卵巢癌 - 臺北榮民總醫院
卵巢癌 - 臺北榮民總醫院
卵巢癌 - 臺北榮民總醫院

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
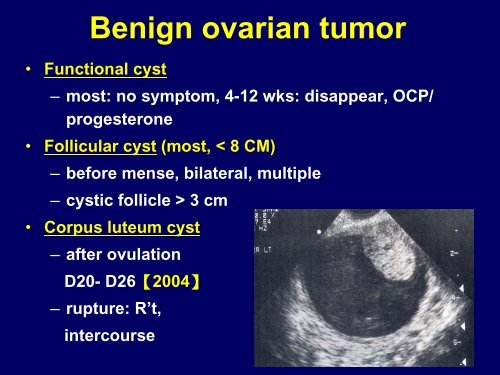
Benign ovarian tumor<br />
• Functional cyst<br />
– most: no symptom, 4-12 wks: disappear, OCP/<br />
progesterone<br />
• Follicular cyst (most, < 8 CM)<br />
– before mense, bilateral, multiple<br />
– cystic follicle > 3 cm<br />
• Corpus luteum cyst<br />
– after ovulation<br />
D20- D26【2004】<br />
– rupture: R’t,<br />
intercourse
• Thecal luteum cyst<br />
– due to Beta-HCG (endo-/ecto-), bilateral<br />
• Luteoma<br />
– not true neoplasm<br />
– Masculinization: [M] / [F]: 30% / 65%<br />
– 母親及女嬰男性化 [2007]<br />
• Granulosa cell tumor<br />
– Fibroma<br />
– Meig’ s syndrome (ascites, PE, fibroma) [200?]<br />
• Epithelial cyst<br />
– Mucinous cystadenoma – huge<br />
– Serous cystadenoma – bilateral, 20 %,<br />
Psamoma Body: fine calcification granulation
• Dermoid cyst<br />
– 15% torsion(中等大小), 10 % bilateral, 1-3 % SCC<br />
– WBC, abd. pain, tenderness -> surgery [1996]<br />
– The most common tumor of the first decade of life<br />
->>>>> dysgerminoma (malignancy)
Fluid-Fluid Level
Dermoid cyst (mature cystic teratoma: triphasic teratoma)<br />
[1997] 毛髮, 牙齒, 軟骨, 皮膚附屬器官
註:Struma Ovarii<br />
~ 甲狀腺組織 thyroid tissue<br />
~ 為 monodermal teratoma 中的一種
• [2007] 下列何者為最常見的生殖細胞腫瘤(germ-cell tumor)?<br />
– 惡性胚胎瘤(dysgerminoma)<br />
– 絨毛膜癌(choriocarcinoma)<br />
– 內胚層竇瘤(endodermal sinus tumor)<br />
– 成熟性畸胎瘤(mature teratoma)<br />
• [2008] 一位20 歲女大學生因急性腹痛而接受手術,取出卵巢腫瘤(如<br />
下圖所示),則下列診斷何者最正確?<br />
– 卵巢外孕 - 卵巢畸胎瘤 - 卵巢單純囊腫 - 卵巢黃體囊腫
Ovarian mass management<br />
• Expectant<br />
– Functional<br />
• For resolution of functional<br />
ovarian cyst<br />
– No difference between<br />
observation and OCP<br />
• OCP<br />
– Reducing the risk of<br />
subsequent ovarian cyst<br />
• Suspected ovarian torsion<br />
– Surgical<br />
• Exploratory<br />
– avoid in a suspicion of<br />
malignancy<br />
• Size<br />
– Before menopause<br />
• 3.5X2x1.5 cm<br />
– In early menopause<br />
• 2x1.5x0.5 cm<br />
– In late menopause<br />
• 1.5x0.75x0.5 cm
[2006]<br />
Unilocular: 3-6 M f/u<br />
Solid part or > 8-10 cm: op<br />
Multiloculate: pre-MC: karyotype, AFP<br />
post-MC: 3-6 M f/u / OCP<br />
Few than 1 ~ 2 % ovarian malignancy occur in children<br />
10~35 % malignancy in children and adolescent (< 20 y/o)<br />
Germ cell tumor : 50 ~ 70 % ovarian neoplasm (< 20 y/o) : 20% 成人
• Endometriosis<br />
– presence of endometrial tissue (gland and stroma) outside<br />
the uterus<br />
– 7% of reproductive age women (25-45 y/o [1996] ) most<br />
frequent site: ovary, uterosacral ligament, pelvic viscera .<br />
peritoneum, uterus, CDS …<br />
– Etiology<br />
• 1.retrograde menstruation<br />
• 2.ectopic transplantation of endometrial tissue<br />
• 3.coelomic metaplasia<br />
• 4.the induction theory<br />
• 5.immunological factor<br />
• 6.multifactorial gene (family history, first-degree)<br />
– S/S: 經痛,不孕, 出血, 性交痛 (週期性血尿 xxxx [2000] )
• Endometrioma<br />
– Chocolate cyst<br />
– CA-125: PID, menses, myoma, endometriosis, pregnancy,<br />
ovarian cancer, pancreatic/renal/hepatic disease ([2001]<br />
EM hyperplasia xxxxxx)<br />
Novak’s<br />
Textbook
UT<br />
chocolate
[2005] 下列何者能正確診斷出內膜異位症?<br />
1.腹腔鏡. 2.超音波. 3.電腦斷層. 4.內診
Mild / Peritoneum / US ligament
Mild / Uterine Superficial
Severe / Adhesion Bands
Surgery
– American Society for Reproductive Medicine<br />
• Stage 1(minimal): 1~5, stage 2 (mild): 6~15,<br />
stage 3(moderate): 16~40, stage 4 (severe): >40<br />
• Depth, appearance, size, adhesion<br />
• Not degree of pain/ infertility<br />
– [2002] 右側 5 cm卵巢深層endometrioma, 為stage ?
藥物治療 ( [1998] Estrogen and Tamoxifen xxxxx )<br />
• NSAIDs<br />
– 可以抑制導致疼痛的前列腺素,有效治療因子宮內膜異位而引起之經痛,<br />
並減少發炎反應<br />
• Danazol (Androgen/ Anti-gonadotropic agent)<br />
– Pseudo-menopause<br />
– 對減少子宮內膜異位症所造成之疼痛非常有效<br />
– 會有體重增加,水腫,痤瘡,油脂性皮膚及多毛症的副作用<br />
• 促性腺激素釋放素(GnRH agonist)<br />
– Medical oophorectomy<br />
– 現今廣泛使用於治療子宮內膜異位症之藥物<br />
• 避孕藥<br />
– Pseudo-pregnancy<br />
– 避孕藥常為用來治療子宮內膜異位症所造成的慢性疼痛,它的治療作用是<br />
抑制排卵,減少促性腺激素及月經量,促使異位的內膜脫落<br />
• 黃體素<br />
– 作用機轉是抑制下丘腦及腦垂體中樞,降低血液裡雌激素的濃度;並可直<br />
接作用於子宮內膜,讓異位之內膜組織萎縮脫落。同時,可抑制血管增生<br />
來減少內膜移植和腹腔內發炎
• [2004] endometriosis 的敘述, 何者為非 ?<br />
– 1.estrogen dependent disease<br />
– 2.endometrial tissue ectopic growth<br />
– 3.family hx (7 x, if a first-degree relative)<br />
– 4.no association with immune system.<br />
• [2005] 28 y/o, infertility, bilateral ov tumor by sonar,<br />
operation->endometrioma, tube: ok -> 以下何者非第一線之<br />
後續治療 ?<br />
– 1.pregnancy after operation<br />
– 2.Danazol<br />
– 3.GnRH-a<br />
– 4.IVF.
• [2006] 目前治療輕度至中度子宮內膜異位症的藥物,下列那<br />
一項錯誤?<br />
– Progestins (黃體素)<br />
– Dexamethasone.<br />
– Danazol<br />
– Gonadotropin-releasing hormone(GnRH)agonist<br />
• [2008] 一位42 歲母親,20 年前罹患子宮內膜異位症曾接受手<br />
術治療,現在她的大女兒也有相同疾病,她很擔心二女兒也<br />
會有相同疾病。據你所知,子宮內膜異位症可能是下列那一<br />
種疾病?<br />
– Autosomal recessive with variable penetrance<br />
– Polygenic multifactorial<br />
– Spontaneous mutations<br />
– No evidence of genetic inheritance
• [2008] 一位25 歲女性,訴說常常在月經的前兩天開始就<br />
感到劇烈的下腹疼痛,疼痛並且一直持續到月經結束,這<br />
已經持續有一年的時間。在此之前,她通常是在月經來的<br />
第一天才會感覺到疼痛。她自行吃止痛藥,但無法改善症<br />
狀。因此到婦產科醫院求診,經超音波檢查後,發現左側<br />
卵巢有個6 公分的卵巢囊腫。她向來月經週期都很準時是<br />
28 天,每次也都持續約5 天左右,經血量也沒什麼特別之<br />
處。醫師在診查之後,心中已有初步臆斷,因此處方黃體<br />
素給予治療。果然,投藥後疼痛症狀即稍有改善。你覺得<br />
最可能的診斷是:<br />
– 卵巢功能退化<br />
– 子宮肌瘤<br />
– 黃體囊腫<br />
– 子宮內膜異位
Ovarian Cancer<br />
Novak’s (Ch 35), 台北榮總實用婦產部手冊 (page 170)<br />
• Incidence increases with age<br />
Survival guide 4.0 (page 85)<br />
• 60% of patients present advanced disease<br />
• Overall 5-year survival rate: 38%<br />
• Increased risk<br />
– Advancing age (age 40 or 79: 15.7/100,000 or 54/100,000)<br />
– Family history (RR 3.6, lifetime risk 5%-7%)<br />
– Genetic lineage (lifetime risk 50%)<br />
• BRCA1 (17), BRCA2 (13), HNPCC (lynch II), P53, Cmyc,<br />
Ras, HER2/Neu
• Increased risk (續)<br />
– Nulliparity (2X)<br />
– Ethnicity (North America and Europe)<br />
– Talc powder ? High-fat diet ? Fertility drugs ?<br />
• Decreased risk<br />
– Prolonged breast feeding<br />
– Oral contraceptives<br />
• [2004, 2005] OV ca, EM ca, ectopic, benign breast<br />
disease, functional ov cyst, PID, myoma, colon ca,<br />
endometriosis, dysmenorrhea<br />
• [2005] 增加藥效 : BZD, Coffeine, Theophylline,<br />
Alcohol, Diazepam. 減少藥效:Aspirin, Morphine<br />
• Thrombosis, stroke, DVT, DM, HTN(mild), TG<br />
– Multiparous<br />
– Reproductive surgery (tubal ligation, TAH)
• Epithelial (most) -> CA-125<br />
– Serous (75%) [2007]<br />
– Mucinous (25%)<br />
– Endometroid<br />
– Clear cell (DES)<br />
• Germ cell -> AFP, HCG-> dysgerminoma (most) ←→<br />
mature cystic teratoma<br />
• Stromal ->LDH, inhibin<br />
• Metastatic (6-7%, 雙側) (krukenberg) -> CEA [2004]<br />
– [1998] Stomach/ Breast/ Colon ca (bladder XXX)<br />
– 1.presence of ovarian stromal invasion<br />
– 2.mucin-producting signet-ring cell [2000]<br />
– 3.ovarian stromal sarcomatoid proliferation
Endodermal sinus tumor (yolk-sac tumor) : Schiller-Duval body<br />
Granulosa cell tumor : Coffee-bean nuclei, Call-exner body<br />
Serous tumor : Psammoma body<br />
Clear cell carcinoma : Hobnail cell<br />
Mucinous tumor: Pseudomyxoma
• Borderline tumor<br />
– 30-50 y/o, pre-menopauseal women<br />
– or low malignant potential (more atypia/<br />
mitosis than benign ovarian tumor)<br />
– 5 years survival rate: > 80 %, good prognosis<br />
– pathology:<br />
• 1.epithelial proliferation, papillary<br />
formation, pseudostratification<br />
• 2.nuclear atypia/ mitosis<br />
• 3.absence of true stromal invasion
• [2003, 2005] S/S (most: no symptom)<br />
– Abdominal pain<br />
– Urinary frequency and urgency<br />
– Constipation or diarrhea<br />
– Abnormal vaginal bleeding<br />
– Abdominal distension<br />
– Increased abdominal girth<br />
– Dyspnea<br />
– Abdominal mass<br />
– Pelvic mass<br />
– Pleural effusion<br />
– Ascites
• Survery<br />
– Pelvic examination<br />
– Transvaginal ultrasound (solid part, septum, papillary<br />
growth, multilocular, ascites, > 6 cm)<br />
– [2007] benign: cystic<br />
– [2005] Color Doppler imaging (PI< 0.8, RI
• CA-125<br />
– Elevated (>35) in 80% of all cases<br />
– Elevated in only 50% of stage I cases<br />
– Low specificity (PID, menses, myoma, endometriosis,<br />
pregnancy, pancreatic / renal / hepatic disease)<br />
– Most useful for follow-up<br />
• Stage I [2001] 單側 ov ca+ascites. [1998] capsule有
• Stage II [to CDS, to broad ligament, to uterus]<br />
• IIIA: microscopic peritoneal metastasis beyond pelvis<br />
• IIIB: macroscopic peritoneal metastasis (< 2cm)<br />
• IIIC: peritoneal metastasis beyond pelvis (> 2cm )<br />
and/or regional node metastasis [1998, 1997]<br />
• IV: distant metastasis (excludes peritoneal metastasis)<br />
to liver parenchyma or malignant pleural effusion<br />
(Lung> liver)
• Debulking surgery (Cytoreduction) = _____
• Primary goal [2003, 2005]<br />
– resection of disease (移除所有可切除的病變)<br />
– organ resection, if necessary<br />
• Secondary goal<br />
– optimal debulking<br />
– removal of as much tumor as possible<br />
– surgical cytoreduction (C/T)<br />
– optimal &. suboptimal (1 cm)
• Preserve fertility<br />
– stage IA/IB, grade 1/grade 2, non-clear cell<br />
type<br />
– unilateral salpingo-oophorectomy +<br />
PALNS+unilateral PLND+<br />
appendectomy+omentectomy<br />
– no marked lesion over another ovary<br />
– hold wedge resection<br />
– bilateral ovarian cancer: both resection<br />
– uterus: hysteroscopy + curettage
• Prognosis<br />
–Stage<br />
• I 5-year survival:85-90%<br />
• II 5-year survival:80%<br />
• III 5-year survival:15-20%<br />
• IV 5-year survival:5%<br />
– Suboptimal &. optimal debulking<br />
• 5-year survival:10-20% vs 30-50% (
• Chemotherapy [2003, 2004, 2005]<br />
– Paclitaxel + cisplatin/ carboplatin (T+P)<br />
– Cyclophosphamide + cisplatin/ carboplatin (C+P)<br />
– Bleomycin+Etoposide+Cisplatin (germ cell ov ca)<br />
(BEP)<br />
• Paclitaxel 175mg/m2, 3hrs 135mg/m2, 24hrs<br />
• Cisplatin 50mg/m2<br />
• Doxorubicin 50mg/m2<br />
• Carboplatin AUC 4-5 or 5 –6<br />
• Cyclophosphamide 600-750mg/m2<br />
• Q3wks x 6 cycles<br />
• IP (Intra-peritoneal C/T)<br />
• IA/IB, grade 1: obs.<br />
• IA/IB, grade 2: obs. or 3-6 C/T<br />
• IC/ grade 3/ clear cell ca: 3-6 C/T<br />
• 2nd debulking . 2nd looking operation [1996]
• [2007] 下列何因素不會增加卵巢癌的危險?<br />
– 初經來得早.<br />
– 停經時間較晚<br />
– 使用口服避孕藥<br />
– 低胎次(low parity)<br />
• [2007] 卵巢癌最常見的組織型態為:<br />
– 漿液性(serous).<br />
– 黏液性(mucinous)<br />
– 子宮內膜樣<br />
(endometrioid).<br />
– 亮細胞(clear cell)<br />
• [?] 62 y/o, 停經 11 yrs, 6 cm ov tumor-> 血流,CA-125,colonoscopy<br />
(tumor aspiration for biopsy xxxxxx)
Other ovarian tumor<br />
• Dysgerminoma<br />
– Bilateral: 10-15%<br />
– Radiosensitive -> R/T<br />
– Most ov. ca. associated with pregnancy<br />
• Teratoma<br />
– Immature: neural tissue ~ grade 1-3<br />
– Malignant transformation: SCC: 1~3 %<br />
• Endodermal sinus tumor (EST): yolk sac<br />
– Very malignancy<br />
– Always unilateral side [1998] 對側 xxxx<br />
– Schllier-Duval body (中間一小血管被腫瘤細胞包圍著)<br />
– Conservative DB + adjuvant C/T (60~70%)<br />
• Sexual cord stromal tumor [1998]有何種類,分類<br />
– 1.Granulosa-stromal tumor: 25% EM hyperplasia, 5% EM ca.<br />
– 2.Sertoil-leydig cell tumor (androblastoma).<br />
– 3.Thecoma. 4.Hilus cell tumor. 5.Gonadoblastoma.<br />
[2002] 17 y/o, right ovarian<br />
tumor (7 cm), biopsy:<br />
schiller-duval body<br />
[2005]