Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
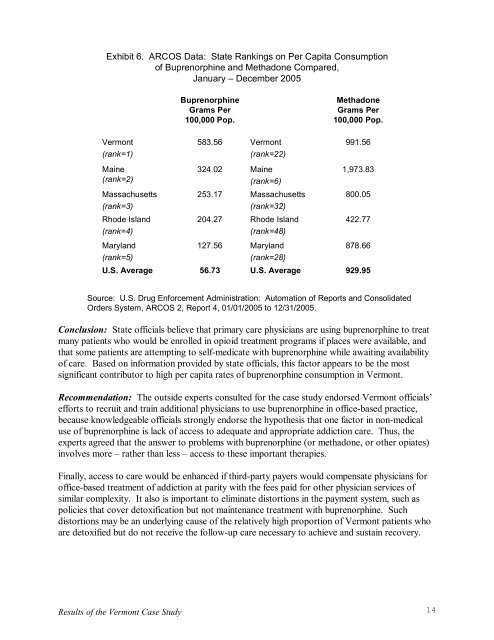
Exhibit 6. ARCOS Data: State Rankings on Per Capita Consumption<br />
<strong>of</strong> <strong>Buprenorphine</strong> <strong>and</strong> Methadone Compared,<br />
January – December 2005<br />
Vermont<br />
(rank=1)<br />
Maine<br />
(rank=2)<br />
Massachusetts<br />
(rank=3)<br />
Rhode Isl<strong>and</strong><br />
(rank=4)<br />
Maryl<strong>and</strong><br />
(rank=5)<br />
U.S. Average<br />
<strong>Buprenorphine</strong><br />
Grams Per<br />
100,000 Pop.<br />
Methadone<br />
Grams Per<br />
100,000 Pop.<br />
583.56 Vermont 991.56<br />
(rank=22)<br />
324.02 Maine 1,973.83<br />
(rank=6)<br />
253.17 Massachusetts 800.05<br />
(rank=32)<br />
204.27 Rhode Isl<strong>and</strong> 422.77<br />
(rank=48)<br />
127.56 Maryl<strong>and</strong> 878.66<br />
(rank=28)<br />
56.73 U.S. Average 929.95<br />
Source: U.S. Drug Enforcement Administration: Automation <strong>of</strong> Reports <strong>and</strong> Consolidated<br />
Orders System, ARCOS 2, Report 4, 01/01/2005 to 12/31/2005.<br />
Conclusion: State <strong>of</strong>ficials believe that primary care physicians are using buprenorphine to treat<br />
many patients who would be enrolled in opioid treatment programs if places were available, <strong>and</strong><br />
that some patients are attempting to selfmedicate with buprenorphine while awaiting availability<br />
<strong>of</strong> care. Based on information provided by state <strong>of</strong>ficials, this factor appears to be the most<br />
significant contributor to high per capita rates <strong>of</strong> buprenorphine consumption in Vermont.<br />
Recommendation: The outside experts consulted for the case study endorsed Vermont <strong>of</strong>ficials’<br />
efforts to recruit <strong>and</strong> train additional physicians to use buprenorphine in <strong>of</strong>ficebased practice,<br />
because knowledgeable <strong>of</strong>ficials strongly endorse the hypothesis that one factor in nonmedical<br />
use <strong>of</strong> buprenorphine is lack <strong>of</strong> access to adequate <strong>and</strong> appropriate addiction care. Thus, the<br />
experts agreed that the answer to problems with buprenorphine (or methadone, or other opiates)<br />
involves more – rather than less – access to these important therapies.<br />
Finally, access to care would be enhanced if thirdparty payers would compensate physicians for<br />
<strong>of</strong>ficebased treatment <strong>of</strong> addiction at parity with the fees paid for other physician services <strong>of</strong><br />
similar complexity. It also is important to eliminate distortions in the payment system, such as<br />
policies that cover detoxification but not maintenance treatment with buprenorphine. Such<br />
distortions may be an underlying cause <strong>of</strong> the relatively high proportion <strong>of</strong> Vermont patients who<br />
are detoxified but do not receive the followup care necessary to achieve <strong>and</strong> sustain recovery.<br />
Results <strong>of</strong> the Vermont Case Study<br />
14