Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Vermont<br />
Maine<br />
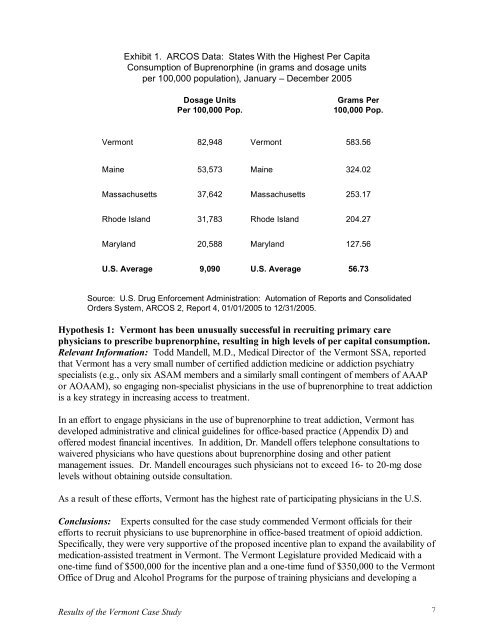
Exhibit 1. ARCOS Data: States With the Highest Per Capita<br />
Consumption <strong>of</strong> <strong>Buprenorphine</strong> (in grams <strong>and</strong> dosage units<br />
per 100,000 population), January – December 2005<br />
Massachusetts<br />
Rhode Isl<strong>and</strong><br />
Maryl<strong>and</strong><br />
U.S. Average<br />
Dosage Units Grams Per<br />
Per 100,000 Pop. 100,000 Pop.<br />
82,948 Vermont 583.56<br />
53,573 Maine 324.02<br />
37,642 Massachusetts 253.17<br />
31,783 Rhode Isl<strong>and</strong> 204.27<br />
20,588 Maryl<strong>and</strong> 127.56<br />
9,090 U.S. Average 56.73<br />
Source: U.S. Drug Enforcement Administration: Automation <strong>of</strong> Reports <strong>and</strong> Consolidated<br />
Orders System, ARCOS 2, Report 4, 01/01/2005 to 12/31/2005.<br />
Hypothesis 1: Vermont has been unusually successful in recruiting primary care<br />
physicians to prescribe buprenorphine, resulting in high levels <strong>of</strong> per capital consumption.<br />
Relevant Information: Todd M<strong>and</strong>ell, M.D., Medical Director <strong>of</strong> the Vermont SSA, reported<br />
that Vermont has a very small number <strong>of</strong> certified addiction medicine or addiction psychiatry<br />
specialists (e.g., only six ASAM members <strong>and</strong> a similarly small contingent <strong>of</strong> members <strong>of</strong> AAAP<br />
or AOAAM), so engaging nonspecialist physicians in the use <strong>of</strong> buprenorphine to treat addiction<br />
is a key strategy in increasing access to treatment.<br />
In an effort to engage physicians in the use <strong>of</strong> buprenorphine to treat addiction, Vermont has<br />
developed administrative <strong>and</strong> clinical guidelines for <strong>of</strong>ficebased practice (Appendix D) <strong>and</strong><br />
<strong>of</strong>fered modest financial incentives. In addition, Dr. M<strong>and</strong>ell <strong>of</strong>fers telephone consultations to<br />
waivered physicians who have questions about buprenorphine dosing <strong>and</strong> other patient<br />
management issues. Dr. M<strong>and</strong>ell encourages such physicians not to exceed 16 to 20mg dose<br />
levels without obtaining outside consultation.<br />
As a result <strong>of</strong> these efforts, Vermont has the highest rate <strong>of</strong> participating physicians in the U.S.<br />
Conclusions: Experts consulted for the case study commended Vermont <strong>of</strong>ficials for their<br />
efforts to recruit physicians to use buprenorphine in <strong>of</strong>ficebased treatment <strong>of</strong> opioid addiction.<br />
Specifically, they were very supportive <strong>of</strong> the proposed incentive plan to exp<strong>and</strong> the availability <strong>of</strong><br />
medicationassisted treatment in Vermont. The Vermont Legislature provided Medicaid with a<br />
onetime fund <strong>of</strong> $500,000 for the incentive plan <strong>and</strong> a onetime fund <strong>of</strong> $350,000 to the Vermont<br />
Office <strong>of</strong> Drug <strong>and</strong> Alcohol Programs for the purpose <strong>of</strong> training physicians <strong>and</strong> developing a<br />
Results <strong>of</strong> the Vermont Case Study<br />
7