Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...
Diversion and Abuse of Buprenorphine: A Brief Assessment of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
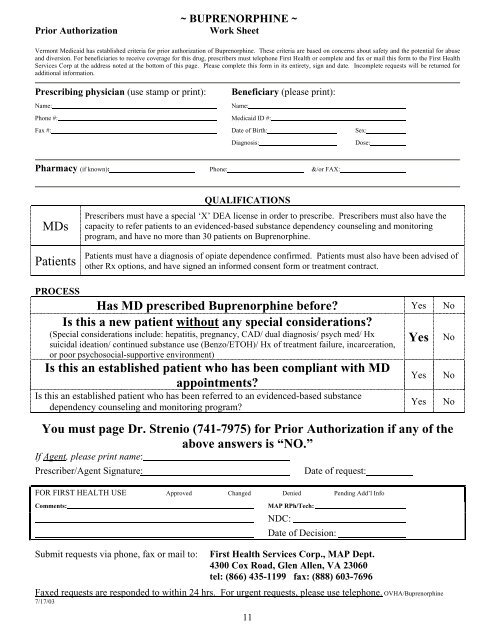
~ BUPRENORPHINE ~<br />
Prior Authorization Work Sheet<br />
Vermont Medicaid has established criteria for prior authorization <strong>of</strong> <strong>Buprenorphine</strong>. These criteria are based on concerns about safety <strong>and</strong> the potential for abuse<br />
<strong>and</strong> diversion. For beneficiaries to receive coverage for this drug, prescribers must telephone First Health or complete <strong>and</strong> fax or mail this form to the First Health<br />
Services Corp at the address noted at the bottom <strong>of</strong> this page. Please complete this form in its entirety, sign <strong>and</strong> date. Incomplete requests will be returned for<br />
additional information.<br />
Prescribing physician (use stamp or print): Beneficiary (please print):<br />
Name: Name:<br />
Phone #: Medicaid ID #:<br />
Fax #: Date <strong>of</strong> Birth: Sex:<br />
Diagnosis: Dose:<br />
Pharmacy (if known): Phone: &/or FAX:<br />
QUALIFICATIONS<br />
Prescribers must have a special ‘X’ DEA license in order to prescribe. Prescribers must also have the<br />
MDs capacity to refer patients to an evidenced-based substance dependency counseling <strong>and</strong> monitoring<br />
program, <strong>and</strong> have no more than 30 patients on <strong>Buprenorphine</strong>.<br />
Patients must have a diagnosis <strong>of</strong> opiate dependence confirmed. Patients must also have been advised <strong>of</strong><br />
Patients other Rx options, <strong>and</strong> have signed an informed consent form or treatment contract.<br />
PROCESS<br />
Has MD prescribed <strong>Buprenorphine</strong> before?<br />
Is this a new patient without any special considerations?<br />
Yes No<br />
(Special considerations include: hepatitis, pregnancy, CAD/ dual diagnosis/ psych med/ Hx<br />
suicidal ideation/ continued substance use (Benzo/ETOH)/ Hx <strong>of</strong> treatment failure, incarceration,<br />
or poor psychosocial-supportive environment)<br />
Yes No<br />
Is this an established patient who has been compliant with MD<br />
appointments?<br />
Is this an established patient who has been referred to an evidenced-based substance<br />
dependency counseling <strong>and</strong> monitoring program?<br />
Yes No<br />
Yes No<br />
You must page Dr. Strenio (741-7975) for Prior Authorization if any <strong>of</strong> the<br />
above answers is “NO.”<br />
If Agent, please print name:<br />
Prescriber/Agent Signature: Date <strong>of</strong> request:<br />
FOR FIRST HEALTH USE Approved Changed Denied Pending Add’l Info<br />
Comments: MAP RPh/Tech:<br />
NDC:<br />
Date <strong>of</strong> Decision:<br />
Submit requests via phone, fax or mail to: First Health Services Corp., MAP Dept.<br />
4300 Cox Road, Glen Allen, VA 23060<br />
tel: (866) 435-1199 fax: (888) 603-7696<br />
Faxed requests are responded to within 24 hrs. For urgent requests, please use telephone. OVHA/<strong>Buprenorphine</strong><br />
7/17/03<br />
11