Seizures and Epilepsy
Seizures and Epilepsy
Seizures and Epilepsy

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
36 ■ Section 2: Common Pediatric Neurologic Problems<br />
Table 3-11.<br />
Prognostic Factors for Stopping AEDs<br />
Favorable Unfavorable<br />
Primary generalized epilepsy Partial epilepsy<br />
Idiopathic epilepsy Identifiable lesions<br />
Childhood onset Adult onset<br />
Easy to control Difficult to control<br />
Normal neurological examination Abnormal neurologic<br />
examination<br />
Normal intelligence Mental retardation<br />
More than 2–3 years seizure-free Less than 3 years seizurefree<br />
Normal EEG Epileptiform EEG<br />
From Geyer J, Keating J, Potts D, Carney P, eds. Neurology for the Boards. 3rd ed.<br />
Philadelphia: Lippincott Williams & Wilkins; 2006.<br />
Non-epileptic Events<br />
Non-epileptic events are unusual in the pediatric population,<br />
especially in the younger child. Several categories<br />
of non-epileptic events (thrashing, staring, etc.) have<br />
different natural histories <strong>and</strong> variable prognosis. Etiologies<br />
include conversion disorder, malingering, <strong>and</strong><br />
medical conditions, especially cardiac disorders. Symptoms<br />
suggesting non-epileptic events include closed<br />
eyes, resisted eyelid opening, non-physiologic progression,<br />
pelvic thrusting, lack of cyanosis, lack of tongue<br />
biting, variable semiology, crying, <strong>and</strong> rapid reorientation<br />
following the event. 54-56<br />
Neonatal <strong>Seizures</strong><br />
Neonatal seizures are poorly classified, under-recognized,<br />
especially in sick neonates, <strong>and</strong> often difficult to treat.<br />
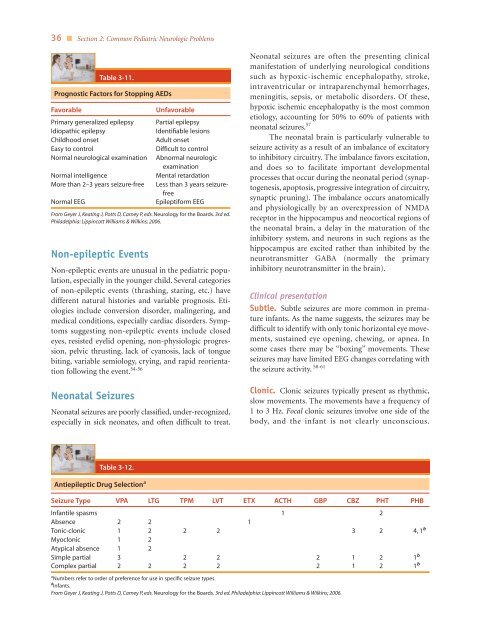
Table 3-12.<br />
Antiepileptic Drug Selection a<br />
Neonatal seizures are often the presenting clinical<br />
manifestation of underlying neurological conditions<br />
such as hypoxic-ischemic encephalopathy, stroke,<br />
intraventricular or intraparenchymal hemorrhages,<br />
meningitis, sepsis, or metabolic disorders. Of these,<br />
hypoxic ischemic encephalopathy is the most common<br />
etiology, accounting for 50% to 60% of patients with<br />
neonatal seizures. 57<br />
The neonatal brain is particularly vulnerable to<br />
seizure activity as a result of an imbalance of excitatory<br />
to inhibitory circuitry. The imbalance favors excitation,<br />
<strong>and</strong> does so to facilitate important developmental<br />
processes that occur during the neonatal period (synaptogenesis,<br />
apoptosis, progressive integration of circuitry,<br />
synaptic pruning). The imbalance occurs anatomically<br />
<strong>and</strong> physiologically by an overexpression of NMDA<br />
receptor in the hippocampus <strong>and</strong> neocortical regions of<br />
the neonatal brain, a delay in the maturation of the<br />
inhibitory system, <strong>and</strong> neurons in such regions as the<br />
hippocampus are excited rather than inhibited by the<br />
neurotransmitter GABA (normally the primary<br />
inhibitory neurotransmitter in the brain).<br />
Clinical presentation<br />
Subtle. Subtle seizures are more common in premature<br />
infants. As the name suggests, the seizures may be<br />
difficult to identify with only tonic horizontal eye movements,<br />
sustained eye opening, chewing, or apnea. In<br />
some cases there may be “boxing” movements. These<br />
seizures may have limited EEG changes correlating with<br />
the seizure activity. 58-61<br />
Clonic. Clonic seizures typically present as rhythmic,<br />
slow movements. The movements have a frequency of<br />
1 to 3 Hz. Focal clonic seizures involve one side of the<br />
body, <strong>and</strong> the infant is not clearly unconscious.<br />
Seizure Type VPA LTG TPM LVT ETX ACTH GBP CBZ PHT PHB<br />
Infantile spasms 1 2<br />
Absence 2 2 1<br />
Tonic-clonic 1 2 2 2 3 2 4, 1 bb<br />
Myoclonic 1 2<br />
Atypical absence 1 2<br />
Simple partial 3 2 2 2 1 2 1 bb<br />
Complex partial 2 2 2 2 2 1 2 1 bb<br />
aNumbers refer to order of preference for use in specific seizure types.<br />
bb<br />
Infants.<br />
From Geyer J, Keating J, Potts D, Carney P, eds. Neurology for the Boards. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 2006.