2012 HMO Schedule of Benefits for CVS Caremark - Health Net
2012 HMO Schedule of Benefits for CVS Caremark - Health Net
2012 HMO Schedule of Benefits for CVS Caremark - Health Net

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
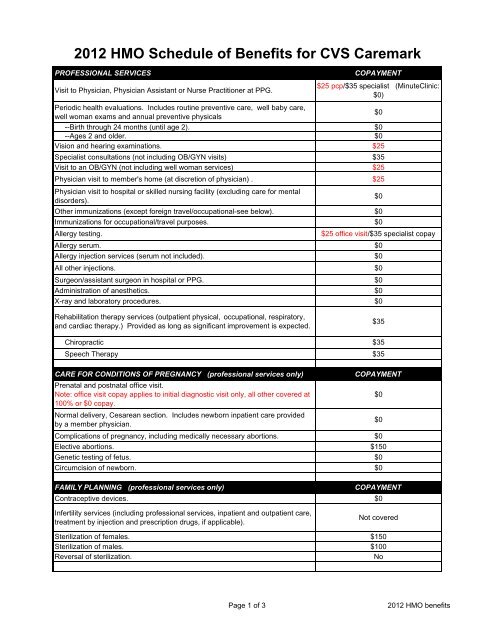
<strong>2012</strong> <strong>HMO</strong> <strong>Schedule</strong> <strong>of</strong> <strong>Benefits</strong> <strong>for</strong> <strong>CVS</strong> <strong>Caremark</strong><br />
PROFESSIONAL SERVICES<br />
COPAYMENT<br />
Visit to Physician, Physician Assistant or Nurse Practitioner at PPG.<br />
$25 pcp/$35 specialist (MinuteClinic:<br />
$0)<br />
Periodic health evaluations. Includes routine preventive care, well baby care,<br />
well woman exams and annual preventive physicals<br />
$0<br />
--Birth through 24 months (until age 2). $0<br />
--Ages 2 and older. $0<br />
Vision and hearing examinations. $25<br />
Specialist consultations (not including OB/GYN visits) $35<br />
Visit to an OB/GYN (not including well woman services) $25<br />
Physician visit to member's home (at discretion <strong>of</strong> physician) . $25<br />
Physician visit to hospital or skilled nursing facility (excluding care <strong>for</strong> mental<br />
disorders).<br />
$0<br />
Other immunizations (except <strong>for</strong>eign travel/occupational-see below). $0<br />
Immunizations <strong>for</strong> occupational/travel purposes. $0<br />
Allergy testing.<br />
$25 <strong>of</strong>fice visit/$35 specialist copay<br />
Allergy serum. $0<br />
Allergy injection services (serum not included). $0<br />
All other injections. $0<br />
Surgeon/assistant surgeon in hospital or PPG. $0<br />
Administration <strong>of</strong> anesthetics. $0<br />
X-ray and laboratory procedures. $0<br />
Rehabilitation therapy services (outpatient physical, occupational, respiratory,<br />
and cardiac therapy.) Provided as long as significant improvement is expected.<br />
$35<br />
Chiropractic $35<br />
Speech Therapy $35<br />
CARE FOR CONDITIONS OF PREGNANCY (pr<strong>of</strong>essional services only)<br />
COPAYMENT<br />
Prenatal and postnatal <strong>of</strong>fice visit.<br />
Note: <strong>of</strong>fice visit copay applies to initial diagnostic visit only, all other covered at<br />
$0<br />
100% or $0 copay.<br />
Normal delivery, Cesarean section. Includes newborn inpatient care provided<br />
by a member physician.<br />
$0<br />
Complications <strong>of</strong> pregnancy, including medically necessary abortions. $0<br />
Elective abortions. $150<br />
Genetic testing <strong>of</strong> fetus. $0<br />
Circumcision <strong>of</strong> newborn. $0<br />
FAMILY PLANNING (pr<strong>of</strong>essional services only)<br />
COPAYMENT<br />
Contraceptive devices. $0<br />
Infertility services (including pr<strong>of</strong>essional services, inpatient and outpatient care,<br />
treatment by injection and prescription drugs, if applicable).<br />
Not covered<br />
Sterilization <strong>of</strong> females. $150<br />
Sterilization <strong>of</strong> males. $100<br />
Reversal <strong>of</strong> sterilization.<br />
No<br />
Page 1 <strong>of</strong> 3 <strong>2012</strong> <strong>HMO</strong> benefits
OTHER SERVICES<br />
COPAYMENT<br />
Medical social services. $0<br />
Patient education. $0<br />
Ground ambulance $0<br />
Air ambulance $0<br />
Durable medical equipment. $5000 plan year max $0<br />
Orthotics (braces and supports) $0<br />
Custom footwear.<br />
Not covered<br />
Diabetic supplies (except footwear) $0<br />
Diabetic footwear $0<br />
Hearing aids. Combined with Durable Medical Equipment plan year max $0<br />
Prosthesis (replacing body parts). $0<br />
Blood, blood plasma, blood factors and blood derivatives. $0<br />
Nuclear medicine (pr<strong>of</strong>essional services only). $0<br />
Organ and bone marrow transplants (non-experimental and non-investigative.<br />
Pr<strong>of</strong>essional services only).<br />
$0<br />
Chemotherapy (pr<strong>of</strong>essional services only). $0<br />
Renal dialysis (pr<strong>of</strong>essional services only). $0<br />
Home health visit. 100 visits per plan year. $25<br />
Hospice care $0<br />
HOSPITAL AND SKILLED NURSING FACILITY SERVICES<br />
COPAYMENT<br />
Unlimited days <strong>of</strong> hospital care in a semi-private room or ICU with ancillary<br />
services. Excludes care <strong>for</strong> mental disorders.<br />
$250 per admission<br />
Confinement in a skilled nursing facility. 100 days per plan year $0<br />
Maternity care. Includes routine nursery charges.<br />
$250 per admission<br />
Outpatient services, excluding surgery. $0<br />
Outpatient surgery at hospital or ambulatory surgical center. $0<br />
EMERGENCY CARE/URGENTLY NEEDED CARE<br />
COPAYMENT<br />
The copayment will not be required if the member is admitted as a hospital inpatient directly from the emergency room<br />
or urgent care center<br />
Use <strong>of</strong> emergency room (facility and pr<strong>of</strong>essional services). $125<br />
Use <strong>of</strong> urgent care center (facility and pr<strong>of</strong>essional services). $35<br />
OUT OF POCKET MAXIMUM<br />
COPAYMENT<br />
Single contract. $1,000<br />
Two-party contract. $2,000<br />
Family contract (3 or more members). $3,000<br />
CHEMICAL DEPENDENCY REHABILITATION and CARE <strong>for</strong> MENTAL DISORDERS<br />
Severe Mental Illnesses (1)<br />
Outpatient<br />
Outpatient copay $25<br />
Maximum visits per calendar year<br />
Unlimited<br />
Inpatient<br />
Inpatient care in hospital or residential treatment facility<br />
$250 copay per admission<br />
Maximum days per calendar year<br />
Unlimited<br />
Physician visit to hospital or residential treatment facility $0<br />
Other Mental Illnesses<br />
Outpatient<br />
Outpatient copay $25<br />
Maximum visits per calendar year<br />
Unlimited<br />
Page 2 <strong>of</strong> 3 <strong>2012</strong> <strong>HMO</strong> benefits
CHEMICAL DEPENDENCY REHABILITATION and CARE <strong>for</strong> MENTAL DISORDERS (continued)<br />
Inpatient<br />
Inpatient care in hospital or residential treatment facility<br />
$250 copay per admission<br />
Maximum days per calendar year<br />
Unlimited<br />
Physician visit to hospital or residential treatment facility $0<br />
CHEMICAL DEPENDENCY REHABILITATION and CARE <strong>for</strong> MENTAL DISORDERS (continued)<br />
Chemical Dependency Rehabilitation<br />
Outpatient<br />
Individual therapy session $25<br />
Group therapy session 12.50<br />
Maximum visits per calendar year<br />
Unlimited<br />
Detoxification<br />
Inpatient<br />
Chemical dependency rehabilitation<br />
Maximum days per calendar year<br />
$250 copay per admission<br />
$250 copay per admission<br />
n/a<br />
Page 3 <strong>of</strong> 3 <strong>2012</strong> <strong>HMO</strong> benefits