082098 Staphylococcus aureus Infections - Goodsamim.com
082098 Staphylococcus aureus Infections - Goodsamim.com
082098 Staphylococcus aureus Infections - Goodsamim.com

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
MEDICAL PROGRESS<br />
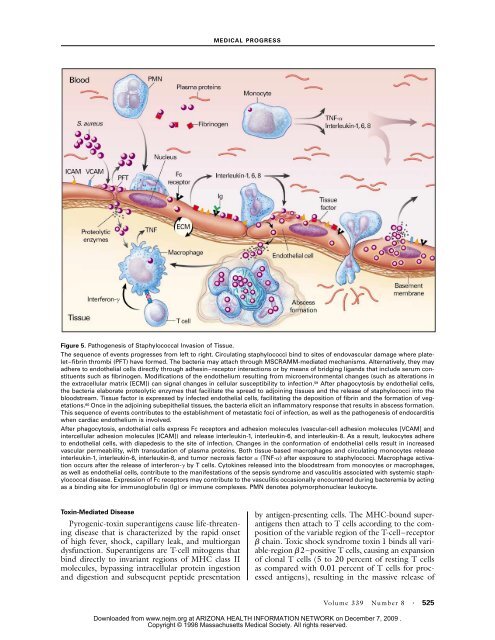
Figure 5. Pathogenesis of Staphylococcal Invasion of Tissue.<br />
The sequence of events progresses from left to right. Circulating staphylococci bind to sites of endovascular damage where platelet–fibrin<br />
thrombi (PFT) have formed. The bacteria may attach through MSCRAMM-mediated mechanisms. Alternatively, they may<br />
adhere to endothelial cells directly through adhesin–receptor interactions or by means of bridging ligands that include serum constituents<br />
such as fibrinogen. Modifications of the endothelium resulting from microenvironmental changes (such as alterations in<br />
the extracellular matrix [ECM]) can signal changes in cellular susceptibility to infection. 59 After phagocytosis by endothelial cells,<br />
the bacteria elaborate proteolytic enzymes that facilitate the spread to adjoining tissues and the release of staphylococci into the<br />
bloodstream. Tissue factor is expressed by infected endothelial cells, facilitating the deposition of fibrin and the formation of vegetations.<br />
60 Once in the adjoining subepithelial tissues, the bacteria elicit an inflammatory response that results in abscess formation.<br />
This sequence of events contributes to the establishment of metastatic foci of infection, as well as the pathogenesis of endocarditis<br />
when cardiac endothelium is involved.<br />
After phagocytosis, endothelial cells express Fc receptors and adhesion molecules (vascular-cell adhesion molecules [VCAM] and<br />
intercellular adhesion molecules [ICAM]) and release interleukin-1, interleukin-6, and interleukin-8. As a result, leukocytes adhere<br />
to endothelial cells, with diapedesis to the site of infection. Changes in the conformation of endothelial cells result in increased<br />
vascular permeability, with transudation of plasma proteins. Both tissue-based macrophages and circulating monocytes release<br />
interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor a (TNF-a) after exposure to staphylococci. Macrophage activation<br />
occurs after the release of interferon-g by T cells. Cytokines released into the bloodstream from monocytes or macrophages,<br />
as well as endothelial cells, contribute to the manifestations of the sepsis syndrome and vasculitis associated with systemic staphylococcal<br />
disease. Expression of Fc receptors may contribute to the vasculitis occasionally encountered during bacteremia by acting<br />
as a binding site for immunoglobulin (Ig) or immune <strong>com</strong>plexes. PMN denotes polymorphonuclear leukocyte.<br />
Toxin-Mediated Disease<br />
Pyrogenic-toxin superantigens cause life-threatening<br />
disease that is characterized by the rapid onset<br />
of high fever, shock, capillary leak, and multiorgan<br />
dysfunction. Superantigens are T-cell mitogens that<br />
bind directly to invariant regions of MHC class II<br />
molecules, bypassing intracellular protein ingestion<br />
and digestion and subsequent peptide presentation<br />
by antigen-presenting cells. The MHC-bound superantigens<br />
then attach to T cells according to the <strong>com</strong>position<br />
of the variable region of the T-cell–receptor<br />
b chain. Toxic shock syndrome toxin 1 binds all variable-region<br />
b2–positive T cells, causing an expansion<br />
of clonal T cells (5 to 20 percent of resting T cells<br />
as <strong>com</strong>pared with 0.01 percent of T cells for processed<br />
antigens), resulting in the massive release of<br />
Volume 339 Number 8 · 525<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.