082098 Staphylococcus aureus Infections - Goodsamim.com
082098 Staphylococcus aureus Infections - Goodsamim.com
082098 Staphylococcus aureus Infections - Goodsamim.com

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
The New England Journal of Medicine<br />
Review Articles<br />
Medical Progress<br />
STAPHYLOCOCCUS AUREUS INFECTIONS<br />
FRANKLIN D. LOWY, M.D.<br />
Micrococcus, which, when limited in its extent and activity,<br />
causes acute suppurative inflammation (phlegmon), produces,<br />
when more extensive and intense in its action on<br />
the human system, the most virulent forms of septicæmia<br />
and pyæmia. 1<br />
IN an elegant series of clinical observations and<br />
laboratory studies published in 1880 and 1882,<br />
Ogston described staphylococcal disease and its<br />
role in sepsis and abscess formation. 1,2 More than 100<br />
years later, <strong>Staphylococcus</strong> <strong>aureus</strong> remains a versatile<br />
and dangerous pathogen in humans. The frequencies<br />
of both <strong>com</strong>munity-acquired and hospital-acquired<br />
staphylococcal infections have increased steadily, with<br />
little change in overall mortality. Treatment of these<br />
infections has be<strong>com</strong>e more difficult because of the<br />
emergence of multidrug-resistant strains. This review<br />
focuses on developments in our understanding of the<br />
pathogenesis, epidemiology, and management of lifethreatening<br />
staphylococcal disease since this topic was<br />
last examined in the Journal. 3,4<br />
STAPHYLOCOCCAL COMPONENTS<br />
AND PRODUCTS<br />
S. <strong>aureus</strong> is a member of the Micrococcaceae family<br />
(Fig. 1). On microscopical examination, the organisms<br />
appear as gram-positive cocci in clusters (Fig.<br />
2). S. <strong>aureus</strong> is distinguished from other staphylococcal<br />
species on the basis of the gold pigmentation of<br />
colonies and positive results of coagulase, mannitolfermentation,<br />
and deoxyribonuclease tests. 5<br />
Genome<br />
The staphylococcal genome consists of a circular<br />
chromosome (of approximately 2800 bp), with prophages,<br />
plasmids, and transposons. Genes governing<br />
virulence and resistance to antibiotics are found on<br />
From the Division of Infectious Diseases, Department of Medicine,<br />
Montefiore Medical Center, and the Departments of Medicine, Microbiology,<br />
and Immunology, Albert Einstein College of Medicine — both in<br />
Bronx, N.Y. Address reprint requests to Dr. Lowy at the Department of<br />
Medicine, Montefiore Medical Center, 111 E. 210th St., Bronx, NY 10467.<br />
©1998, Massachusetts Medical Society.<br />
the chromosome, as well as the extrachromosomal elements.<br />
6 These genes are transferred between staphylococcal<br />
strains, species, or other gram-positive bacterial<br />
species through the extrachromosomal elements. 7<br />
Cell Wall<br />
The staphylococcal cell wall is 50 percent peptidoglycan<br />
by weight. Peptidoglycan consists of alternating<br />
polysaccharide subunits of N-acetylglucosamine<br />
and N-acetylmuramic acid with 1,4-b linkages.<br />
The peptidoglycan chains are cross-linked by tetrapeptide<br />
chains bound to N-acetylmuramic acid and<br />
by a pentaglycine bridge specific for S. <strong>aureus</strong>. Peptidoglycan<br />
may have endotoxin-like activity, stimulating<br />
the release of cytokines by macrophages, activation<br />
of <strong>com</strong>plement, and aggregation of platelets.<br />
Differences in the peptidoglycan structure of staphylococcal<br />
strains may contribute to variations in their<br />
capacity to cause disseminated intravascular coagulation.<br />
8 Ribitol teichoic acids, covalently bound to peptidoglycan,<br />
are major constituents of the cell wall.<br />
Lipoteichoic acid is a glycerol phosphate polymer<br />
linked to a glycolipid terminus anchored in the cytoplasmic<br />
membrane.<br />
Capsule<br />
Most staphylococci produce microcapsules. Of<br />
the 11 types of microcapsular polysaccharide serotypes<br />
that have been identified, types 5 and 8 account<br />
for 75 percent of human infections. Most<br />
methicillin-resistant S. <strong>aureus</strong> isolates are type 5. The<br />
chemical <strong>com</strong>position of four of these antiphagocytic<br />
polysaccharides, including types 5 and 8, has been<br />
determined, and all four have been shown to be<br />
chemically related. 9<br />
Surface Proteins<br />
Many staphylococcal surface proteins have certain<br />
structural features in <strong>com</strong>mon. These features include<br />
a secretory signal sequence at the N terminal, positively<br />
charged amino acids that extend into the cytoplasm,<br />
a hydrophobic membrane-spanning domain,<br />
and a cell-wall–anchoring region, all at the carboxyl<br />
terminal. A ligand-binding domain at the N terminal<br />
that is exposed on the surface of the bacterial cell enables<br />
some of these proteins to function as adhesins. 10<br />
Protein A, the prototype of these proteins, has antiphagocytic<br />
properties that are based on its ability to<br />
bind the Fc portion of immunoglobulin (Fig. 1).<br />
Several of these related proteins bind extracellularmatrix<br />
molecules and have been designated microbialsurface<br />
<strong>com</strong>ponents recognizing adhesive matrix<br />
molecules (MSCRAMM). Recent studies suggest<br />
520 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
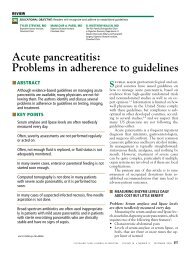
Figure 1. Structure of S. <strong>aureus</strong>.<br />
Panel A shows the surface and secreted proteins. The synthesis of many of these proteins is dependent on the growth phase, as<br />
shown by the graph, and is controlled by regulatory genes such as agr. Panels B and C show cross sections of the cell envelope.<br />
Many of the surface proteins have a structural organization similar to that of clumping factor, including repeated segments of amino<br />
acids (Panel C). TSST-1 denotes toxic shock syndrome toxin 1.<br />
that these proteins play an important part in the ability<br />
of staphylococci to colonize host tissue. 11<br />
Toxins<br />
Staphylococci produce numerous toxins that are<br />
grouped on the basis of their mechanisms of action.<br />
Cytotoxins, such as the 33-kd protein-alpha toxin,<br />
cause pore formation and induce proinflammatory<br />
changes in mammalian cells. The consequent cellular<br />
damage may contribute to manifestations of the<br />
sepsis syndrome. 12,13 The pyrogenic-toxin superantigens<br />
are structurally related, sharing various degrees<br />
of amino acid sequence homology. They function as<br />
superantigens by binding to major histo<strong>com</strong>patibility<br />
<strong>com</strong>plex (MHC) class II proteins, causing extensive<br />
T-cell proliferation and cytokine release. 14 Different<br />
domains of the enterotoxin molecule are responsible<br />
for the two diseases caused by these proteins, the<br />
toxic shock syndrome and food poisoning. 15 Despite<br />
little amino acid sequence homology, toxic shock<br />
syndrome toxin 1 is structurally similar to enterotoxins<br />
B and C. The gene for toxic shock syndrome toxin<br />
1 is found in 20 percent of S. <strong>aureus</strong> isolates. 14<br />
The exfoliative toxins, including epidermolytic toxins<br />
A and B, cause skin erythema and separation, as<br />
seen in the staphylococcal scalded skin syndrome.<br />
The mechanism of action of these toxins remains<br />
controversial. Panton–Valentine leukocidin is a leukocytolytic<br />
toxin that has been epidemiologically associated<br />
with severe cutaneous infections. 16<br />
Enzymes and Other Bacterial Components<br />
Staphylococci produce various enzymes, such as<br />
protease, lipase, and hyaluronidase, that destroy tissue.<br />
These bacterial products may facilitate the spread<br />
of infection to adjoining tissues, although their role<br />
in the pathogenesis of disease is not well defined.<br />
b-Lactamase is an enzyme that inactivates penicillin.<br />
Penicillin-binding proteins are enzymes located<br />
in the cytoplasmic membrane that are involved in<br />
cell-wall assembly. 5 A novel penicillin-binding protein<br />
is responsible for staphylococcal resistance to the<br />
penicillinase-resistant penicillins and cephalosporins.<br />
Coagulase, a prothrombin activator, converts fibrinogen<br />
to fibrin. Its contribution to bacterial virulence<br />
is uncertain.<br />
Volume 339 Number 8 · 521<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
EPIDEMIOLOGY OF STAPHYLOCOCCAL<br />
DISEASE<br />
Colonization and Infection<br />
Humans are a natural reservoir of S. <strong>aureus</strong>. Thirty<br />
to 50 percent of healthy adults are colonized, with<br />
10 to 20 percent persistently colonized. 21,22 Both<br />
methicillin-sensitive and methicillin-resistant isolates<br />
are persistent colonizers. 22,23 Persons colonized with<br />
S. <strong>aureus</strong> are at increased risk for subsequent infections.<br />
24 Rates of staphylococcal colonization are high<br />
among patients with type 1 diabetes, 25 intravenous<br />
drug users, 26 patients undergoing hemodialysis, 27<br />
surgical patients, 28,29 and patients with the acquired<br />
immunodeficiency syndrome. 30 Patients with qualitative<br />
or quantitative defects in leukocyte function<br />
are also at increased risk for staphylococcal disease. 31<br />
Transmission<br />
Persons colonized with S. <strong>aureus</strong> strains are at increased<br />
risk of be<strong>com</strong>ing infected with these strains.<br />
Most cases of noso<strong>com</strong>ial infection are acquired<br />
through exposure to the hands of health care workers<br />
after they have been transiently colonized with<br />
staphylococci from their own reservoir or from contact<br />
with an infected patient. Outbreaks may also result<br />
from exposure to a single long-term carrier or<br />
environmental sources, but these modes of transmission<br />
are less <strong>com</strong>mon. 22,32<br />
Figure 2. Staphylococci with Polymorphonuclear Leukocytes in<br />
a Sputum Sample (Gram’s Stain, ¬1000).<br />
Genetic Regulation of Virulence-Determinant Expression<br />
Global regulatory genes that coordinate the expression<br />
of various groups of staphylococcal genes<br />
have been identified. 17,18 The most extensively studied<br />
gene, agr, induces the expression of exoprotein<br />
(extracellular protein) while suppressing the expression<br />
of surface protein through a bacterial-density–<br />
sensing octapeptide. 19 Surface proteins are predominantly<br />
synthesized during the exponential growth<br />
phase, and the secreted proteins are synthesized during<br />
the stationary phase (Fig. 1A). This sequential<br />
expression of genes may have clinical importance.<br />
Different stages of staphylococcal infection appear<br />
to require different panels of virulence determinants.<br />
During the initial stages of infection, the expression<br />
of surface proteins that bind extracellular-matrix molecules<br />
favors successful colonization of host tissues,<br />
whereas the synthesis of exoproteins favors the spread<br />
to adjacent tissues. This hypothesis is supported by<br />
studies in animals showing that the inactivation of<br />
regulatory genes reduces bacterial virulence. 20<br />
Temporal Trends in S. <strong>aureus</strong> Disease<br />
The numbers of both <strong>com</strong>munity-acquired and<br />
hospital-acquired staphylococcal infections have increased<br />
in the past 20 years. This trend parallels the<br />
increased use of intravascular devices. 33,34 During<br />
the period from 1990 through 1992, S. <strong>aureus</strong> was<br />
the most <strong>com</strong>mon cause of noso<strong>com</strong>ial cases of pneumonia<br />
and surgical-wound infections and the second<br />
most <strong>com</strong>mon cause (after coagulase-negative staphylococci)<br />
of noso<strong>com</strong>ial bloodstream infections, according<br />
to data from the National Noso<strong>com</strong>ial <strong>Infections</strong><br />
Surveillance system of the Centers for Disease<br />
Control and Prevention (CDC). 35<br />
A second trend, resulting in part from selective<br />
antibiotic pressure, has been the dramatic worldwide<br />
increase in the proportion of infections caused by<br />
methicillin-resistant S. <strong>aureus</strong>. 36,37 Initially noted in<br />
tertiary care hospitals, methicillin-resistant strains<br />
are increasingly found in the <strong>com</strong>munity. 38 Data<br />
from the National Noso<strong>com</strong>ial <strong>Infections</strong> Surveillance<br />
system for the period from 1987 to 1997 show<br />
that the number of methicillin-resistant S. <strong>aureus</strong> infections<br />
in intensive care units has continued to increase<br />
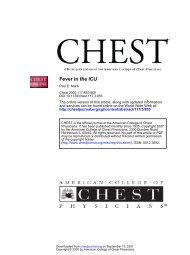
(Fig. 3). Methicillin-resistant strains have also<br />
be<strong>com</strong>e resistant to other antimicrobial agents. 37<br />
The same 10-year CDC survey showed that the proportion<br />
of methicillin-resistant isolates with sensitivity<br />
only to van<strong>com</strong>ycin increased from 22.8 percent<br />
522 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
No. of <strong>Infections</strong><br />
3000<br />
2000<br />
1000<br />
0<br />
1987<br />
No. of infections<br />
Percent of infections resistant to methicillin<br />
Percent of methicillin-resistant infections<br />
sensitive only to van<strong>com</strong>ycin<br />
1988<br />
1989<br />
1990<br />
1991<br />
1992<br />
Year<br />
1993<br />
1994<br />
1995<br />
1996<br />
1997<br />
Figure 3. S. <strong>aureus</strong> <strong>Infections</strong> in Intensive Care Units in the<br />
National Noso<strong>com</strong>ial <strong>Infections</strong> Surveillance System, 1987<br />
through 1997.<br />
Data include total infections, infections with methicillin-resistant<br />
strains, and infections with methicillin-resistant strains sensitive<br />
only to van<strong>com</strong>ycin. Isolates were tested for sensitivity to<br />
the following antimicrobial agents: gentamicin, tobramycin,<br />
amikacin, ciprofloxacin, clindamycin, erythromycin, chloramphenicol,<br />
trimethoprim–sulfamethoxazole, and van<strong>com</strong>ycin.<br />
Some hospitals did not test for susceptibility to all these antibiotics.<br />
Data were kindly provided by Dr. Robert Gaynes, Hospital<br />
Infection Program, National Center for Infectious Diseases.<br />
in 1987 to 56.2 percent in 1997 (Fig. 3). These isolates<br />
constitute the subgroup of strains from which<br />
the S. <strong>aureus</strong> strains with intermediate sensitivity to<br />
van<strong>com</strong>ycin (glycopeptide-intermediate S. <strong>aureus</strong>)<br />
have recently emerged. 39 New molecular typing techniques<br />
have clearly documented the ability of epidemic,<br />
disease-producing clones of methicillin-resistant<br />
S. <strong>aureus</strong> to populate hospitals and spread to<br />
diverse geographic regions rapidly. 40,41 The rapid<br />
spread and pathogenicity of these clones suggest<br />
that they possess unique, as yet undefined, determinants<br />
of virulence.<br />
PATHOGENESIS OF STAPHYLOCOCCAL<br />
DISEASE<br />
S. <strong>aureus</strong> has a diverse arsenal of <strong>com</strong>ponents and<br />
products that contribute to the pathogenesis of infection.<br />
These <strong>com</strong>ponents and products have overlapping<br />
roles and can act either in concert or alone.<br />
A great deal is known about the contribution of<br />
these bacterial factors to the development of infection.<br />
14,31,42,43 Considerably less is known about their<br />
80<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
Percent of <strong>Infections</strong><br />
interaction with each other and with host factors<br />
and their relative importance in infection.<br />
The virulence of S. <strong>aureus</strong> infection is remarkable,<br />
given that the organism is a <strong>com</strong>mensal that colonizes<br />
the nares, axillae, vagina, pharynx, or damaged skin<br />
surfaces. 21,22 <strong>Infections</strong> are initiated when a breach of<br />
the skin or mucosal barrier allows staphylococci access<br />
to adjoining tissues or the bloodstream. Whether an<br />
infection is contained or spreads depends on a <strong>com</strong>plex<br />
interplay between S. <strong>aureus</strong> virulence determinants<br />
and host defense mechanisms.<br />
The biology of colonization of the nares, the primary<br />
reservoir for staphylococci, is in<strong>com</strong>pletely<br />
understood. Mucin appears to be the critical host<br />
surface that is colonized in a process involving interactions<br />
between staphylococcal protein and mucin<br />
carbohydrate. 44,45 The role of other <strong>com</strong>mensals,<br />
secretory IgA, or specific staphylococcal adhesins is<br />
unknown.<br />
The risk of infection is increased by the presence<br />
of foreign material. Elek and Conen 46 first demonstrated<br />
the ability of sutures to reduce the threshold<br />
for infection. Several factors contribute to the increased<br />
susceptibility to infection. Phagocytic function<br />
in the presence of foreign material is seriously<br />
impaired. 47 Devices such as intravenous catheters are<br />
rapidly coated with serum constituents, such as<br />
fibrinogen or fibronectin, which enable staphylococci<br />
to adhere through MSCRAMM-mediated mechanisms<br />
and to elaborate glycocalices that further facilitate<br />
colonization. 48,49 Intravenous catheters are<br />
frequently implicated in the pathogenesis of noso<strong>com</strong>ial<br />
endocarditis. The introduction of long-term<br />
indwelling catheters has led to cases of noso<strong>com</strong>ial<br />
endocarditis that resemble the animal model of endocarditis.<br />
The catheter traumatizes the valvular surface,<br />
creating a nonbacterial thrombus on the cardiac<br />
valve that facilitates subsequent bacterial adherence. 50<br />
Invasive <strong>Infections</strong><br />
Staphylococcal bacteremia may be <strong>com</strong>plicated by<br />
endocarditis, metastatic infection, or the sepsis syndrome.<br />
The endothelial cell is central to these pathogenic<br />
processes. Not only is it a potential target for<br />
injury, but also its activation contributes to the progression<br />
of endovascular disease. Staphylococci avidly<br />
adhere to endothelial cells and bind through adhesin–receptor<br />
interactions. 51-53 In vitro studies demonstrate<br />
that after adherence, staphylococci are phagocytized<br />
by endothelial cells (Fig. 4). 52,55<br />
The intracellular environment protects staphylococci<br />
from host defense mechanisms as well as the<br />
bactericidal effects of antibiotics. Vesga et al. 56 demonstrated<br />
that the intraendothelial-cell milieu fosters<br />
the formation of small-colony variants. These factors<br />
may enhance bacterial survival and contribute to the<br />
development of persistent or recurrent infections. 57<br />
Staphylococcal strains that cause endocarditis are<br />
Volume 339 Number 8 · 523<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
Figure 4. Endothelial-Cell Phagocytosis of S. <strong>aureus</strong> in Vitro.<br />
The left-hand panel shows staphylococci after incubation with human umbilical-vein endothelial cells in tissue culture for 30<br />
minutes. The bacteria have been phagocytized, enclosed within membrane-bound vacuoles, and transported into the cell. The bar<br />
represents 0.5 µm. The right-hand panel shows an endothelial cell from a section of rabbit aorta incubated with staphylococci. The<br />
bacteria were incubated with tissue for 30 minutes and then incubated with medium for 5 1 /2 hours. The endothelial cell contains a<br />
large number of bacteria enclosed within vacuoles. The cell has ruptured, releasing bacteria into the medium. The bar represents<br />
1.0 µm. Reprinted from Lowy et al. 54 with the permission of the publisher.<br />
resistant to serum, adhere to both damaged and undamaged<br />
native valvular surfaces, are resistant to<br />
platelet microbicidal proteins, 58 and elaborate proteolytic<br />
enzymes that facilitate spread to adjacent tissues.<br />
5 The adherence of staphylococci to the platelet–fibrin<br />
thrombus that forms on damaged valvular<br />
surfaces may involve the adherence of MSCRAMM<br />
proteins to exposed matrix molecules. Staphylococcal<br />
endocarditis also occurs on undamaged valves.<br />
The invasion of endothelial cells by S. <strong>aureus</strong> may<br />
initiate the cellular alterations, including the expression<br />
of tissue factor, that promote the formation of<br />
vegetations (Fig. 5). 52,53,55,60,61<br />
The capacity to invade endovascular tissue also favors<br />
spread to other tissues. The tissue tropism of<br />
S. <strong>aureus</strong> cannot be explained solely on the basis of<br />
patterns of blood flow. MSCRAMM may mediate<br />
the adherence of staphylococci to exposed matrix<br />
molecules in the presence of endovascular injury, as<br />
a means of tissue invasion. Alternatively, staphylococci<br />
may bind endothelium directly. The potential<br />
role of MSCRAMM is best illustrated by collagenbinding<br />
protein. Its presence facilitates infection of<br />
bones and joints in animals. 62<br />
The cellular events leading to septic shock are similar<br />
in staphylococcal infection and infection with<br />
gram-negative bacteria. In both cases, monocytes<br />
and macrophages have a central role, although polymorphonuclear<br />
leukocytes, endothelial cells, and<br />
platelets also play a part. The monocytes release tumor<br />
necrosis factor a and interleukin-1, interleukin-6,<br />
and interleukin-8 after contact with intact staphylococci,<br />
peptidoglycan, or lipoteichoic acid. 63,64 In<br />
contrast, the expression of interleukin-1 and interleukin-6<br />
by endothelial cells requires bacterial phagocytosis.<br />
65 As a result of cytokine and cellular activation,<br />
the <strong>com</strong>plement and coagulation pathways are activated,<br />
arachidonic acid is metabolized, and plateletactivating<br />
factor is released. These events, in turn,<br />
cause fever, hypotension, capillary leak, disseminated<br />
intravascular coagulopathy, depression of myocardial<br />
function, and multiorgan dysfunction. Several staphylococcal<br />
<strong>com</strong>ponents appear to be capable of initiating<br />
the sepsis syndrome. 66 Peptidoglycan, especially<br />
when <strong>com</strong>bined with lipoteichoic acid, reproduces<br />
many of the physiologic responses of endotoxin in<br />
animal models of sepsis. 67,68 Alpha toxin alone reproduces<br />
many of the findings of sepsis, including<br />
hypotension, thrombocytopenia, and reduced oxygenation,<br />
in animal models. 12<br />
524 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
Figure 5. Pathogenesis of Staphylococcal Invasion of Tissue.<br />
The sequence of events progresses from left to right. Circulating staphylococci bind to sites of endovascular damage where platelet–fibrin<br />
thrombi (PFT) have formed. The bacteria may attach through MSCRAMM-mediated mechanisms. Alternatively, they may<br />
adhere to endothelial cells directly through adhesin–receptor interactions or by means of bridging ligands that include serum constituents<br />
such as fibrinogen. Modifications of the endothelium resulting from microenvironmental changes (such as alterations in<br />
the extracellular matrix [ECM]) can signal changes in cellular susceptibility to infection. 59 After phagocytosis by endothelial cells,<br />
the bacteria elaborate proteolytic enzymes that facilitate the spread to adjoining tissues and the release of staphylococci into the<br />
bloodstream. Tissue factor is expressed by infected endothelial cells, facilitating the deposition of fibrin and the formation of vegetations.<br />
60 Once in the adjoining subepithelial tissues, the bacteria elicit an inflammatory response that results in abscess formation.<br />
This sequence of events contributes to the establishment of metastatic foci of infection, as well as the pathogenesis of endocarditis<br />
when cardiac endothelium is involved.<br />
After phagocytosis, endothelial cells express Fc receptors and adhesion molecules (vascular-cell adhesion molecules [VCAM] and<br />
intercellular adhesion molecules [ICAM]) and release interleukin-1, interleukin-6, and interleukin-8. As a result, leukocytes adhere<br />
to endothelial cells, with diapedesis to the site of infection. Changes in the conformation of endothelial cells result in increased<br />
vascular permeability, with transudation of plasma proteins. Both tissue-based macrophages and circulating monocytes release<br />
interleukin-1, interleukin-6, interleukin-8, and tumor necrosis factor a (TNF-a) after exposure to staphylococci. Macrophage activation<br />
occurs after the release of interferon-g by T cells. Cytokines released into the bloodstream from monocytes or macrophages,<br />
as well as endothelial cells, contribute to the manifestations of the sepsis syndrome and vasculitis associated with systemic staphylococcal<br />
disease. Expression of Fc receptors may contribute to the vasculitis occasionally encountered during bacteremia by acting<br />
as a binding site for immunoglobulin (Ig) or immune <strong>com</strong>plexes. PMN denotes polymorphonuclear leukocyte.<br />
Toxin-Mediated Disease<br />
Pyrogenic-toxin superantigens cause life-threatening<br />
disease that is characterized by the rapid onset<br />
of high fever, shock, capillary leak, and multiorgan<br />
dysfunction. Superantigens are T-cell mitogens that<br />
bind directly to invariant regions of MHC class II<br />
molecules, bypassing intracellular protein ingestion<br />
and digestion and subsequent peptide presentation<br />
by antigen-presenting cells. The MHC-bound superantigens<br />
then attach to T cells according to the <strong>com</strong>position<br />
of the variable region of the T-cell–receptor<br />
b chain. Toxic shock syndrome toxin 1 binds all variable-region<br />
b2–positive T cells, causing an expansion<br />
of clonal T cells (5 to 20 percent of resting T cells<br />
as <strong>com</strong>pared with 0.01 percent of T cells for processed<br />
antigens), resulting in the massive release of<br />
Volume 339 Number 8 · 525<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
cytokines by both macrophages and T cells. These<br />
cytokines mediate the toxic shock syndrome, whose<br />
pathophysiology mimics that of endotoxin shock. In<br />
both syndromes, bacterial products induce the release<br />
of excessive quantities of cytokines, which then<br />
cause tissue damage. 14,66,69<br />
Host Response to Infection<br />
The typical pathological finding of staphylococcal<br />
disease is abscess formation. Leukocytes are the primary<br />
host defense against S. <strong>aureus</strong> infection. 70 The<br />
migration of leukocytes to the site of infection results<br />
from the orchestrated expression of adhesion<br />
molecules on endothelial cells. This cytokine-mediated<br />
process is triggered by bacteria and tissue-based<br />
macrophages. After infection, cytokines are first demonstrable<br />
within vessels, extending into tissues as<br />
inflammatory cells migrate to the sites of infection. 71<br />
S. <strong>aureus</strong>–infected endothelial cells also express intercellular<br />
adhesion molecule 1 (CD54), vascularcell<br />
adhesion molecule 1 (CD106), and MHC class<br />
I molecules and probably contribute to this process<br />
(Fig. 5). 72 Genetically manipulated mice lacking intercellular<br />
adhesion molecule 1 have a defect in leukocyte<br />
migration that results in increased mortality,<br />
but they also have less severe staphylococcal infections<br />
than normal mice, perhaps as a result of decreased<br />
leukocyte-mediated damage. 73<br />
The presence of opsonizing antibody directed<br />
against capsule, peptidoglycan, or <strong>com</strong>plement facilitates<br />
phagocytosis in vitro. 9,74,75 The role of antibody<br />
in vivo is less certain, since the titer of antistaphylococcal<br />
antibodies is not correlated with protection<br />
from infection, except in the case of toxic shock syndrome,<br />
in which the presence of anti–toxic shock<br />
syndrome toxin 1 is protective. 76,77 At present, it is<br />
not known which staphylococcal <strong>com</strong>ponents are<br />
capable of inducing protection from subsequent infection.<br />
DISEASES CAUSED BY S. AUREUS<br />
S. <strong>aureus</strong> infection is a major cause of skin, softtissue,<br />
respiratory, bone, joint, and endovascular disorders.<br />
The discussion below is limited to life-threatening<br />
staphylococcal infections. The majority of<br />
these infections occur in persons with multiple risk<br />
factors for infection. 78 More detailed discussions of<br />
the clinical manifestations of staphylococcal diseases<br />
can be found in several recent reports. 31,43,78<br />
Bacteremia<br />
The overall rate of mortality from staphylococcal<br />
bacteremia, which has not changed in the past 15<br />
years, ranges from 11 to 43 percent. 79 Factors associated<br />
with increased mortality include an age of<br />
more than 50 years, nonremovable foci of infection,<br />
and serious underlying cardiac, neurologic, or respiratory<br />
disease. Bacteremia caused by methicillinresistant<br />
strains is not associated with increased mortality.<br />
The change in the Acute Physiology and<br />
Chronic Health Evaluation (APACHE II) score from<br />
the day before to the day of S. <strong>aureus</strong> bacteremia was<br />
recently found to predict the clinical course and out<strong>com</strong>e.<br />
80 The frequency of <strong>com</strong>plications from staphylococcal<br />
bacteremia is high, ranging from 11 to 53<br />
percent. As many as 31 percent of patients with bacteremia<br />
who do not have evidence of endocarditis<br />
do have evidence of metastatic infection. 61,79,81-83<br />
An increasing percentage of bacteremic infections<br />
are related to catheterization. 34 The rate of <strong>com</strong>plications<br />
is lower for catheter-related infections than<br />
for all cases of bacteremia (24 percent), as is the<br />
overall mortality rate (15 percent). 83 Patients with<br />
bacteremia or fever that persists for more than 72<br />
hours after the catheter has been removed may have<br />
an increased risk of <strong>com</strong>plications. 84 The incidence<br />
of endocarditis in patients with catheters, estimated<br />
on the basis of clinical indicators, is also low, ranging<br />
from 0 to 18 percent. 83 Some studies, however, suggest<br />
that the incidence of endocarditis may be higher.<br />
Espersen and Frimodt-Møller 85 reported that the<br />
diagnosis of S. <strong>aureus</strong> endocarditis was made at autopsy<br />
and not suspected clinically in 55 percent of<br />
the patients in their series (65 of 119). Using transesophageal<br />
echocardiography, Fowler et al. 86 recently<br />
found that 25 percent of selected patients with<br />
staphylococcal bacteremia (26 of 103) and 23 percent<br />
of those with catheters as the primary focus (16<br />
of 69) had transesophageal echocardiographic evidence<br />
of endocarditis in the absence of clinical or<br />
transthoracic echocardiographic findings.<br />
Endocarditis<br />
The incidence of S. <strong>aureus</strong> endocarditis has increased<br />
and now accounts for 25 to 35 percent of<br />
cases. 81,87 It occurs in intravenous drug users, elderly<br />
patients, patients with prosthetic valves, and hospitalized<br />
patients. In all four groups, the initial presentation<br />
may be limited to fever and malaise, making<br />
diagnosis difficult. Unlike endocarditis caused by<br />
less virulent pathogens, S. <strong>aureus</strong> endocarditis is characterized<br />
by a rapid onset, high fever, frequent involvement<br />
of normal cardiac valves, and the absence<br />
of physical stigmata of the disease on initial presentation.<br />
88 In one study, 13 percent of febrile intravenous<br />
drug users evaluated in an emergency room had<br />
endocarditis, and the diagnosis could not have been<br />
predicted on the basis of available clinical or laboratory<br />
data. 89<br />
In cases of endocarditis related to intravenous<br />
drug use, the disease is frequently right-sided, the<br />
patients are young, the mortality rate is low, and the<br />
majority of patients do not have antecedent valvular<br />
disease. The prognosis is worse for intravenous drug<br />
users who have advanced disease associated with human<br />
immunodeficiency virus (HIV) infection than it<br />
526 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
is for those without HIV infection. 90 In cases of endocarditis<br />
that are not related to drug use, the disease<br />
is often left-sided, the patients are older, the<br />
mortality rate is high (20 to 44 percent), and the<br />
disease usually involves previously damaged cardiac<br />
valves. 61,81,88 In one review, the incidence of both<br />
embolic and neurologic <strong>com</strong>plications of left-sided<br />
S. <strong>aureus</strong> endocarditis was 50 percent. 88<br />
S. <strong>aureus</strong> is one of the most <strong>com</strong>mon pathogens<br />
in noso<strong>com</strong>ial and prosthetic-valve endocarditis, and<br />
intravascular catheters are the most frequent source<br />
of bacterial inoculation. The mortality rate for noso<strong>com</strong>ial<br />
endocarditis, regardless of the pathogen, is<br />
40 to 56 percent, and the rate is even higher when<br />
the pathogen is S. <strong>aureus</strong>. 91 In many of these cases,<br />
the diagnosis is obscured by other conditions or the<br />
administration of antibiotics. Prosthetic-valve endocarditis,<br />
especially in the early postoperative period,<br />
is often fulminant and is characterized by the formation<br />
of myocardial abscesses and the development of<br />
valvular insufficiency. Fang et al. 92 noted a 43 percent<br />
incidence of endocarditis in patients with prosthetic<br />
valves who had noso<strong>com</strong>ial bacteremia. The<br />
most <strong>com</strong>mon pathogen was S. <strong>aureus</strong>.<br />
Metastatic <strong>Infections</strong><br />
S. <strong>aureus</strong> has a tendency to spread to particular<br />
sites, including the bones, joints, kidneys, and<br />
lungs. 78,82,88 Suppurative collections at these sites<br />
serve as potential foci for recurrent infections. 78 Patients<br />
with persistent fever despite appropriate therapy<br />
should be evaluated for the presence of suppurative<br />
collections.<br />
Sepsis<br />
A minority of bacteremic or local infections<br />
progress to sepsis. Risk factors for sepsis include advanced<br />
age, immunosuppression, chemotherapy, and<br />
invasive procedures. The presentation of staphylococcal<br />
sepsis is similar to that of gram-negative sepsis,<br />
with fever, hypotension, tachycardia, and tachypnea.<br />
S. <strong>aureus</strong> is one of the most <strong>com</strong>mon gram-positive<br />
pathogens in cases of sepsis. 66 Severe cases progress<br />
to multiorgan dysfunction, disseminated intravascular<br />
coagulation, lactic acidosis, and death. 66 In both<br />
gram-positive and gram-negative sepsis, the levels of<br />
circulating tumor necrosis factor a, interleukin-1,<br />
and interleukin-6 are predictive of the out<strong>com</strong>e. 93<br />
Toxic Shock Syndrome<br />
Staphylococcal toxic shock syndrome came to<br />
prominence in 1980–1981, when numerous cases<br />
were associated with the introduction of superabsorbent<br />
tampons for use during menstruation. The disease<br />
is characterized by a fulminant onset, often in<br />
previously healthy persons. The diagnosis is based<br />
on clinical findings that include high fever, erythematous<br />
rash with subsequent desquamation, hypotension,<br />
and multiorgan damage. Alternative diagnoses,<br />
including Rocky Mountain spotted fever, streptococcal<br />
scarlet fever, and leptospirosis, must be ruled<br />
out. The toxic shock syndrome often develops from<br />
a site of colonization rather than infection. 94<br />
Although toxic shock syndrome toxin 1 accounts<br />
for more than 90 percent of cases of the syndrome<br />
that are associated with menstruation, other enterotoxins<br />
account for 50 percent of cases unrelated to<br />
menstruation. Nonmenstrual cases have increased<br />
and now account for approximately one third of all<br />
cases. These nonmenstrual cases have been associated<br />
with localized infections, surgery, or insect bites.<br />
Patients with nonmenstrual toxic shock syndrome<br />
have a higher mortality rate than those with menstrual<br />
toxic shock syndrome. 76<br />
MECHANISMS OF RESISTANCE<br />
TO ANTIMICROBIAL AGENTS<br />
Penicillin is inactivated by b-lactamase, a serine<br />
protease that hydrolyzes the b-lactam ring. Less than<br />
5 percent of isolates remain sensitive to penicillin.<br />
Resistance to methicillin confers resistance to all<br />
penicillinase-resistant penicillins and cephalosporins.<br />
This high level of resistance requires the presence of<br />
the mec gene that encodes penicillin-binding protein<br />
2a. 95 The mec genes probably originated from a different<br />
species of staphylococci. 96 Although many<br />
methicillin-resistant strains appear to be descendants<br />
of a limited number of clones, some appear to be<br />
multiclonal in origin, suggesting the horizontal transfer<br />
of mec DNA. 96-98 Other staphylococcal genes, including<br />
bla (for b-lactamase) and fem (for factors<br />
essential for methicillin resistance), affect the expression<br />
of resistance. The expression of resistance to<br />
methicillin is often heterogeneous, and the percentage<br />
of a bacterial population that expresses the<br />
resistance phenotype varies according to the environmental<br />
conditions. Antimicrobial-sensitivity testing<br />
has been modified to enhance the detection of<br />
the resistance phenotype. 95<br />
There has been increasing concern about the possible<br />
emergence of van<strong>com</strong>ycin-resistant S. <strong>aureus</strong><br />
strains. Resistance to van<strong>com</strong>ycin has been reported<br />
in clinical isolates of S. haemolyticus, 99 a coagulase-negative<br />
species. The enterococcal plasmid-bearing gene<br />
for resistance to van<strong>com</strong>ycin has been transferred by<br />
conjugation to S. <strong>aureus</strong> in vitro. 100 Four recent case<br />
reports (one from Japan and three from the United<br />
States) have documented the isolation of clinical<br />
strains with intermediate sensitivity to van<strong>com</strong>ycin<br />
(minimal inhibitory concentration, 8 mg per milliliter).<br />
39,101 The mechanism of resistance in these isolates<br />
is not known but is not due to the van genes<br />
present in enterococci. Both increased cell-wall synthesis<br />
and alterations in the cell wall that prevent van<strong>com</strong>ycin<br />
from reaching sites of cell-wall synthesis have<br />
been suggested as mechanisms. 39,102 Screening for<br />
Volume 339 Number 8 · 527<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
TABLE 1. ANTIMICROBIAL THERAPY FOR SERIOUS S. AUREUS INFECTIONS.*<br />
SENSITIVITY OR RESISTANCE<br />
OF ISOLATE DRUG OF CHOICE ALTERNATIVE COMMENTS<br />
Sensitive to penicillin<br />
Sensitive to methicillin<br />
Resistant to methicillin<br />
Resistant to methicillin<br />
with intermediate sensitivity<br />
to van<strong>com</strong>ycin§<br />
Not yet known<br />
Penicillin G (4 million<br />
units every 4 hr)<br />
Nafcillin or oxacillin<br />
(2 g every 4 hr)<br />
Van<strong>com</strong>ycin (1 g every<br />
12 hr)†<br />
Uncertain<br />
Van<strong>com</strong>ycin (1 g every<br />
12 hr)<br />
Nafcillin (2 g every 4 hr), oxacillin<br />
(2 g every 4 hr), cefazolin (2 g<br />
every 8 hr), van<strong>com</strong>ycin (1 g every<br />
12 hr)<br />
Cefazolin (2 g every 8 hr)†, van<strong>com</strong>ycin<br />
(1 g every 12 hr)†<br />
TMP–SMZ (TMP, 5 mg/kg of body<br />
weight every 12 hr),† minocycline<br />
(100 mg every 12 hr orally),† ciprofloxacin<br />
(400 mg every 12 hr),†<br />
trovafloxacin (300 mg every 24 hr),<br />
levofloxacin (500 mg every 24<br />
hr),† as well as investigational<br />
drugs (quinupristin–dalfopristin,<br />
oxzolidinones, new carbapenem<br />
[L-695,256])<br />
Same as for methicillin-resistant<br />
strains<br />
Less than 5 percent of isolates are sensitive to penicillin<br />
Patients with penicillin allergy can be treated with a cephalosporin<br />
if the allergy does not involve an anaphylactic<br />
or accelerated reaction; van<strong>com</strong>ycin is the alternative;<br />
desensitization to b-lactams may be necessary in some<br />
cases‡<br />
Sensitivity testing is necessary before an alternative drug<br />
is used; adjunctive drugs (those that should be used<br />
only in <strong>com</strong>bination with other antimicrobial agents)<br />
include gentamicin, rifampin, and fusidic acid (not<br />
readily available in the United States); quinupristin–dalfopristin<br />
is bactericidal against methicillin-resistant isolates<br />
unless the strain is erythromycin-resistant; the<br />
newer quinolones may retain in vitro activity against<br />
ciprofloxacin-resistant isolates; resistance may develop<br />
during therapy; the efficacy of adjunctive therapy is unknown‡<br />
Same as for methicillin-resistant strains<br />
— Empirical therapy is given when the susceptibility of the<br />
isolate is not known. Van<strong>com</strong>ycin with or without an<br />
aminoglycoside is re<strong>com</strong>mended for suspected <strong>com</strong>munity-<br />
or hospital-acquired S. <strong>aureus</strong> infections because<br />
of the increased frequency of methicillin-resistant<br />
strains in the <strong>com</strong>munity<br />
*The route of administration is intravenous unless otherwise indicated. TMP–SMZ denotes trimethoprim–sulfamethoxazole.<br />
†The dosage must be adjusted in patients with reduced creatinine clearance.<br />
‡For the treatment of prosthetic-valve endocarditis, the addition of gentamicin (1 mg per kilogram every 8 hours) and rifampin (300 mg orally every<br />
8 hours) is re<strong>com</strong>mended, with adjustment of the dosage of gentamicin if the creatinine clearance is reduced.<br />
§Van<strong>com</strong>ycin-resistant S. <strong>aureus</strong> isolates have not been reported to date.<br />
strains of S. <strong>aureus</strong> with intermediate sensitivities to<br />
glycopeptides including van<strong>com</strong>ycin (glycopeptideintermediate<br />
strains) can be performed with the use<br />
of brain–heart infusion agar plates supplemented with<br />
6 mg of van<strong>com</strong>ycin per milliliter. Confirmation of<br />
sensitivity by the broth-dilution method is re<strong>com</strong>mended.<br />
103 Van<strong>com</strong>ycin-resistant S. <strong>aureus</strong> strains are<br />
likely to pose a major therapeutic challenge in the<br />
future.<br />
TREATMENT OF S. AUREUS INFECTION<br />
Penicillin remains the drug of choice if the isolate<br />
is sensitive to it (Table 1). A semisynthetic penicillin<br />
(nafcillin or oxacillin) is indicated for b-lactamase–<br />
producing strains. In patients with histories of delayed-type<br />
penicillin allergy, a cephalosporin such as<br />
cefazolin or cephalothin is an acceptable alternative.<br />
In vitro data from experimental and clinical studies<br />
suggest that van<strong>com</strong>ycin is a less effective antistaphylococcal<br />
drug than the b-lactams. 104,105 Therefore,<br />
the selection of van<strong>com</strong>ycin as an alternative to a<br />
b-lactam in a patient with a history of allergy should<br />
be carefully considered.<br />
Van<strong>com</strong>ycin is the drug of choice for methicillin-resistant<br />
isolates. Patients unable to tolerate van<strong>com</strong>ycin<br />
have been treated with fluoroquinolones,<br />
trimethoprim–sulfamethoxazole, clindamycin, or minocycline.<br />
Each of these drugs has been effective in<br />
cases that require bactericidal therapy. 95,106 They are<br />
not as effective as van<strong>com</strong>ycin, however, either because<br />
they have less antistaphylococcal activity or because<br />
resistance develops during therapy. 95,107 Quinolones<br />
with enhanced antistaphylococcal activity have<br />
recently be<strong>com</strong>e available, but their use may also be<br />
limited by the development of resistance during<br />
therapy. A number of potentially active drugs are<br />
under investigation, including quinupristin–dalfopristin,<br />
a new carbapenem, and a new family of antimicrobial<br />
drugs, oxzolidinones. 106 The glycopeptide-intermediate<br />
strains reported to date have been<br />
variably sensitive to chloramphenicol, gentamicin,<br />
rifampin, trimethoprim–sulfamethoxazole, and tetracycline.<br />
39,101,103 The initial case involving a glycopeptide-intermediate<br />
strain was treated with surgical<br />
débridement and ampicillin–sulbactam plus an aminoglycoside.<br />
39<br />
528 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
Antimicrobial <strong>com</strong>binations have been used to increase<br />
bactericidal activity or to prevent the development<br />
of antimicrobial resistance. The <strong>com</strong>bination<br />
of b-lactams and aminoglycosides increases bacterial<br />
killing in vitro and in animal models of endocarditis.<br />
108 In a clinical trial <strong>com</strong>paring a single drug with<br />
<strong>com</strong>bination therapy for the treatment of endocarditis,<br />
<strong>com</strong>bination therapy resulted in more rapid<br />
clearance of bacteria from the bloodstream, but the<br />
clinical out<strong>com</strong>e was the same with the two approaches.<br />
109 Many clinicians use an aminoglycoside,<br />
when possible, for the first few days of therapy.<br />
Rifampin is another potent antistaphylococcal drug,<br />
but resistance invariably develops if it is used alone.<br />
Although the efficacy of rifampin as an adjunctive<br />
drug in patients with life-threatening infections remains<br />
controversial, it is re<strong>com</strong>mended in <strong>com</strong>bination<br />
with gentamicin and van<strong>com</strong>ycin or nafcillin for<br />
the treatment of prosthetic-valve endocarditis. 110 Rifampin<br />
has also been <strong>com</strong>bined with quinolones in<br />
an effort to prevent the development of resistance. 111<br />
The duration of therapy for invasive, life-threatening<br />
infections, including those that cause endocarditis,<br />
osteomyelitis, or arthritis, is four weeks or longer.<br />
The appropriate duration of treatment for bacteremias<br />
originating from a removable focus of infection,<br />
such as an intravascular catheter, is controversial. A<br />
two-week period of therapy has been re<strong>com</strong>mended<br />
for infections considered to pose a low risk of <strong>com</strong>plications<br />
(those caused by catheterization in nonimmuno<strong>com</strong>promised<br />
patients without valvular abnormalities,<br />
with prompt removal of the catheter, rapid<br />
clearance of bacteremia, and no evidence of metastatic<br />
infection). 61,83 However, a meta-analysis concluded<br />
that, despite the reportedly low <strong>com</strong>plication rates,<br />
the available data do not justify short-course therapy<br />
in such patients. 83 There is also concern that endocarditis<br />
has been underdiagnosed because of a reliance<br />
on clinical criteria. 85,86 Despite some promising<br />
studies, tests for serum anti–teichoic acid antibodies<br />
to help identify patients at risk for <strong>com</strong>plications have<br />
not proved useful. 31,112<br />
When short-course therapy is being considered,<br />
performance of transesophageal echocardiography<br />
clearly reduces the likelihood of missing a diagnosis of<br />
endocarditis, but it does not eliminate the possibility<br />
of recurrent infections resulting from metastatic suppurative<br />
collections. Risk factors that would reliably<br />
identify patients at risk for the development of metastatic<br />
suppurative collections have not been identified.<br />
In a few studies, parenteral therapy given for two<br />
weeks or oral therapy given for four weeks was effective<br />
in intravenous drug users with tricuspid-valve<br />
endocarditis. Most of the patients were nonimmuno<strong>com</strong>promised<br />
and had un<strong>com</strong>plicated, tricuspid-valve<br />
endocarditis caused by methicillin-sensitive<br />
S. <strong>aureus</strong>. Defervescence occurred promptly after the<br />
institution of therapy with either regimen. The parenteral<br />
regimen consisted of a semisynthetic penicillin<br />
plus an aminoglycoside (1 mg per kilogram of body<br />
weight every 8 hours), whereas the oral regimen<br />
<strong>com</strong>bined ciprofloxacin (750 mg every 12 hours)<br />
with rifampin (300 mg every 12 hours). 110,111,113-115<br />
The oral regimen may also be used for long-term<br />
suppressive therapy. The possible development of<br />
antimicrobial-resistant strains during therapy remains<br />
a concern with this regimen.<br />
In addition to antimicrobial therapy, drainage of<br />
suppurative collections is necessary. The likelihood<br />
of sterilizing an infected site in the presence of a foreign<br />
device is low. In one study, the success rate for<br />
treating Hickman catheter–associated infections without<br />
removal of the catheters was 18 percent. 116 On<br />
the basis of this and similar studies, the re<strong>com</strong>mendation<br />
is to remove the device when possible. Recent<br />
studies suggest that in patients with prosthetic-valve<br />
endocarditis, valve replacement results in a better out<strong>com</strong>e<br />
than medical management alone. 117<br />
The treatment of toxic shock syndrome is directed<br />
against the consequences of the toxin. Management<br />
includes fluid replacement for shock, careful monitoring<br />
and antibiotic therapy to eliminate staphylococcal<br />
colonization or infection, and removal of infected<br />
material. Glucocorticoids are of uncertain value.<br />
In vitro studies have shown that the use of intravenous<br />
immune globulin with high titers of antienterotoxin<br />
antibodies prevents T-cell stimulation by enterotoxins,<br />
suggesting that immune globulin may have a<br />
role in the treatment of the toxic shock syndrome. 118<br />
PREVENTION OF STAPHYLOCOCCAL<br />
DISEASE<br />
The use of topical agents to eliminate staphylococcal<br />
colonization in high-risk groups, such as patients<br />
undergoing hemodialysis or surgery, has been<br />
shown to reduce the incidence of subsequent infections.<br />
27 Mupirocin, a topical antistaphylococcal agent<br />
that inhibits RNA and protein synthesis, eliminates<br />
nasal colonization in carriers and can reduce the incidence<br />
of wound infections. 24,119 Although the development<br />
of resistance to mupirocin to date has<br />
been limited, prolonged use of the drug has been associated<br />
with resistance. 120<br />
A capsular polysaccharide–protein conjugate antistaphylococcal<br />
vaccine has produced improved phagocytosis<br />
in vitro and improved survival in experimental<br />
models of staphylococcal infection, including<br />
endocarditis. 121,122 Balaban et al. 123 demonstrated<br />
that immunization with RNAIII-activating protein,<br />
an agr-encoded protein involved in regulating the<br />
expression of staphylococcal exoproteins, is protective<br />
in an experimental model of cutaneous infection.<br />
Other potential approaches involve the development<br />
of multi<strong>com</strong>ponent vaccines incorporating<br />
proteins identified as having a role in the pathogenesis<br />
of staphylococcal disease.<br />
Volume 339 Number 8 · 529<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
At present, prevention of the spread of infection<br />
relies on the application of appropriate principles of<br />
infection control. These approaches have been effective<br />
in reducing the noso<strong>com</strong>ial spread of staphylococcal<br />
infection. Guidelines for the isolation of subjects<br />
colonized with glycopeptide-intermediate or<br />
van<strong>com</strong>ycin-resistant S. <strong>aureus</strong> strains have recently<br />
been published. 124,125<br />
Supported in part by grants from the American Heart Association and<br />
the National Institute on Drug Abuse (DA09656 and DA11868).<br />
I am indebted to Drs. Abigail Zuger, Timothy J. Foster, and David<br />
Hammerman for their critical review of the manuscript; to Dr. Robert<br />
Gaynes for providing unpublished data from the National Noso<strong>com</strong>ial<br />
<strong>Infections</strong> Surveillance system; and to Dr. Christine Lawrence<br />
for providing the photograph of staphyloccoci with Gram’s stain.<br />
REFERENCES<br />
1. Ogston A. Micrococcus poisoning. J Anat 1882;17:24-58.<br />
2. Classics in infectious diseases: “On abscesses”: Alexander Ogston<br />
(1844-1929). J Infect Dis 1984;6:122-8.<br />
3. Brumfitt W, Hamilton-Miller J. Methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong>.<br />
N Engl J Med 1989;320:1188-96.<br />
4. Sheagren JN. <strong>Staphylococcus</strong> <strong>aureus</strong>: the persistent pathogen. N Engl<br />
J Med 1984;310:1368-73, 1437-42.<br />
5. Wilkinson BJ, Biology. In: Crossley KB, Archer GL, eds. The staphylococci<br />
in human disease. New York: Churchill Livingstone, 1997:1-38.<br />
6. Novick RP. The staphylococcus as a molecular genetic system. In: Novick<br />
RP, ed. Molecular biology of the staphylococci. New York: VCH,<br />
1990:1-37.<br />
7. Schaberg DR, Zervos MJ. Intergeneric and interspecies gene exchange<br />
in gram-positive cocci. Antimicrob Agents Chemother 1986;30:817-22.<br />
8. Kessler CM, Nussbaum E, Tuazon CU. Disseminated intravascular coagulation<br />
associated with <strong>Staphylococcus</strong> <strong>aureus</strong> septicemia is mediated by<br />
peptidoglycan-induced platelet aggregation. J Infect Dis 1991;164:101-7.<br />
9. Lee JC. The prospects for developing a vaccine against <strong>Staphylococcus</strong><br />
<strong>aureus</strong>. Trends Microbiol 1996;4:162-6.<br />
10. Foster TJ, McDevitt D. Surface-associated proteins of <strong>Staphylococcus</strong><br />
<strong>aureus</strong>: their possible roles in virulence. FEMS Microbiol Lett 1994;118:<br />
199-205.<br />
11. Patti JM, Allen BL, McGavin MJ, Höök M. MSCRAMM-mediated<br />
adherence of microorganisms to host tissues. Ann Rev Microbiol 1994;48:<br />
585-617.<br />
12. Bhakdi S, Tranum-Jensen J. Alpha-toxin of <strong>Staphylococcus</strong> <strong>aureus</strong>.<br />
Microbiol Rev 1991;55:733-51.<br />
13. Walev I, Reske K, Palmer M, Valeva A, Bhakdi S. Potassium-inhibited<br />
processing of IL-1b in human monocytes. EMBO J 1995;14:1607-14.<br />
14. Marrack P, Kappler J. The staphylococcal enterotoxins and their relatives.<br />
Science 1990;248:705-11. [Erratum, Science 1990;248:1066.]<br />
15. Harris TO, Grossman D, Kappler JW, Marrack P, Rich RR, Betley MJ.<br />
Lack of <strong>com</strong>plete correlation between T-cell-stimulatory activities of staphylococcal<br />
enterotoxins. Infect Immun 1993;61:3175-83.<br />
16. Cribier B, Prevost G, Couppie P, Finck-Barbancon V, Grosshans E,<br />
Piemont Y. <strong>Staphylococcus</strong> <strong>aureus</strong> leukocidin: a new virulence factor in<br />
cutaneous infections? An epidemiological and experimental study. Dermatology<br />
1992;185:175-80.<br />
17. Peng HL, Novick RP, Kreiswirth B, Kornblum J, Schlievert P. Cloning,<br />
characterization, and sequencing of an accessory gene regulator (agr)<br />
in <strong>Staphylococcus</strong> <strong>aureus</strong>. J Bacteriol 1988;170:4365-72.<br />
18. Cheung AL, Koomey JM, Butler CA, Projan SJ, Fischetti VA. Regulation<br />
of exoprotein expression in <strong>Staphylococcus</strong> <strong>aureus</strong> by a locus (sar)<br />
distinct from agr. Proc Natl Acad Sci U S A 1992;89:6462-6.<br />
19. Ji G, Beavis RC, Novick RP. Cell density control of staphylococcal virulence<br />
mediated by an octapeptide pheromone. Proc Natl Acad Sci U S A<br />
1995;92:12055-9.<br />
20. Cheung AL, Eberhardt KJ, Chung E, et al. Diminished virulence of a<br />
sar ¡ agr ¡ mutant of <strong>Staphylococcus</strong> <strong>aureus</strong> in the rabbit model of endocarditis.<br />
J Clin Invest 1994;94:1815-22.<br />
21. Noble WC, Valkenburg HA, Wolters CHL. Carriage of <strong>Staphylococcus</strong><br />
<strong>aureus</strong> in random samples of a normal population. J Hyg (Lond) 1967;65:<br />
567-73.<br />
22. Casewell MW, Hill RLR. The carrier state: methicillin-resistant <strong>Staphylococcus</strong><br />
<strong>aureus</strong>. J Antimicrob Chemother 1986;18:Suppl A:1-12.<br />
23. Sanford MD, Widmer AF, Bale MJ, Jones RN, Wenzel RP. Efficient<br />
detection and long-term persistence of the carriage of methicillin-resistant<br />
<strong>Staphylococcus</strong> <strong>aureus</strong>. Clin Infect Dis 1994;19:1123-8.<br />
24. Wenzel RP, Perl TM. The significance of nasal carriage of <strong>Staphylococcus</strong><br />
<strong>aureus</strong> and the incidence of postoperative wound infection. J Hosp<br />
Infect 1995;31:13-24.<br />
25. Tuazon CU, Perez A, Kishaba T, Sheagren JN. <strong>Staphylococcus</strong> <strong>aureus</strong><br />
among insulin-injecting diabetic patients: an increased carrier rate. JAMA<br />
1975;231:1272.<br />
26. Tuazon CU, Sheagren JN. Increased rate of carriage of <strong>Staphylococcus</strong><br />
<strong>aureus</strong> among narcotic addicts. J Infect Dis 1974;129:725-7.<br />
27. Yu VL, Goetz A, Wagener M, et al. <strong>Staphylococcus</strong> <strong>aureus</strong> nasal carriage<br />
and infection in patients on hemodialysis: efficacy of antibiotic prophylaxis.<br />
N Engl J Med 1986;315:91-6.<br />
28. Weinstein HJ. The relation between the nasal-staphylococcal-carrier<br />
state and the incidence of postoperative <strong>com</strong>plications. N Engl J Med<br />
1959;260:1303-8.<br />
29. Kluytmans JAJW, Mouton JW, Ijzerman EPF, et al. Nasal carriage of<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> as a major risk factor for wound infections after cardiac<br />
surgery. J Infect Dis 1995;171:216-9.<br />
30. Weinke T, Schiller R, Fehrenbach FJ, Pohle HD. Association between<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> nasopharyngeal colonization and septicemia in patients<br />
infected with the human immunodeficiency virus. Eur J Clin Microbiol<br />
Infect Dis 1992;11:985-9.<br />
31. Waldvogel FA. <strong>Staphylococcus</strong> <strong>aureus</strong> (including toxic shock syndrome).<br />
In: Mandell GL, Bennett JE, Dolin R, eds. Mandell, Douglas and<br />
Bennett’s principles and practice of infectious diseases. 4th ed. Vol. 2. New<br />
York: Churchill Livingstone, 1995:1754-77.<br />
32. Sheretz RJ, Reagan DR, Hampton KD, et al. A cloud adult: the <strong>Staphylococcus</strong><br />
<strong>aureus</strong>-virus interaction revisited. Ann Intern Med 1996;124:539-47.<br />
33. Banerjee SN, Emori TG, Culver DH, et al. Secular trends in noso<strong>com</strong>ial<br />
primary bloodstream infections in the United States, 1980-1989. Am<br />
J Med 1991;91:Suppl 3B:3B-86S–3B-89S.<br />
34. Steinberg JP, Clark CC, Hackman BO. Noso<strong>com</strong>ial and <strong>com</strong>munityacquired<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> bacteremias from 1980 to 1993: impact of<br />
intravascular devices and methicillin resistance. Clin Infect Dis 1996;23:<br />
255-9.<br />
35. Emori TG, Gaynes RP. An overview of noso<strong>com</strong>ial infections, including<br />
the role of the microbiology laboratory. Clin Microbiol Rev 1993;6:<br />
428-42.<br />
36. Panlilio A, Culver DH, Gaynes RP, et al. Methicillin-resistant <strong>Staphylococcus</strong><br />
<strong>aureus</strong> in U.S. hospitals, 1975-1991. Infect Control Hosp Epidemiol<br />
1992;13:582-6.<br />
37. Speller DCE, Johnson AP, James D, Marples RR, Charlett A, George<br />
RC. Resistance to methicillin and other antibiotics in isolates of <strong>Staphylococcus</strong><br />
<strong>aureus</strong> from blood and cerebrospinal fluid, England and Wales,<br />
1989-95. Lancet 1997;350:323-5.<br />
38. Moreno F, Crisp C, Jorgensen JH, Patterson JE. Methicillin-resistant<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> as a <strong>com</strong>munity organism. Clin Infect Dis 1995;21:<br />
1308-12.<br />
39. Hiramatsu K, Hanaki H, Ino T, Yabuta K, Oguri T, Tenover FC.<br />
Methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong> clinical strain with reduced van<strong>com</strong>ycin<br />
susceptibility. J Antimicrob Chemother 1997;40:135-6.<br />
40. Sanches IS, Ramirez M, Troni H, et al. Evidence for the geographic<br />
spread of a methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong> clone between Portugal<br />
and Spain. J Clin Microbiol 1995;33:1243-6.<br />
41. Dominguez MA, de Lencastre H, Linares J, Tomasz A. Spread and<br />
maintenance of a dominant methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong><br />
(MRSA) clone during an outbreak of MRSA disease in a Spanish hospital.<br />
J Clin Microbiol 1994;32:2081-7.<br />
42. Foster TJ, Hartford O, O’Donnell D. Host–pathogen protein–protein<br />
interactions in <strong>Staphylococcus</strong>. In: McCrae MA, Saunders JR, Smyth CJ,<br />
Stow ND, eds. Molecular aspects of host–pathogen interaction. Cambridge,<br />
England: Cambridge University Press, 1997:67-94.<br />
43. Crossley KB, Archer GL, eds. The staphylococci in human disease.<br />
New York: Churchill Livingstone, 1997.<br />
44. Sanford BA, Ramsay MA. In vivo localization of <strong>Staphylococcus</strong> <strong>aureus</strong><br />
in nasal tissues of healthy and influenza A virus-infected ferrets. Proc Soc<br />
Exp Biol Med 1989;191:163-9.<br />
45. Shuter J, Hatcher VB, Lowy FD. <strong>Staphylococcus</strong> <strong>aureus</strong> binding to human<br />
nasal mucin. Infect Immun 1996;64:310-8.<br />
46. Elek SD, Conen PE. The virulence of <strong>Staphylococcus</strong> pyogenes for man:<br />
a study of the problems of wound infection. Br J Exp Pathol 1957;38:573-<br />
86.<br />
47. Zimmerli W, Lew PD, Waldvogel FA. Pathogenesis of foreign body infection:<br />
evidence for a local granulocyte defect. J Clin Invest 1984;73:<br />
1191-200.<br />
48. Cheung AL, Fischetti VA. The role of fibrinogen in staphylococcal<br />
adherence to catheters in vitro. J Infect Dis 1990;161:1177-86.<br />
49. Vaudaux P, Pittet D, Haeberli A, et al. Fibronectin is more active than<br />
530 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
MEDICAL PROGRESS<br />
fibrin or fibrinogen in promoting <strong>Staphylococcus</strong> <strong>aureus</strong> adherence to inserted<br />
intravascular catheters. J Infect Dis 1993;167:633-41.<br />
50. Tsao MM, Katz D. Central venous catheter-induced endocarditis: human<br />
correlate of the animal experimental model of endocarditis. Rev Infect<br />
Dis 1984;6:783-90.<br />
51. Vercellotti GM, Lussenhop D, Peterson PK, et al. Bacterial adherence<br />
to fibronectin and endothelial cells: a possible mechanism for bacterial tissue<br />
tropism. J Lab Clin Med 1984;103:34-43.<br />
52. Ogawa SK, Yurberg ER, Hatcher VB, Levitt MA, Lowy FD. Bacterial<br />
adherence to human endothelial cells in vitro. Infect Immun 1985;50:218-24.<br />
53. Tompkins DC, Hatcher VB, Patel D, Orr GA, Higgins LL, Lowy FD.<br />
A human endothelial cell membrane protein that binds <strong>Staphylococcus</strong> <strong>aureus</strong><br />
in vitro. J Clin Invest 1990;85:1248-54.<br />
54. Lowy FD, Fant J, Higgins LL, Ogawa SK, Hatcher VB. <strong>Staphylococcus</strong><br />
<strong>aureus</strong> — human endothelial cell interactions. J Ultrastruct Mol Struct Res<br />
1988;98:137-46.<br />
55. Hamill RJ, Vann JM, Proctor RA. Phagocytosis of <strong>Staphylococcus</strong> <strong>aureus</strong><br />
by cultured bovine aortic endothelial cells: model for postadherence<br />
events in endovascular infections. Infect Immun 1986;54:833-6.<br />
56. Vesga O, Groeschel MC, Otten MF, Brar DW, Vann JM, Proctor RA.<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> small colony variants are induced by the endothelial<br />
cell intracellular milieu. J Infect Dis 1996;173:739-42.<br />
57. Proctor RA, van Langevelde P, Kristjansson M, Maslow JN, Arbeit<br />
RD. Persistent and relapsing infections associated with small-colony variants<br />
of <strong>Staphylococcus</strong> <strong>aureus</strong>. Clin Infect Dis 1995;20:95-102.<br />
58. Wu T, Yeaman MR, Bayer AS. In vitro resistance to platelet microbicidal<br />
protein correlates with endocarditis source among bacteremic staphylococcal<br />
and streptococcal isolates. Antimicrob Agents Chemother 1994;<br />
38:729-32.<br />
59. Alston WK, Elliott DA, Epstein ME, Hatcher VB, Tang M, Lowy FD.<br />
Extracellular matrix heparan sulfate modulates endothelial cell susceptibility<br />
to <strong>Staphylococcus</strong> <strong>aureus</strong>. J Cell Physiol 1997;173:102-9.<br />
60. Drake TA, Pang M. <strong>Staphylococcus</strong> <strong>aureus</strong> induces tissue factor expression<br />
in cultured human cardiac valve endothelium. J Infect Dis 1988;157:749-56.<br />
61. Ing MB, Baddour LM, Bayer AS. Bacteremia and infective endocarditis:<br />
pathogenesis, diagnosis, and <strong>com</strong>plications. In: Crossley KB, Archer<br />
GL, eds. The staphylococci in human disease. New York: Churchill Livingstone,<br />
1997:331-54.<br />
62. Patti JM, Bremell T, Krajewska-Pietrasik D, et al. The <strong>Staphylococcus</strong><br />
<strong>aureus</strong> collagen adhesin is a virulence determinant in experimental septic<br />
arthritis. Infect Immun 1994;62:152-61.<br />
63. Timmerman CP, Mattsson E, Martinez-Martinez L, et al. Induction<br />
of release of tumor necrosis factor from human monocytes by staphylococci<br />
and staphylococcal peptidoglycans. Infect Immun 1993;61:4167-72.<br />
64. Heumann D, Barras C, Severin A, Glauser MP, Tomasz A. Grampositive<br />
cell walls stimulate synthesis of tumor necrosis factor alpha and<br />
interleukin-6 by human monocytes. Infect Immun 1994;62:2715-21.<br />
65. Yao L, Bengualid V, Lowy FD, Gibbons JJ, Hatcher VB, Berman JW.<br />
Internalization of <strong>Staphylococcus</strong> <strong>aureus</strong> by endothelial cells induces cytokine<br />
gene expression. Infect Immun 1995;63:1835-9.<br />
66. Bone RC. Gram-positive organisms and sepsis. Arch Intern Med 1994;<br />
154:26-34.<br />
67. Spika JS, Peterson PK, Wilkinson BJ, et al. Role of peptidoglycan from<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> in leukopenia, thrombocytopenia, and <strong>com</strong>plement<br />
activation associated with bacteremia. J Infect Dis 1982;146:227-34.<br />
68. De Kimpe SJ, Kengatharan M, Thiemermann C, Vane JR. The cell<br />
wall <strong>com</strong>ponents peptidoglycan and lipoteichoic acid from <strong>Staphylococcus</strong><br />
<strong>aureus</strong> act in synergy to cause shock and multiple organ failure. Proc Natl<br />
Acad Sci U S A 1995;92:10359-63.<br />
69. Bohach GA, Fast DJ, Nelson RD, Schlievert PM. Staphylococcal and<br />
streptococcal pyrogenic toxins involved in toxic shock syndrome and related<br />
illnesses. Crit Rev Microbiol 1990;17:251-72.<br />
70. Verdrengh M, Tarkowski A. Role of neutrophils in experimental septicemia<br />
and septic arthritis induced by <strong>Staphylococcus</strong> <strong>aureus</strong>. Infect Immun<br />
1997;65:2517-21.<br />
71. Yao L, Berman JW, Factor SM, Lowy FD. Correlation of histopathologic<br />
and bacteriologic changes with cytokine expression in an experimental<br />
murine model of bacteremic <strong>Staphylococcus</strong> <strong>aureus</strong> infection. Infect Immun<br />
1997;65:3889-95.<br />
72. Beekhuizen H, van de Gevel JS, Olsson B, van Benten IJ, van Furth<br />
R. Infection of human vascular endothelial cells with <strong>Staphylococcus</strong> <strong>aureus</strong><br />
induces hyperadhesiveness for human monocytes and granulocytes. J Immunol<br />
1997;158:774-82.<br />
73. Verdrengh M, Springer TA, Gutierrez-Ramos J-C, Tarkowski A. Role<br />
of intercellular adhesion molecule 1 in pathogenesis of staphylococcal arthritis<br />
and in host defense against staphylococcal bacteremia. Infect Immun<br />
1996;64:2804-7.<br />
74. Peterson PK, Wilkinson BJ, Kim Y, et al. The key role of peptidoglycan<br />
in the opsonization of <strong>Staphylococcus</strong> <strong>aureus</strong>. J Clin Invest 1978;61:597-<br />
609.<br />
75. Karakawa WW, Sutton A, Schneerson R, Karpas A, Vann WF. Capsular<br />
antibodies induce type-specific phagocytosis of capsulated <strong>Staphylococcus</strong><br />
<strong>aureus</strong> by human polymorphonuclear leukocytes. Infect Immun 1988;56:<br />
1090-5.<br />
76. Wergeland HI, Haaheim LR, Natås OB, Wesenberg F, Oeding P. Antibodies<br />
to staphylococcal peptidoglycan and its peptide epitopes, teichoic<br />
acid, and lipoteichoic acid in sera from blood donors and patients with<br />
staphylococcal infections. J Clin Microbiol 1989;27:1286-91.<br />
77. Freedman JD, Beer DJ. Expanding perspectives on the toxic shock syndrome.<br />
Adv Intern Med 1991;36:363-97.<br />
78. Musher DM, Lamm N, Darouiche RO, Young EJ, Hamill RJ, Landon<br />
GC. The current spectrum of <strong>Staphylococcus</strong> <strong>aureus</strong> infection in a tertiary<br />
care hospital. Medicine (Baltimore) 1994;73:186-208.<br />
79. Mylotte JM, McDermott C, Spooner JA. Prospective study of 114<br />
consecutive episodes of <strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia. Rev Infect Dis<br />
1987;9:891-907.<br />
80. Yzerman EPF, Boelens HAM, Tjhie JHT, Kluytmans JAJW, Mouton<br />
JW, Verbrugh HA. DAPACHE II for predicting course and out<strong>com</strong>e of<br />
noso<strong>com</strong>ial <strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia and its relation to host defense.<br />
J Infect Dis 1996;173:914-9.<br />
81. Sanabria TJ, Alpert JS, Goldberg R, Pape LA, Cheeseman SH. Increasing<br />
frequency of staphylococcal infective endocarditis: experience at a university<br />
hospital, 1981 through 1988. Arch Intern Med 1990;150:1305-9.<br />
82. Libman H, Arbeit RD. Complications associated with <strong>Staphylococcus</strong><br />
<strong>aureus</strong> bacteremia. Arch Intern Med 1984;144:541-5.<br />
83. Jernigan JA, Farr BM. Short-course therapy of catheter-related <strong>Staphylococcus</strong><br />
<strong>aureus</strong> bacteremia: a meta-analysis. Ann Intern Med 1993;119:<br />
304-11.<br />
84. Raad II, Sabbagh MF. Optimal duration of therapy of catheter-related<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia: a study of 55 cases and review. Clin Infect<br />
Dis 1992;14:75-82.<br />
85. Espersen F, Frimodt-Møller N. <strong>Staphylococcus</strong> <strong>aureus</strong> endocarditis: a<br />
review of 119 cases. Arch Intern Med 1986;146:1118-21.<br />
86. Fowler VG Jr, Li J, Corey GR, et al. Role of echocardiography in evaluation<br />
of patients with <strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia: experience in 103<br />
patients. J Am Coll Cardiol 1997;30:1072-8.<br />
87. Sandre RM, Shafran SD. Infective endocarditis: review of 135 cases<br />
over 9 years. Clin Infect Dis 1996;22:276-86.<br />
88. Chambers HF, Korzeniowski OM, Sande MA. <strong>Staphylococcus</strong> <strong>aureus</strong><br />
endocarditis: clinical manifestations in addicts and nonaddicts. Medicine<br />
(Baltimore) 1983;62:170-7.<br />
89. Marantz PR, Linzer M, Feiner CJ, Feinstein SA, Kozin AM, Friedland<br />
GH. Inability to predict diagnosis in febrile intravenous drug abusers. Ann<br />
Intern Med 1987;106:823-8.<br />
90. Pulvirenti JJ, Kerns E, Benson C, Lisowski J, Demarais P, Weinstein<br />
RA. Infective endocarditis in injection drug users: importance of human<br />
immunodeficiency virus serostatus and degree of immunosuppression.<br />
J Infect Dis 1996;22:40-5.<br />
91. Fernández-Guerrero ML, Verdejo C, Azofra J, de Górgolas M. Hospital-acquired<br />
infectious endocarditis not associated with cardiac surgery:<br />
an emerging problem. Clin Infect Dis 1995;20:16-23.<br />
92. Fang G, Keys TF, Gentry LO, et al. Prosthetic valve endocarditis resulting<br />
from noso<strong>com</strong>ial bacteremia: a prospective, multicenter study. Ann<br />
Intern Med 1993;119:560-7.<br />
93. Casey LC, Balk RA, Bone RC. Plasma cytokine and endotoxin levels<br />
correlate with survival in patients with the sepsis syndrome. Ann Intern<br />
Med 1993;119:771-8.<br />
94. Chesney PJ, Davis JP, Purdy WK, Wand PJ, Chesney RW. Clinical<br />
manifestations of toxic shock syndrome. JAMA 1981;246:741-8.<br />
95. Chambers HF. Methicillin resistance in staphylococci: molecular and<br />
biochemical basis and clinical implications. Clin Microbiol Rev 1997;10:<br />
781-91.<br />
96. Archer GL, Niemeyer DM. Origin and evolution of DNA associated<br />
with resistance to methicillin in staphylococci. Trends Microbiol 1994;2:<br />
343-7.<br />
97. Kreiswirth B, Kornblum J, Arbeit RD, et al. Evidence for a clonal origin<br />
of methicillin resistance in <strong>Staphylococcus</strong> <strong>aureus</strong>. Science 1993;259:227-30.<br />
98. Musser JM, Kapur V. Clonal analysis of methicillin-resistant <strong>Staphylococcus</strong><br />
<strong>aureus</strong> strains from intercontinental sources: association of the mec<br />
gene with divergent phylogenetic lineages implies dissemination by horizontal<br />
transfer and re<strong>com</strong>bination. J Clin Microbiol 1992;30:2058-63.<br />
99. Schwalbe RS, Stapleton JT, Gilligan PH. Emergence of van<strong>com</strong>ycin resistance<br />
in coagulase-negative staphylococci. N Engl J Med 1987;316:927-31.<br />
100. Noble WC, Virani Z, Cree RG. Co-transfer of van<strong>com</strong>ycin and other<br />
resistance genes from Enterococcus faecalis NCTC 12201 to <strong>Staphylococcus</strong><br />
<strong>aureus</strong>. FEMS Microbiol Lett 1992;72:195-8.<br />
101. Update: <strong>Staphylococcus</strong> <strong>aureus</strong> with reduced susceptibility to van<strong>com</strong>ycin<br />
— United States, 1997. MMWR Morb Mortal Wkly Rep 1997;46:<br />
813-5. [Erratum, MMWR Morb Mortal Wkly Rep 1997;46:851.]<br />
102. Sieradzki K, Tomasz A. Inhibition of cell wall turnover and autolysis<br />
Volume 339 Number 8 · 531<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine<br />
by van<strong>com</strong>ycin in a highly van<strong>com</strong>ycin-resistant mutant of <strong>Staphylococcus</strong><br />
<strong>aureus</strong>. J Bacteriol 1997;179:2557-66.<br />
103. Tenover FC, Lancaster MV, Hill BC, et al. Characterization of staphylococci<br />
with reduced susceptibilities to van<strong>com</strong>ycin and other glycopeptides.<br />
J Clin Microbiol 1998;36:1020-7.<br />
104. Levine DP, Fromm BS, Reddy BR. Slow response to van<strong>com</strong>ycin or<br />
van<strong>com</strong>ycin plus rifampin in methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong><br />
endocarditis. Ann Intern Med 1991;115:674-80.<br />
105. Karchmer AW. <strong>Staphylococcus</strong> <strong>aureus</strong> and van<strong>com</strong>ycin: the sequel.<br />
Ann Intern Med 1991;115:739-41.<br />
106. Michel M, Gutmann L. Methicillin-resistant <strong>Staphylococcus</strong> <strong>aureus</strong><br />
and van<strong>com</strong>ycin-resistant enterococci: therapeutic realities and possibilities.<br />
Lancet 1997;349:1901-6.<br />
107. Trucksis M, Hooper DC, Wolfson JS. Emerging resistance to fluoroquinolones<br />
in staphylococci: an alert. Ann Intern Med 1991;114:424-6.<br />
108. Miller MH, Wexler MA, Steigbigel NH. Single and <strong>com</strong>bination<br />
antibiotic therapy of <strong>Staphylococcus</strong> <strong>aureus</strong> experimental endocarditis: emergence<br />
of gentamicin-resistant mutants. Antimicrob Agents Chemother<br />
1978;14:336-43.<br />
109. Korzeniowski O, Sande MA, National Collaborative Study Group.<br />
Combination antimicrobial therapy for <strong>Staphylococcus</strong> <strong>aureus</strong> endocarditis<br />
in patients addicted to parenteral drugs and in nonaddicts: a prospective<br />
study. Ann Intern Med 1982;97:496-503.<br />
110. Wilson WR, Karchmer AW, Dajani AS, et al. Antibiotic treatment of<br />
adults with infective endocarditis due to streptococci, enterococci, staphylococci,<br />
and HACEK microorganisms. JAMA 1995;274:1706-13.<br />
111. Dworkin RJ, Lee BL, Sande MA, Chambers HF. Treatment of rightsided<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> endocarditis in intravenous drug abusers with<br />
ciprofloxacin and rifampicin. Lancet 1989;2:1071-3.<br />
112. Rahal JJ Jr, Chan Y-K, Johnson G. Relationship of staphylococcal<br />
tolerance, teichoic acid antibody, and serum bactericidal activity to therapeutic<br />
out<strong>com</strong>e in <strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia. Am J Med 1986;81:<br />
43-52.<br />
113. Chambers HF. Short-course <strong>com</strong>bination and oral therapies of <strong>Staphylococcus</strong><br />
<strong>aureus</strong> endocarditis. Infect Dis Clin North Am 1993;7:69-80.<br />
114. Ribera E, Gómez-Jimenez J, Cortes E, et al. Effectiveness of cloxacillin<br />
with and without gentamicin in short-term therapy for right-sided<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> endocarditis: a randomized, controlled trial. Ann<br />
Intern Med 1996;125:969-74.<br />
115. Heldman AW, Hartert TV, Ray SC, et al. Oral antibiotic treatment of<br />
right-sided staphylococcal endocarditis in injection drug users: prospective<br />
randomized <strong>com</strong>parison with parenteral therapy. Am J Med 1996;101:68-76.<br />
116. Dugdale DC, Ramsey PG. <strong>Staphylococcus</strong> <strong>aureus</strong> bacteremia in<br />
patients with Hickman catheters. Am J Med 1990;89:137-41.<br />
117. Yu VL, Fang GD, Keys TF, et al. Prosthetic valve endocarditis: superiority<br />
of surgical valve replacement versus medical therapy only. Ann<br />
Thorac Surg 1994;58:1073-7.<br />
118. Takei S, Arora YK, Walker SM. Intravenous immunoglobulin contains<br />
specific antibodies inhibitory to activation of T cells by staphylococcal<br />
toxin superantigens. J Clin Invest 1993;91:602-7.<br />
119. Reagan DR, Doebbeling BN, Pfaller MA, et al. Elimination of<br />
coincident <strong>Staphylococcus</strong> <strong>aureus</strong> nasal and hand carriage with intranasal application<br />
of mupirocin calcium ointment. Ann Intern Med 1991;114:101-6.<br />
120. Moy JA, Caldwell-Brown D, Lin AN, Pappa KA, Carter DM. Mupirocin-resistant<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> after long-term treatments of patients<br />
with epidermolysis bullosa. J Am Acad Dermatol 1990;22:893-5.<br />
121. Fattom AI, Sarwar J, Ortiz A, Naso R. A <strong>Staphylococcus</strong> <strong>aureus</strong> capsular<br />
polysaccharide (CP) vaccine and CP-specific antibodies protect mice<br />
against bacterial challenge. Infect Immun 1996;64:1659-65.<br />
122. Lee JC, Park J-S, Shepherd SE, Carey V, Fattom A. Protective efficacy<br />
of antibodies to the <strong>Staphylococcus</strong> <strong>aureus</strong> type 5 capsular polysaccharide<br />
in a modified model of endocarditis in rats. Infect Immun 1997;65:<br />
4146-51.<br />
123. Balaban N, Goldkorn T, Nhan RT, et al. Autoinducer of virulence as<br />
a target for vaccine and therapy against <strong>Staphylococcus</strong> <strong>aureus</strong>. Science 1998;<br />
280:438-40.<br />
124. Interim guidelines for prevention and control of staphylococcal infection<br />
associated with reduced susceptibility to van<strong>com</strong>ycin. MMWR Morb<br />
Mortal Wkly Rep 1997;46:626-8, 635.<br />
125. Edmond MB, Wenzel RP, Pasculle AW. Van<strong>com</strong>ycin-resistant <strong>Staphylococcus</strong><br />
<strong>aureus</strong>: perspectives on measures needed for control. Ann Intern<br />
Med 1996;124:329-34.<br />
532 · August 20, 1998<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
New England Journal of Medicine<br />
CORRECTION<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> <strong>Infections</strong><br />
To the Editor: In his review of <strong>Staphylococcus</strong> <strong>aureus</strong> infections, Dr.<br />
Lowy (Aug.<br />
20 issue) 1 states that bacteremia involving methicillinresistant<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> (MRSA) is not associated with<br />
higher mortality than bacteremia involving methicillin-susceptible S.<br />
<strong>aureus</strong> (MSSA). However, Romero-Vivas et al., 2 who conducted the<br />
largest study, noted a significantly higher fatality rate among patients<br />
with MRSA bacteremia. In their <strong>com</strong>parison of 100 cases of MSSA<br />
bacteremia and 84 cases of MRSA bacteremia, the mortality rates<br />
were 32 percent and 58.3 percent, respectively (P
New England Journal of Medicine<br />
4. Wood MJ. The <strong>com</strong>parative efficacy and safety of teicoplanin<br />
and van<strong>com</strong>ycin. J Antimicrob Chemother 1996;37:209-222.<br />
[Erratum, J Antimicrob Chemother 1996;38:919; J Antimicrob<br />
Chemother 1997;40:147.]<br />
To the Editor: In his splendid review of S. <strong>aureus</strong> infections, Lowy<br />
discusses life-threatening infections. Although he states that patients<br />
with human immunodeficiency virus (HIV) infection are at increased<br />
risk for staphylococcal colonization, he does not detail the peculiar<br />
characteristics of this infection in such patients. S. <strong>aureus</strong> pneumonia<br />
has been reported to occur in HIV-infected patients at a frequency<br />
exceeding that in the general population. 1<br />
We conducted a retrospective case–control study in the department of<br />
infectious diseases of a 1700-bed university hospital in Rome. For the<br />
period from 1986 through 1997, we identified 350 episodes of bacterial<br />
pneumonia (as defined elsewhere 2 ) and 28 episodes of S. <strong>aureus</strong><br />
pneumonia. The attack rate for S. <strong>aureus</strong> pneumonia was 8.31 cases<br />
per 1000 HIV-related hospital admissions. S. <strong>aureus</strong> pneumonia was<br />
a <strong>com</strong>munity-acquired infection in two thirds of the HIV-positive patients,<br />
a finding at variance with the frequently reported finding that in<br />
immuno<strong>com</strong>petent patients, a noso<strong>com</strong>ial origin of S. <strong>aureus</strong> pneumonia<br />
is more <strong>com</strong>mon.<br />
In conclusion, we emphasize the importance of S. <strong>aureus</strong> as an etiologic<br />
agent of life-threatening pulmonary infections in HIV-positive<br />
persons. Although other microorganisms can cause pneumonia, HIVpositive<br />
patients who have an acute onset with lobar involvement and<br />
pleural effusion on chest radiography should be carefully evaluated<br />
for the possibility of S. <strong>aureus</strong> pneumonia.<br />
Evelina Tacconelli, M.D.<br />
Mario Tumbarello, M.D.<br />
Roberto Cauda, M.D.<br />
Università Cattolica Sacro Cuore<br />
00168 Rome, Italy<br />
References<br />
1. Tumbarello M, Tacconelli E, Lucia MB, Cauda R, Ortona L. Predictors<br />
of <strong>Staphylococcus</strong> <strong>aureus</strong> pneumonia associated with human<br />
immunodeficiency virus infection. Respir Med 1996;90:531-537.<br />
2. Tumbarello M, Tacconelli E, de Gaetano K, et al. Bacterial pneumonia<br />
in HIV-infected patients: analysis of risk factors and prognostic<br />
indicators. J Acquir Immune Defic Syndr Hum Retrovirol<br />
1998;18:39-45.<br />
Dr. Lowy replies:<br />
To the Editor: Blot et al. cite several studies suggesting that the out<strong>com</strong>e<br />
of infections caused by MRSA is worse than that of infections<br />
caused by MSSA. Other reports argue against the greater virulence<br />
of MRSA strains. 1,2 As Blot et al.<br />
note, these studies must be interpreted<br />
cautiously, because of the frequent association of MRSA<br />
infections with a greater severity of illness, an underlying disease of<br />
a different nature, prolonged hospitalization, and increased antibiotic<br />
use. These variables make <strong>com</strong>parative analyses difficult, especially<br />
for retrospective studies.<br />
The virulence of staphylococcal infection<br />
may be more closely tied to particular strains than to the presence or<br />
absence of methicillin resistance.<br />
As Dr. Conde suggests, teicoplanin was not mentioned because it<br />
is not available in the United States. Although it has some pharmacologic<br />
advantages, teicoplanin has been reported to have less antistaphylococcal<br />
activity than van<strong>com</strong>ycin, or at best, similar activity. 3<br />
Tacconelli et al. describe an important presentation of staphylococcal<br />
disease in HIV-positive patients. The incidence of staphylococcal<br />
disease in general appears to be increased in this population.<br />
There have also been reports of an increased incidence of bloodstream,<br />
skin, and soft-tissue infections, as well as respiratory tract<br />
infections. 4,5 The basis of these infections is uncertain, but it may<br />
be related to the immuno<strong>com</strong>promised status of the patients, an increased<br />
colonization rate, and the use of more frequent invasive procedures<br />
that breach skin or mucosal barriers.<br />
There is an error on page 520 of my article (first column, last paragraph,<br />
second line). The size of the chromosome should be 2.8<br />
megabase pairs, not 2800 base pairs.<br />
Franklin D. Lowy, M.D.<br />
Montefiore Medical Center<br />
Bronx, NY 10467<br />
References<br />
1. French GL, Cheng AF, Ling JM, Mo P, Donnan S. Hong Kong<br />
strains of methicillin-resistant and methicillin-sensitive <strong>Staphylococcus</strong><br />
<strong>aureus</strong> have similar virulence. J Hosp Infect 1990;15:117-<br />
125.<br />
2. Harbath S, Rutschmann O, Sudre P, Pittet D. Impact of methicillin<br />
resistance on the out<strong>com</strong>e of patients with bacteremia caused by<br />
<strong>Staphylococcus</strong> <strong>aureus</strong>. Arch Intern Med 1998;158:182-189.<br />
3. Chambers HF. Parenteral antibiotics for the treatment of bacteremia<br />
and other serious staphylococcal infections. In: Crossley<br />
KB, Archer GL, eds. The staphylococci in human disease. New<br />
York: Churchill Livingstone, 1997:583-601.<br />
4. Weinke T, Schiller R, Fehrenbach FJ, Pohle HD. Association between<br />
<strong>Staphylococcus</strong> <strong>aureus</strong> nasopharyngeal colonization and<br />
septicemia in patients infected with human immunodeficiency<br />
virus. Eur J Clin Microbiol Infect Dis 1992;11:985-989.<br />
5. Krumholz HM, Sande MA, Lo B. Community-acquired bacteremia<br />
in patients with acquired immunodeficiency syndrome:<br />
clinical<br />
N Engl J Med 1998;339:2025<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.
New England Journal of Medicine<br />
presentation, bacteriology, and out<strong>com</strong>e. Am J Med 1989;86:776-<br />
779.<br />
N Engl J Med 1998;339:2025<br />
Downloaded from www.nejm.org at ARIZONA HEALTH INFORMATION NETWORK on December 7, 2009 .<br />
Copyright © 1998 Massachusetts Medical Society. All rights reserved.