Community Wards (Beverley, Hornsea, Withernsea) Guideline for ...
Community Wards (Beverley, Hornsea, Withernsea) Guideline for ...
Community Wards (Beverley, Hornsea, Withernsea) Guideline for ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Community</strong> <strong>Wards</strong><br />
(<strong>Beverley</strong>, <strong>Hornsea</strong>, <strong>Withernsea</strong>) <strong>Guideline</strong> <strong>for</strong><br />
the use of Patients’ Own Drugs (PODs) and<br />
Medicines Reconciliation.<br />
If your first language is not English, or if you would like this<br />
document in a <strong>for</strong>mat <strong>for</strong> people who are blind or have visual<br />
problems, we can make arrangements to help you.<br />
Please contact<br />
Phone:<br />
Textphone:<br />
Head of Quality and Risk<br />
01377 208802<br />
01482 315747<br />
Nëse dëshironi ndihmë me këtë dokument, ju lutemi telefononi 01430 457351<br />
Eğer bu döküman ile ilgili olarak yardım istiyorsanız, lütfen 01430 457353 numaralı<br />
telefonu arayınız.<br />
Potrzebujesz pomocy w zrozumieniu tego dokumentu? Zatelefonuj pod 01430<br />
457367<br />
Ref No CP59<br />
Version 2<br />
Ratified by: Evidence Based Practice Group<br />
Date ratified: 14 th September 2009<br />
Name of Author: Fiona Hammond, Ann Wetherill, Di Ledger<br />
Director: Director of Quality & Professional Services<br />
(Executive Nurse)<br />
Date Issued: 1st July 2009<br />
Review Date: September 2011<br />
VALIDITY STATEMENT<br />
Only the electronic copy of this document is guaranteed to be the currently<br />
valid version. Downloaded versions must be regularly checked <strong>for</strong> validity,<br />
this is the responsibility of the individual user.<br />
Page 1 of 23
CONTROL SHEET<br />
<strong>Guideline</strong>s Title: <strong>Community</strong> <strong>Wards</strong> <strong>Guideline</strong>s <strong>for</strong> the use of Patients’<br />
Own drugs (PODs)<br />
Intended Recipients: <strong>Community</strong> wards, Locality Matrons, Prescribers<br />
<strong>for</strong> the community wards in <strong>Beverley</strong>, <strong>Hornsea</strong> and <strong>Withernsea</strong>.<br />
Is the <strong>Guideline</strong> new or<br />
<strong>for</strong> review?<br />
New: Yes Review:<br />
Name of co-authors/contributors: Fiona Hammond, Ann Wetherill and<br />
Di Ledger<br />
Contributions from Jackie Matthews and Nick Borrill<br />
Name of Sponsoring Executive: N/A<br />
Training/Resource implications: Training provided by community<br />
services medicines management team.<br />
Audit/Monitoring Arrangements: Monitoring conducted by the<br />
community services medicines management team. Audit conducted as<br />
per the clinical audit annual plan.<br />
Reviewed by Evidence Based<br />
Practice Group<br />
Date: 14 th September 2009<br />
Approved by Medicines<br />
Management Group<br />
Date: 17/3/2010<br />
All new Policies need <strong>Community</strong><br />
Services Committee/Board approval<br />
Date: N/A<br />
Implementation Date: 1 st July 2009<br />
Review Date: September 2011<br />
Name of the person responsible <strong>for</strong> the review: Fiona Hammond<br />
How will this protocol be disseminated? Via Team Brief. Copy to be<br />
placed on the Trust Web-site and on Policy Data base on the V Drive<br />
Indicate where the protocol will be<br />
stored<br />
Has an equality assessment been<br />
carried out?<br />
V drive<br />
Yes<br />
Page 2 of 23
CONTENTS<br />
1. Introduction 4<br />
2. Definitions 4<br />
3. Scope 4<br />
4. Equality and Diversity 5<br />
5. Roles and Responsibilities 5<br />
6. Training 6<br />
7. Procedure <strong>for</strong> the use of patients’ own drugs (PODS) 6<br />
7.1 On admission (Collection & Checking)<br />
7.2 Use of POD’s at NHS East Riding of Yorkshire<br />
<strong>Community</strong> Hospitals<br />
7.3 Ordering further supplies<br />
7.4 Patients’ own controlled drugs<br />
7.5 Discharge with POD’s<br />
8. Communication and Documentation 10<br />
9. Risk Management 11<br />
10. Monitoring and Audit 12<br />
11. Implementation 13<br />
12. References 13<br />
Appendices:<br />
A. Patient consent <strong>for</strong>m<br />
B. Criteria <strong>for</strong> assessing PODs<br />
C. POD’s medication checklist<br />
D. Medication destruction <strong>for</strong>m<br />
E. Patient discharge leaflet<br />
F. Employee record<br />
Page 3 of 23
1. INTRODUCTION<br />
The implementation of Patients’ own drug (POD’s) processes was<br />
recommended by the Audit Commission in the document “Spoonful of<br />
Sugar” and address a requirement of the National Service Framework<br />
(NSF) <strong>for</strong> Older People to introduce ‘one stop dispensing/dispensing <strong>for</strong><br />
discharge’ schemes. The process has been shown to reduce waste<br />
and be cost effective, in addition to improving medicines management<br />
by patients.<br />
This guideline has been produced to ensure the standardised, efficient<br />
and safe use of patients’ own drugs (POD’s) within <strong>Community</strong><br />
Hospitals in East Riding of Yorkshire <strong>Community</strong> Services, and that all<br />
medication a patient is currently taking is correctly documented on<br />
admission and at each transfer of care.<br />
All inpatients of the <strong>Community</strong> Hospital identified in the title will have<br />
any medicines they bring to the hospital assessed <strong>for</strong> suitability <strong>for</strong> use<br />
according to this protocol. It will be used in conjunction with NHS East<br />
Riding of Yorkshire <strong>Community</strong> Services Policy <strong>for</strong> the Management<br />
and Administration of Medicines and the Nursing and Midwifery Council<br />
(NMC) Code of Professional Conduct, <strong>Guideline</strong>s <strong>for</strong> Records and<br />
Record Keeping, Standards <strong>for</strong> Medicines Management, and<br />
<strong>Guideline</strong>s <strong>for</strong> the Administration of Medicines.<br />
2. DEFINITIONS<br />
Medicines reconciliation is a process designed to ensure that all<br />
medication a patient is currently taking is correctly documented on<br />
admission and at each transfer of care. It encompasses:<br />
• Collection of the medication history from a variety of sources<br />
(usually a minimum of 2).<br />
• Assessing concordance with treatment-as-prescribed prior to<br />
admission and identifying potential <strong>for</strong> partial or non-compliance.<br />
• Checking that medicines prescribed on admission <strong>for</strong> the patient<br />
are correct. The “checking” step involves ensuring that the<br />
medicines and doses that are now prescribed <strong>for</strong> the patient<br />
accurately reflect the sources consulted.<br />
• Communicating any changes in medicines so that they are<br />
readily available to the next person(s) caring <strong>for</strong> the patient.<br />
Communication must include reasons <strong>for</strong> the change(s) and any<br />
follow-up requirements. There must also be a written record in<br />
the patient’s medical record and/or on the prescription chart.<br />
Page 4 of 23
3. SCOPE<br />
This guidance should be used when a patient is admitted to an<br />
identified <strong>Community</strong> Hospital.<br />
This guidance promotes best practice relating to the use of Patients<br />
own drugs and is intended <strong>for</strong> use by all staff employed by <strong>Community</strong><br />
Services.<br />
The aim of this guidance is to;<br />
• Promote the use of POD’s which are both in good condition and<br />
are still appropriate <strong>for</strong> the patient’s treatment.<br />
• Avoid drug wastage, duplication of discharge medication,<br />
support self care, and improve a patient’s understanding of their<br />
medical condition.<br />
• May highlight problems with patients’ compliance which can be<br />
addressed to facilitate safe discharge and reduce unnecessary<br />
readmissions due to medicine related issues.<br />
4. EQUALITY AND DIVERSITY<br />
In developing this guidance, an equalities impact assessment has been<br />
undertaken. An adverse impact is unlikely, and on the contrary the<br />
procedure has the clear potential to have a positive impact by enabling<br />
improved communication between staff and patients, faster local<br />
system of medication procurement, waste management and reduction<br />
and an improved patient care and healthcare experience. If at any<br />
time, this guidance is considered to be discriminatory in any way, the<br />
author of the guidance should be contacted immediately to discuss<br />
these concerns.<br />
5. ROLES AND RESPONSIBILITIES<br />
5.1 Chief Executive<br />
The Chief Executive of the Trust has overall responsibility <strong>for</strong> the<br />
safe and secure handling of medicines by staff employed by<br />
<strong>Community</strong> Services.<br />
5.2 The Assistant Director <strong>for</strong> Medicines Management<br />
The Assistant Director <strong>for</strong> Medicines Management oversees the<br />
medicine management on behalf of the Chief Executive. This is<br />
managed in <strong>Community</strong> Services through an internal Service<br />
Level Agreement.<br />
5.3 <strong>Community</strong> Services Medicines Management Team<br />
Medicines reconciliation whenever and wherever possible<br />
should involve pharmacists and pharmacy technicians.<br />
Page 5 of 23
5.4 Managers<br />
The ward manager of the <strong>Community</strong> Hospital is responsible <strong>for</strong><br />
ensuring that all staff are aware of the guidance and follow its<br />
contents.<br />
It is the responsibility <strong>for</strong> managers to ensure that their staff are<br />
made aware of this guidance.<br />
It should be included in the local induction programme.<br />
It is the responsibility of a manager to identify to new staff, key<br />
aspects of the guidance which relate to their area of work.<br />
Managers will ensure that training needs <strong>for</strong> staff in medicine<br />
management are identified and delivered through the<br />
<strong>Community</strong> Services annual per<strong>for</strong>mance and development<br />
review linked to the Knowledge and Skills Framework.<br />
5.5 All Staff<br />
6. TRAINING<br />
Medicines Reconciliation is the responsibility of all staff involved<br />
in the admission, prescribing, monitoring, transfer and discharge<br />
of patients requiring medicines.<br />
The staff carrying out medicines reconciliation must be appropriately<br />
trained. The <strong>Community</strong> Services Medicines Management team have<br />
developed a training package which must be accessed by all<br />
healthcare staff involved in the Patient’s Own Drug process.<br />
It is the responsibility of a manager to identify to new staff, key aspects<br />
of the guidance which relate to their area of work. Training should be<br />
included in staff induction programmes.<br />
7. PROCEDURE FOR USING PATIENTS’ OWN DRUGS<br />
All patients admitted onto a community should be encouraged to bring<br />
their own medications into hospital.<br />
Medication brought onto a ward will be assessed by a registered nurse<br />
using the appropriate documentation and following the procedure laid<br />
out in Appendix B.<br />
Medication that is suitable and appropriate to the patient’s treatment<br />
can be used once a consent <strong>for</strong>m has been completed. (Appendix A)<br />
Page 6 of 23
7.1 On admission (Collection & Checking)<br />
The nurse should check that the patient has brought in their own<br />
medications and identify the medications condition. Ascertain<br />
how the patient has been taking the medication to assess<br />
partial/non-compliance.<br />
Every ef<strong>for</strong>t should be made to ensure that the patient has their<br />
own supply of medications when admitted onto the ward.<br />
If the patient has no medications with them or all of the patient’s<br />
medications are of poor condition then a new supply will need to<br />
be obtained.<br />
On occasions it may not be possible to get a full history from an<br />
unwell patient who may still require a prescription to be written.<br />
Every ef<strong>for</strong>t should be made to ensure that such a prescription is<br />
safe and appropriate to the needs of the patient and that a full<br />
history is obtained at the earliest opportunity. Details of the<br />
exceptional circumstance and subsequent decision to treat must<br />
be recorded in the patient’s notes.<br />
Explain the POD scheme to the patient.<br />
Obtain patient consent <strong>for</strong> POD’s use and destruction.<br />
(Appendix A).<br />
If the patient refuses or is unable to give consent <strong>for</strong> the POD’s<br />
to be used then a new supply of medications <strong>for</strong> use will need to<br />
be obtained.<br />
The nurse should assess the POD’s using the set criteria and<br />
checklist. (Appendix B). (Appendix C).<br />
Patients admitted may have been receiving their medication<br />
from a multi-dose compliance aid e.g. weekly NOMAD cassettes<br />
or monthly MANREX systems. These can be regarded as<br />
patients’ own medication only if they have been dispensed by a<br />
pharmacy and are sealed. Medication that has been put into<br />
cassettes by relatives or carers cannot be accepted as patients’<br />
own medication.<br />
For a POD to be acceptable it must satisfy all sections of<br />
the criteria.<br />
Review of medicines prescribed by a member of the pharmacy<br />
team. This should usually occur within 72 hours of admission.<br />
Page 7 of 23
7.2 Use of POD’s<br />
Any medication suitable <strong>for</strong> use should be labelled with a yellow<br />
sticker by the nurse. The nurse should then sign and date this<br />
sticker.<br />
Any queries that arise regarding the use of POD’s should be<br />
directed to the Medicines Management Team.<br />
Any remaining medicines that are deemed unsatisfactory <strong>for</strong> use<br />
should ideally be destroyed or returned to a community<br />
pharmacy <strong>for</strong> disposal. Details of any medications to be<br />
destroyed should be entered onto the medication destruction<br />
<strong>for</strong>m. (Appendix D). This <strong>for</strong>m should be signed by both the<br />
nurse and a witness to the destruction. If the patient does not<br />
consent to the medicines being destroyed the medications<br />
should be left in the patient locker clearly segregated from those<br />
to be used and clearly labelled “unsuitable <strong>for</strong> administration”.<br />
Where possible the patient’s relatives or representatives should<br />
be encouraged to take the medication home and return them to<br />
a community pharmacy <strong>for</strong> destruction, or disposal of in a DOOP<br />
bin.<br />
Any POD’s to be used should be stored in the patient’s<br />
individual bedside locker. Any medications that require special<br />
storage e.g. fridge items or controlled drugs need to be stored<br />
appropriately as per the policy <strong>for</strong> Medicines Management policy<br />
and a record made detailing their separate storage. If the locker<br />
is full the medication should then be stored in a designated area<br />
on the ward again recording the separate storage. All storage<br />
areas <strong>for</strong> POD’s should be kept locked and keys kept under the<br />
control of the ward manager.<br />
POD’s should never be administered to any other patient<br />
Only POD’s that have a signed yellow sticker and have been<br />
checked against the patient’s prescription can be administered.<br />
Any administration of medication will be recorded on the<br />
patient’s drug chart. Any administration of controlled drugs will<br />
also have to be recorded after each administration in the<br />
controlled drugs register in a separate POD’s section.<br />
Over the counter medications brought in by the patient should<br />
not be administered under a POD unless they have been<br />
prescribed by a doctor.<br />
If treatment is altered, POD’s should be re-labelled by a<br />
dispensing contractor. Alterations to labels and directions should<br />
Page 8 of 23
not be made by ward staff. If re-labelling is not possible the<br />
medication should be re-ordered using the ward FP10. Once this<br />
new supply of correctly labelled medication is received then the<br />
wrongly labelled medicine should be recorded onto the<br />
medication destruction <strong>for</strong>m then destroyed or returned to a<br />
community pharmacy <strong>for</strong> destruction.<br />
7.3 Ordering Further Supplies<br />
POD’s should be checked at least once weekly to determine the<br />
need <strong>for</strong> further supplies.<br />
If a further supply of medication is needed then the ward FP10<br />
prescriptions should be used. FP10s should be used to generate<br />
a prescription <strong>for</strong> the specific named patient at that ward<br />
address <strong>for</strong> the required medications and the supply obtained<br />
from a community pharmacy that is suitable <strong>for</strong> the patient.<br />
If a further supply is needed then all of the patient’s medications<br />
quantities should be assessed and if appropriate a single order<br />
placed. This will ensure the patient has enough <strong>for</strong> the inpatient<br />
stay and a supply <strong>for</strong> discharge.<br />
If the patient has a controlled drug on their drug chart this should<br />
be ordered via the same ward FP10 route.<br />
The ward should keep a record of FP10 usage. Recording the<br />
date, the prescription serial number, the prescribers name, the<br />
patient’s name and which medications have been ordered.<br />
If the patient is prescribed a RED drug, as classed by Hull &<br />
East Riding prescribing committee, then this drug will have to be<br />
obtained via the hospital specialist. If the patient is prescribed a<br />
clinical trial medication then this will have to be obtained via the<br />
clinical trial. (Never destroy clinical trial medication).<br />
When the further supplies are received onto the ward from the<br />
community pharmacy the medications should be checked<br />
against the wards record of the order then checked against the<br />
patient’s drug chart. Once medications have been checked as<br />
correct a signed and dated yellow sticker should be attached to<br />
each medication and then the medications should be placed into<br />
the patient’s individual locker, ensuring items requiring special<br />
storage are stored appropriately.<br />
7.4 Patients Own Controlled Drugs<br />
Any POD’s that are controlled drugs should be counted and<br />
recorded in the ward patients’ own controlled drugs register in<br />
Page 9 of 23
separate patient sections. These controlled drugs should then<br />
be stored in the ward patients’ own controlled drugs cabinet.<br />
Any POD’s that are controlled drugs deemed unsuitable <strong>for</strong> use<br />
should be recorded onto the medication destruction <strong>for</strong>m with a<br />
comment “awaiting CD destruction” as the controlled drugs will<br />
be destroyed at a later date by an authorised person.<br />
All POD’s that are controlled drugs <strong>for</strong> destruction should be<br />
recorded in the ward patients’ own controlled drug register and<br />
then destroyed by an authorised person and witnessed.<br />
Any POD’s that are controlled drugs awaiting destruction must<br />
be clearly labelled as “patient CD <strong>for</strong> destruction” and stored in<br />
the ward patients’ own controlled drugs cabinet and segregated<br />
from normal POD’s controlled drugs to avoid potential<br />
administration errors or re-use.<br />
7.5 Discharge with POD’s<br />
POD’s must never be returned to the patient on discharge<br />
without an assessment by a registered nurse or GP. This is to<br />
ensure that the POD’s returned are correct according to the<br />
patient’s prescription.<br />
Discharge should be with a minimum of 14 days supply.<br />
Any controlled drugs to be returned to the patient should be<br />
recorded in the wards patients’ own controlled drugs register<br />
under the separate patient section.<br />
The patient may be given a leaflet detailing their discharge<br />
prescription and details of where to obtain their next supply of<br />
medications. (Appendix E).<br />
A member of staff must check the locker is empty following<br />
discharge to ensure there is no risk of the next patient receiving<br />
incorrect medications.<br />
8. COMMUNICATION AND DOCUMENTATION<br />
Communicating is the final step in the process, where any changes that<br />
have been made to the patient’s prescription are documented and<br />
dated, ready to be communicated to the next person responsible <strong>for</strong> the<br />
medicines management care of that patient. Examples might include:<br />
• When a medicine has been stopped, and <strong>for</strong> what reason.<br />
• When a medicine has been started and <strong>for</strong> what reason.<br />
• The intended duration of treatment.<br />
• When a dose has been changed and <strong>for</strong> what reason.<br />
Page 10 of 23
8.1 Communication following admission.<br />
This is the responsibility of the admitting practitioner.<br />
• Documentation should always be made in the patient<br />
medical record, noting sources used and dated and signed<br />
by the admitting practitioner.<br />
• Prescription chart (list of medicines prescribed to be<br />
administered) annotated on the front at initial prescription to<br />
show “history taken, sources checked, the date and name of<br />
the practitioner”.<br />
• Intentional medication changes should always be<br />
documented in the patient medical record and on the<br />
prescription chart. Reasons <strong>for</strong> change should be<br />
documented in the medical record.<br />
• A summary of the actions as a result of the medicines<br />
reconciliation should be included.<br />
• Name, signature and contact details of the individual carrying<br />
out the reconciliation. Where changes have been made to<br />
the prescription chart these should also be appropriately<br />
documented.<br />
8. RISK MANAGEMENT<br />
8.1 Discrepancies<br />
Part of the checking process includes the identification of any<br />
discrepancies. A discrepancy can be defined as any difference<br />
between the medicines the patient had been taking in their<br />
previous care setting and the medicines prescribed in their new<br />
care setting.<br />
Discrepancies may be considered as:<br />
• Intentional<br />
• Unintentional<br />
Intentional discrepancies can be defined as any difference<br />
between the medicines the patient was taking prior to admission<br />
and the medicines prescribed in their new care setting that have<br />
been changed intentionally and agreed with the clinician(s)<br />
responsible <strong>for</strong> the patient’s care.<br />
Unintentional discrepancies (errors, omissions or unintentional<br />
additions) can be defined as any difference between the<br />
medicines the patient was taking prior to admission and the<br />
medicines prescribed in their new care setting that is not a<br />
conscious change.<br />
Page 11 of 23
8.2 Reconciling Discrepancies<br />
In the event that a discrepancy is discovered, healthcare staff<br />
must reconcile the discrepancy be<strong>for</strong>e administering medication.<br />
This may be by contact with the patient’s own GP Practice or the<br />
issuing hospital, <strong>for</strong> clarification.<br />
Unintentional medication changes should be discussed with the<br />
prescriber and documented in the patient’s medical record and<br />
(if appropriate) on the prescription chart with recommendations<br />
<strong>for</strong> follow up.<br />
An incident <strong>for</strong>m should be completed.<br />
8.3 Medication Errors<br />
If a medication error occurs related to the use of patients’ own<br />
drugs, the procedure outlined in NHS East Riding of Yorkshire<br />
PCT Policy <strong>for</strong> the Management and Administration of Medicines<br />
should be adhered to and a report made as per the Adverse<br />
Incident Reporting Policy and Procedures.<br />
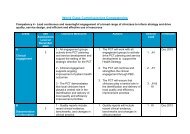
9. MONITORING AND AUDIT<br />
The patients’ own drug scheme will be evaluated using the following<br />
indicators:<br />
Monitoring will also be undertaken via adverse incident reports and an<br />
annual clinical audit. In addition the following may be implemented.<br />
• Number and percentage of patients’ using their own<br />
medication during their inpatient stay.<br />
• Number and percentage of patients’ own drugs not suitable <strong>for</strong> re-<br />
use and the reason why.<br />
• Drug expenditure by the community hospital and expenditure<br />
on medicines destroyed.<br />
10. IMPLEMENTATION<br />
This guideline will be shared with staff via Team Brief, the <strong>Community</strong><br />
Services intranet and the <strong>Community</strong> Services website.<br />
11. REFERENCES<br />
NPC, Medicines reconciliation, A guide to implementation.<br />
NICE in conjunction with NPSA, Technical patient safety solution <strong>for</strong><br />
medicines reconciliation on admission of adults to hospital, December<br />
2007.<br />
Page 12 of 23
Audit Commission, A spoonful of sugar – Medicines Management in<br />
NHS Hospitals.<br />
Page 13 of 23
Appendix A.<br />
Dear Patient,<br />
Page 14 of 23<br />
Attach addressograph or<br />
Name<br />
Address<br />
Date of Birth<br />
At NHS East Riding of Yorkshire <strong>Community</strong> Hospitals we operate a protocol of<br />
using your own medicines. This allows you to continue with familiar tablets and<br />
other treatments and helps to avoid waste.<br />
We will obtain supplies of any new medications you require from a local<br />
community pharmacy and when you go home we will ensure you receive a<br />
supply of all your current medications.<br />
Your medicines may be changed while you are here and there<strong>for</strong>e we may<br />
need to dispose of your old ones.<br />
If you are happy <strong>for</strong> us to use your medicines (<strong>for</strong> your treatment only), obtain<br />
supplies, and destroy any medication not suitable, please sign below.<br />
SIGNED ……………………………………………………….DATE………………..<br />
I confirm that I have explained the use and destruction of patients’ own drugs to<br />
this patient.<br />
Signature………………………………………………………………………………..<br />
Print Name………………………………………………………………………………<br />
Job title…………………………………………………………………………………..<br />
Date………………………………………………………………………………………
Appendix B.<br />
CRITERIA FOR ASSESSING PATIENTS’ OWN DRUGS (PODs)<br />
These criteria are intended to guide staff through the assessment of patients’ own<br />
drugs (PODs). For a POD to be suitable <strong>for</strong> use it must be acceptable in all of the<br />
following categories in both Sections A and B. If you are at all unsure about any<br />
of the PODs you are not under any obligation to sign that they are satisfactory, if<br />
you are unsure about any item obtain a new supply from a community pharmacy<br />
using the ward FP10. There may be circumstances where a POD is used but<br />
does not completely meet the criteria below. This should be at the nurse’s<br />
discretion and in agreement with the patient and also recorded into the patient’s<br />
records.<br />
Ensure patients are asked about the following:<br />
• Have they brought all of their currently prescribed medication with<br />
them?<br />
• Do they take the medication as prescribed? If not, how do they take<br />
it? (Concordance/Adherence)<br />
• Do they take any prn medication?<br />
• Other types of medication including:<br />
o Inhalers<br />
o Eye drops<br />
o Topical preparations<br />
o Once weekly medication e.g. methotrexate<br />
o Injections such as depot antipsychotics or vitamins<br />
o Oral contraceptives<br />
o Hormone replacement therapy<br />
o Nebules<br />
o Home oxygen<br />
o Insulin<br />
o Over the counter medication<br />
o Herbal preparations<br />
o Other non-prescribed medication<br />
Page 15 of 23
Section A. Checking the PODs Appendix B.<br />
CRITERIA USE IF MEDICATION IS: AVOID IF MEDICATION IS:<br />
Type of Product Oral, both solid or liquid<br />
Opened eye or ear preparations<br />
Topical, inhaled, or injected<br />
(unless it can be confirmed as<br />
Dressings, test strips, or ostomy<br />
opened less than one month ago)<br />
Suppository or pessary<br />
Over the counter medication (unless<br />
Unopened eye or ear preparations<br />
this has been prescribed)<br />
Presentation In a recognised medicine container<br />
Unrecognised contents or container<br />
Clean and dry<br />
Broken or damaged<br />
No signs of deterioration<br />
Dirty or damp packaging<br />
Liquids in original container<br />
Poor storage conditions or any signs<br />
of deterioration<br />
Any signs of contamination<br />
Age - Loose Dispensed within the last 3 months<br />
Dispensed more than 3 months ago<br />
tablets in bottles Clearly identifiable<br />
Unidentifiable<br />
Age - Blister<br />
packed tablets<br />
including<br />
Inhalers,<br />
creams &<br />
suppositories<br />
etc.<br />
The date is within the POD printed expiry<br />
date<br />
If no expiry date, then dispensed within the<br />
last 3 months<br />
Care with items requiring special storage<br />
conditions e.g. Insulin<br />
Care with items with a shortened expiry<br />
once opened e.g. GTN tablets<br />
Page 16 of 23<br />
POD is past it’s expiry date<br />
If no expiry date, dispensed more<br />
than 3 months ago or unclear when<br />
dispensed<br />
Unconfirmed or inappropriate<br />
storage conditions<br />
Unclear opening date of products<br />
with shortened expiry once opened
Section A. Checking the PODs Appendix B.<br />
CRITERIA<br />
Age – Monitored<br />
dosage systems<br />
(MDS)<br />
Age – liquids<br />
USE IF MEDICATION IS: AVOID IF MEDICATION IS:<br />
Sealed and filled by a pharmacy<br />
If weekly box – filled within last month<br />
If monthly box – filled within last 2 months<br />
Unchanged since last filled<br />
Page 17 of 23<br />
Not sealed or not filled by a<br />
pharmacy<br />
Filled longer than 1 month <strong>for</strong><br />
weekly boxes or 2 months <strong>for</strong><br />
monthly boxes<br />
No indication of when it was filled<br />
Any changes to medications since<br />
last filled<br />
Dispensed within last 3 months Dispensed more than 3 months ago<br />
Label The POD has the correct patient name on<br />
the label<br />
The POD has the correct drug name, <strong>for</strong>m<br />
and strength on the label<br />
There are instructions on how to take the<br />
POD which match the prescriber’s<br />
prescription<br />
For MDS – must be satisfied that the filled<br />
tablets match the doses and frequencies on<br />
the accompanying sheet or labels<br />
Identity The name of the drug, <strong>for</strong>m and strength<br />
matches that of the blister strip or<br />
packaging<br />
The POD has any other patients<br />
name on the label<br />
The POD does not have the correct<br />
drug name, <strong>for</strong>m or strength on the<br />
label<br />
The POD has unacceptable hand<br />
written annotations on the label or<br />
instructions do not match the<br />
prescriber’s prescription<br />
The suppliers name & address<br />
cannot be identified<br />
Not possible to identify the product<br />
by it’s packaging<br />
Boxes containing mixed contents or<br />
quantities greater than originally<br />
dispensed
Appendix B.<br />
Section B. Checking the PODs against the Drug Chart<br />
Be<strong>for</strong>e the PODs are used they should be checked against the drug chart. To do this, have each item present and check the drug name,<br />
<strong>for</strong>m, strength and dose frequency against the prescription. If there are any discrepancies check with the prescriber and if necessary get<br />
a new supply of the medication(s) via a ward FP10 from a community pharmacy.<br />
The prescriber producing the drug chart should check that the medicines prescribed on admission correspond to those taken prior to<br />
admission.<br />
If there are any discrepancies check with the patient’s discharging hospital or the patient’s own GP.<br />
Page 18 of 23
Medication name,<br />
strength and <strong>for</strong>m<br />
Appendix C.<br />
PODs Medication Checklist<br />
Enter the name of the medication, strength, <strong>for</strong>m, and quantity and expiry date.<br />
Place a √ or a X in the appropriate categories.<br />
A box is provided <strong>for</strong> any other comments.<br />
Attach addressograph or<br />
Name<br />
Address<br />
Date of Birth<br />
Quantity Expiry<br />
date<br />
Good<br />
Condition?<br />
Page 19 of 23<br />
Correct<br />
Instructions?<br />
Suitable<br />
<strong>for</strong> use?<br />
Assessed by …………………………………………………………….. Date……………………<br />
Other comments
Appendix D.<br />
Medication name,<br />
strength and <strong>for</strong>m<br />
PODs Medication destruction <strong>for</strong>m<br />
Attach addressograph or<br />
Name<br />
Address<br />
Date of Birth<br />
Quantity Reason <strong>for</strong><br />
destruction<br />
Page 20 of 23<br />
Comments Destroyed<br />
by:<br />
signature<br />
and date<br />
NOTE: PODs controlled drugs will be destroyed by an authorised person and also recorded<br />
in the patients’ own controlled drug register.<br />
Witnessed<br />
by:<br />
signature<br />
and date
Appendix E.<br />
The community ward gave you at least 14 days supply of your current<br />
medications. Further supplies need to be ordered from your own doctor.<br />
The hospital will send your doctor a list of your current medicines.<br />
Any unwanted medications should be returned to your community pharmacist<br />
<strong>for</strong> safe disposal.<br />
If you have any questions about your medications ask your doctor or<br />
pharmacist.<br />
Page 21 of 23
Patients Name………………………………………………………………….. Date ………………..<br />
Doctor/Surgery…………………………………………………………………<br />
NAME &<br />
STRENGTH<br />
OF<br />
MEDICINE<br />
BREAKFAST<br />
NUMBER OF TABLETS TO TAKE<br />
LUNCH<br />
TEA<br />
Page 22 of 23<br />
BEDTIME<br />
USE AND ACTION
Appendix F.<br />
Title of <strong>Guideline</strong>:<br />
EMPLOYEE RECORD OF HAVING READ THE GUIDANCE<br />
<strong>Community</strong> <strong>Wards</strong> <strong>Guideline</strong> <strong>for</strong> the use of patients’ own drugs (PODs)<br />
I have read and understand the procedures contained in the named <strong>Guideline</strong>.<br />
PRINT FULL NAME<br />
SIGNATURE<br />
DATE<br />
Page 23 of 23