

Diagnostic et traitement des varices des membres inférieurs - KCE
Diagnostic et traitement des varices des membres inférieurs - KCE
Diagnostic et traitement des varices des membres inférieurs - KCE

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Referen<br />
ce<br />
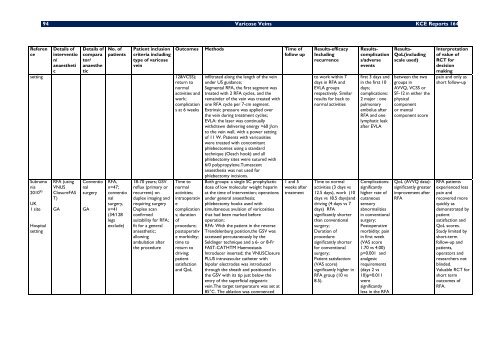
94 Varicose Veins <strong>KCE</strong> Reports 164<br />
D<strong>et</strong>ails of<br />
interventio<br />
n/<br />
anaesth<strong>et</strong>i<br />
c<br />
D<strong>et</strong>ails of<br />
compara<br />
tor/<br />
anaesthe<br />
tic<br />
No. of<br />
patients<br />
Patient inclusion<br />
criteria including<br />
type of varicose<br />
vein<br />
s<strong>et</strong>ting 12&VCSS);<br />
r<strong>et</strong>urn to<br />
normal<br />
activities and<br />
work;<br />
complication<br />
s at 6 weeks<br />
Subramo<br />
nia<br />
2010 95<br />
UK<br />
1 site<br />
Hospital<br />
s<strong>et</strong>ting<br />
RFA (using<br />
VNUS<br />
ClosureFAS<br />
T)<br />
GA<br />
Conventio<br />
nal<br />
surgery<br />
GA<br />
RFA,<br />
n=47;<br />
conventio<br />
nal<br />
surgery,<br />
n=41<br />
(34/128<br />
legs<br />
exclude)<br />
18-70 years; GSV<br />
reflux (primary or<br />
recurrent) on<br />
duplex imaging and<br />
requiring surgery<br />
Duplex scan<br />
confirmed<br />
suitability for RFA;<br />
fit for a general<br />
anaesth<strong>et</strong>ic;<br />
allowing<br />
ambulation after<br />
the procedure<br />
Outcomes M<strong>et</strong>hods Time of<br />
follow up<br />
Time to<br />
normal<br />
activities;<br />
intraoperativ<br />
e<br />
complication<br />
s; duration<br />
of<br />
procedure;<br />
postoperativ<br />
e morbidity;<br />
time to<br />
r<strong>et</strong>urn to<br />
driving;<br />
patient<br />
satisfaction<br />
and QoL<br />
infiltrated along the length of the vein<br />
under US guidance;<br />
Segmental RFA, the first segment was<br />
treated with 2 RFA cycles, and the<br />
remainder of the vein was treated with<br />
one RFA cycle per 7-cm segment.<br />
Extrinsic pressure was applied over<br />
the vein during treatment cycles;<br />
EVLA: the laser was continually<br />
withdrawn delivering energy >60 J/cm<br />
to the vein wall, with a power s<strong>et</strong>ting<br />
of 11 W. Patients with varicosities<br />
were treated with concomitant<br />
phlebectomies using a standard<br />
technique (Oesch hook) and all<br />
phlebectomy sites were sutured with<br />
6/0 polypropylene.Tumescent<br />
anaesthesia was not used for<br />
phlebectomy incisions.<br />
Both groups: a single SC prophylactic<br />
dose of low molecular weight heparin<br />
at the time of intervention; operations<br />
under general anaesthesia;<br />
phlebectomy hooks used with<br />
simultaneous avulsion of varicosities<br />
that had been marked before<br />
operation;<br />
RFA: With the patient in the reverse<br />
Trendelenburg position,the GSV was<br />
accessed percutaneously by the<br />
Seldinger technique and a 6- or 8-Fr<br />
FAST-CATHTM Haemostasis<br />
Introducer inserted; the VNUSClosure<br />
PLUS intravascular cath<strong>et</strong>er with<br />
bipolar electro<strong>des</strong> was introduced<br />
through the sheath and positioned in<br />
the GSV with its tip just below the<br />
entry of the superficial epigastric<br />
vein.The targ<strong>et</strong> temperature was s<strong>et</strong> at<br />
85°C. The ablation was commenced<br />
1 and 5<br />
weeks after<br />
treatment<br />
Results-efficacy<br />
Including<br />
recurrence<br />
to work within 7<br />
days in RFA and<br />
EVLA groups<br />
respectively. Similar<br />
results for back to<br />
normal activities<br />
Time to normal<br />
activities (3 days vs<br />
12.5 days), work (10<br />
days vs 18.5 days)and<br />
driving (4 days vs 7<br />
days) RFA<br />
significantly shorter<br />
than conventional<br />
surgery;<br />
Duration of<br />
procedure:<br />
significantly shorter<br />
for conventional<br />
surgery;<br />
Patient satisfaction:<br />
(VAS score)<br />
significantly higher in<br />
RFA group (10 vs<br />
8.5).<br />
Resultscomplication<br />
s/adverse<br />
events<br />
first 3 days and<br />
in the first 10<br />
days;<br />
complications:<br />
2 major : one<br />
pulmonary<br />
embolus after<br />
RFA and one<br />
lymphatic leak<br />
after EVLA<br />
Complications:<br />
significantly<br />
higher rate of<br />
cutaneous<br />
sensory<br />
abnormalities<br />
in conventional<br />
surgery;<br />
Postoperative<br />
morbidity: pain<br />
in first week<br />
(VAS score<br />
1.70 vs 4.00)<br />
p=0.001 and<br />
analgesic<br />
requirements<br />
(days 2 vs<br />
10)p=0.011<br />
were<br />
significantly<br />
less in the RFA<br />
Results-<br />
QoL(including<br />
scale used)<br />
b<strong>et</strong>ween the two<br />
groups in<br />
AVVQ, VCSS or<br />
SF-12 in either the<br />
physical<br />
component<br />
or mental<br />
component score<br />
QoL (AVVQ data):<br />
significantly greater<br />
improvement after<br />
RFA<br />
Interpr<strong>et</strong>ation<br />
of value of<br />
RCT for<br />
decision<br />
making<br />
pain and only as<br />
short follow-up<br />
RFA patients<br />
experienced less<br />
pain and<br />
recovered more<br />
quickly as<br />
demonstrated by<br />
patient<br />
satisfaction and<br />
QoL scores.<br />
Study limited by<br />
short-term<br />
follow-up and<br />
patients,<br />
operators and<br />
researchers not<br />
blinded.<br />
Valuable RCT for<br />
short term<br />
outcomes of<br />
RFA.













