higher incidence <strong>of</strong> healing complications at<br />
the flap interface or donor-site.<br />
The influence <strong>of</strong> patient factors<br />
» Cigarette smoking adversely affect the outcome <strong>of</strong><br />
digital replantation.<br />
» Blondeel, Br J Plast Surg 1999 - large series - 100<br />
free DIEP flaps for breast reconstruction - smoking was<br />
found to be a risk factor.<br />
37
Microanastomoses to irradiated vessels<br />
• Radiotherapy is known to impair wound healing -<br />
» decreasing the number <strong>of</strong> blood vessels.<br />
» Tissue ischemia.<br />
» Decreasing fibroblast proliferation and collagen<br />
production.<br />
• In earlier studies - patency was significantly lower<br />
in irradiated vessels.<br />
• Mulholland, PRS 1993 - similar failure rates in 226<br />
irradiated and in 108 nonirradiated.<br />
• Schusterman, PRS 1994 - large clinical series in<br />
prior radiotherapy do not predispose to a higher<br />
rate <strong>of</strong> acute flap loss or wound complications.<br />
Microanastomoses to irradiated vessels<br />
• Kroll, PRS 1996 - 854 consecutive free flaps - no<br />
effect to previous irradiation.<br />
• Guelincks, PRS 1984 -<br />
» limit dissection to recipient vessels.<br />
» Restrict electrocoagulation <strong>of</strong> arterial side branches.<br />
» Use small gauge needles.<br />
» Pass the needle from inside to outside.<br />
» Shorten the period <strong>of</strong> vessel cross clamping.<br />
» Flush vessels in heparinized solution.<br />
38
Free flaps<br />
• Twenty years ago - free tissue transfer was in the<br />
hands <strong>of</strong> few pioneers.<br />
• 10 years ago - primarily practiced at university<br />
centers.<br />
• Today -<br />
» free flap surgery is performed at an increasing rate and<br />
for expanding indications.<br />
» Free flaps in more difficult situations -<br />
• Irradiated fields.<br />
• Elderly patients.<br />
• Occlusive peripherovascular disease <strong>of</strong> lower extremity<br />
from arteriosclerosis or diabetes mellitus.<br />
• Success rates -<br />
Free flaps<br />
» 10 years ago - 90 - 94%, with 10% incidence <strong>of</strong><br />
thrombosis.<br />
» Khouri, PRS 1998 - in data from 9 microsurgical<br />
centers -<br />
• The success rate was 98.8%<br />
• Only 3.7% <strong>of</strong> flaps were reexplored for thrombosis.<br />
• Today - microsurgery is more than just to cover<br />
the wound - an esthetic final result is what most<br />
plastic surgeons currently strive for.<br />
39
Free flaps<br />
Free flaps<br />
• Failure <strong>of</strong> free tissue transfers -<br />
• Most <strong>of</strong>ten due to technical factors.<br />
• Khouri, PRS 1998 -<br />
» Most <strong>of</strong> the complications occurred in post traumatic<br />
reconstructions.<br />
» The magnitude <strong>of</strong> the traumatic insult is the single<br />
most important factor.<br />
» One should always seek the vascular pedicle <strong>of</strong> largest<br />
diameter - failures are high when small diameter<br />
pedicles are used, especially if ,1mm.<br />
40
• Free groin flap -<br />
Free flaps - skin<br />
» Superficial circumflex iliac a+v.<br />
» Concealment <strong>of</strong> the donor<br />
deformity.<br />
» Donor site - closed primarily.<br />
» Non hair bearing flap.<br />
» Short donor pedicle.<br />
» Arterial anomaly's.<br />
» Small external diameter 0.8-<br />
1.8mm.<br />
» Flap morbidity 15-20%.<br />
Free flaps - skin<br />
• Free radial forearm flap -<br />
» Radial a, cephalic/basilic v.<br />
» The most common and versatile<br />
skin flap.<br />
» Head and neck reconstructions.<br />
» Thin flap.<br />
» Osseous segment.<br />
» Long vascular pedicle, up to<br />
20cm.<br />
» Can be sensate flap.<br />
» Skin graft to donor site.<br />
» Donor site morbidity.<br />
41
• Free scapular flap -<br />
» Circumflex scapular a+v.<br />
Free flaps - skin<br />
» long vascular pedicle 6-14cm,<br />
arterial diameter 1.5-4.5mm.<br />
» Large flap.<br />
» Donor site closed primarily (up to<br />
9-10cm) - min morbidity.<br />
» Elevation - rapid and easy.<br />
» Nonsansate flap.<br />
» Thickness is variable (1.5-3cm).<br />
» Positioning the patient in lateral<br />
decubitus position.<br />
• Free parascpular flap -<br />
» Terminal branch <strong>of</strong> the<br />
descending circumflex<br />
scapular artery.<br />
» May be combined with the<br />
scapular flap.<br />
Free flaps - skin<br />
42
Free flaps - fascia<br />
• Useful where thin, well<br />
vascularized cover is needed.<br />
• Can provide unrestricted<br />
gliding <strong>of</strong> tendons in the hand.<br />
• Free temporoparietalis<br />
fascial flap -<br />
» Superficial temporal artery +v.<br />
Free flaps - muscle<br />
• Tamai, PRS 1970 - first report <strong>of</strong> free muscle<br />
transfer - rectus femoris muscle transfer in dogs.<br />
• Harii, Ohmori & Torii, PRS 1973 - free gracilis<br />
muscle for facial reanimation.<br />
• Surgical team in china - the lateral portion <strong>of</strong> the<br />
pectoralis major muscle to the forearm.<br />
• A common operation in plastic surgery.<br />
• The majority are to bring bulk <strong>of</strong> s<strong>of</strong>t tissue cover<br />
in traumatic losses, oncologic resections or<br />
osteomyelitis.<br />
43
• The most common -<br />
Free flaps - muscle<br />
» Latissimus dorsi and Rectus abdominis.<br />
• Reliable.<br />
• Large caliber.<br />
• Long vascular pedicles.<br />
• Relatively low donor site morbidity.<br />
• Histology - muscle fibers that are not reinnervted<br />
gradually degenerate and eventually replaced by<br />
fat cells.<br />
• Functional muscles -<br />
Free flaps - muscle<br />
» transfer <strong>of</strong> skeletal muscle by microvascular<br />
anastomosis + reinervation by microsurgical technique.<br />
» The working strength <strong>of</strong> a skeletal muscle is directly<br />
proportional to the cross-section area <strong>of</strong> the contracting<br />
muscle fibers.<br />
» The range <strong>of</strong> muscle contraction is a factor <strong>of</strong> fiber<br />
length.<br />
» The donor muscle nerve should match the anatomy <strong>of</strong><br />
the recipient nerve as possible.<br />
» Terzis, J Hand Surg 1978 - in rabbit rectus femoris -<br />
despite 100% patency <strong>of</strong> the anastomosis, only 25%<br />
working capacity.<br />
» Importance <strong>of</strong> reestablishing correct resting tension.<br />
44
Free flaps - muscle<br />
• Free latissimus dorsi muscle<br />
flap -<br />
» Thoracodorsal system.<br />
» The most common donor site.<br />
» Large - good for extensive defects.<br />
» Good for contaminated wounds.<br />
» Augments blood supply to areas <strong>of</strong><br />
deficiency.<br />
» Long and constant vascular pedicle -<br />
good for lower extremity.<br />
» Can be mayocutaneous.<br />
» Low donor site morbidity.<br />
• Free latissimus dorsi<br />
muscle flap -<br />
» Disadvantages -<br />
• Loss <strong>of</strong> functional<br />
motor unit - minimal<br />
effect on healthy<br />
patient.<br />
• Scar.<br />
Free flaps - muscle<br />
• Seroma at donor site.<br />
• Some winging <strong>of</strong> the<br />
scapula.<br />
45
Free flaps - osseous / osseocutaneous<br />
• First transfer - Ostrup & Friedrickson, PRS 1974 -<br />
• Buncke, PRS 1977 - free rib osseocutaneous flap<br />
to lower leg for tibial pseudoarthrosis.<br />
• Serafin, Br J Plast Surg 1977 - rib<br />
osseocutaneous flap for mandibular<br />
reconstruction.<br />
• Taylor, 1979 - first to report the free fibula flap.<br />
• Taylor, PRS 1978 - free iliac crest flap.<br />
Free flaps - osseous / osseocutaneous<br />
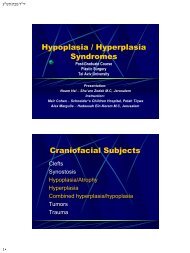
• The free fibula flap -<br />
» Peroneal vessels a+v.<br />
» Up to 26cm <strong>of</strong> vascularized cortical bone.<br />
» Blood supply - endosteal + musculoperiosteal.<br />
» Good for reconstruction <strong>of</strong> - femor, tibia, humerus,<br />
radius and ulna that are not amenable to grafting by<br />
conventional nonvascularized bone graft.<br />
» Mandibular reconstruction.<br />
» Cortical bone - stress and weight bearing.<br />
» The epiphysis <strong>of</strong> the fibular head supplied by branches<br />
<strong>of</strong> the tibial artery.<br />
46
Free fibula flap<br />
47
...<br />
הדות<br />
48