Case presentation
Case presentation
Case presentation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>Case</strong> <strong>presentation</strong><br />
Dr. W.S. Ng<br />
Dr. K.P. Yau<br />
1
• 00:20<br />
• Phone call from ambulance<br />
• M/74 OAHR<br />
• c/o SOB and labored breathing with SaO2<br />
40%<br />
• Will arrive AED in 10 minutes time<br />
2
• On arrival, vital signs<br />
• BP 92/52<br />
• P 129<br />
• SaO2 59% on non-rebreathing mask<br />
• RR 30<br />
• Temp 35.7<br />
• GCS E4V5M6<br />
3
What to do next?<br />
4
Proceed to RSI for<br />
mechanical ventilation<br />
immediately?<br />
What’s in your mind?<br />
5
Differential diagnosis<br />
• Pulmonary<br />
• Asthma, COAD, PE, pneumothorax, pleural<br />
effusion, pneumonia, interstitial lung disease…<br />
• Cardiac<br />
• ACS, CHF, Cardiac tamponade<br />
• Psychogenic<br />
• Hyperventilation, panic attack<br />
• Others<br />
• anemia, anaphylaxis, endocrine, acidosis…<br />
6
• Approach by ABC<br />
• P/E<br />
• Tachypnoic<br />
• Can hardly speak<br />
• Air entry was present both sides but shallow<br />
• Bilateral crepitations at lung base<br />
• Trachea central<br />
• No stridor<br />
• No ankle edema<br />
7
What to do next?<br />
8
Investigations<br />
• ECG<br />
• At Arterial lblood gas<br />
• CXR<br />
• H’stix<br />
• Any other bedside investigations help you making<br />
decision?<br />
9
• See USG<br />
• http://vimeo.com/1025553<br />
12
Sliding sign<br />
Comet tail artifact<br />
13
Sea shore sign<br />
Barcode sign<br />
14
Now patient got Type 2<br />
respiratory failure<br />
What next? Intubation? How?<br />
15
RSI<br />
• General anaesthesia induced by a rapid acting IV induction agent and a rapid<br />
acing muscle relaxant with application of cricoid pressure<br />
• 7P<br />
• Preparation<br />
• prepare all necessary equipment, drugs and back-up plans<br />
• Preoxygenation<br />
• with 100% oxygen, replace nitrogen in the functional residual capacity (FRC) of the<br />
patient's lung with oxygen.<br />
• Premedication<br />
• depending on the patient<br />
• Paralyze +induction of anaesthesia<br />
• Suxamethonium, thiopentone, etomidate, ketamine…<br />
• Pass the tube<br />
• visualize the tube going through the vocal cords<br />
• Proof of placement<br />
• Post intubation care<br />
• secure the tube, ventilate<br />
16
• RSI<br />
• Suxamethonium 75mg<br />
• Etomidate 15mg<br />
• Size 7.5ETT at 22cm first go<br />
• Post intubation<br />
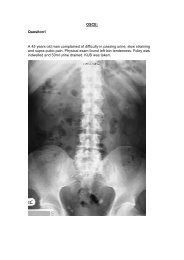
• CXR<br />
• Bilateral diffuse lung fibrosis, no pneumothorax, ETT in situ.<br />
• SaO2 99%<br />
• ETCO2 38<br />
• BP 142/100mmHg P 127<br />
• ICU consulted<br />
• unlikely l to benefit from ICU care<br />
• Admitted to general ward<br />
17
Post intubation ti Xray<br />
18
Progress<br />
• Extubate on the same day due to patient’s<br />
discomfort and irreverible cause.<br />
• Passed away on same day.<br />
• Family members did not satisfy with the<br />
decision of intubation as the patient would<br />
feel discomfort and pain.<br />
• They also disagree on the decision of active<br />
resuscitation and they think that it actually<br />
prolong suffering of Mr. Lo<br />
19
What do you think?<br />
Will you resuscitate the patient<br />
when you are the case MO?<br />
20
• PHx.<br />
• Retired businessman<br />
• Interstitial lung disease dx.2008 in GH On LTOT<br />
5L/min<br />
• PHT<br />
• Gout<br />
• Gall stone<br />
• Chair bound<br />
• OAHR since 8/2010<br />
21
• Hx. Of NIV in UCH<br />
• Very distressing to him<br />
• Refuse any invasive procedure to prolong<br />
dying<br />
• Patient and family opt for DNR in Sept.2010<br />
• “DNR” written in CMS ALERT<br />
25
Pulmonary Fibrosis<br />
26
Pulmonary fibrosis<br />
• Scarring in the lung<br />
• Causes:<br />
• Secondary to<br />
• Chronic inflammation<br />
• sarcoidosis<br />
• Infections<br />
• Environmental agents<br />
• asbestos, silica, exposure to certain gases<br />
• Ionizing radiation<br />
• radiation therapy to treat tumors<br />
• drugs<br />
• Nitrofurantoin, t i methotrexate, t t amiodarone…<br />
• Hypersensitivity pneumonitis<br />
• inhaling dust contaminated with bacterial, fungal, or animal<br />
products<br />
• Idiopathic pulmonary fibrosis (IPF) 27
Diagnosis<br />
• Progressive shortness of breath, cough, and<br />
diminished i i d exercise tolerance<br />
• P/E: Fine inspiratory crackles at the lung bases<br />
• CXR<br />
• Lung function test<br />
• Restrictive lung disease, FEV1and FVC are reduced so the<br />
FEV1/FVC ratio normal or increase<br />
• high-resolution CT<br />
• confirmed by lung biopsy<br />
28
Complications<br />
• Pulmonary hypertension<br />
• Heart failure of the right ventrible<br />
29
Treatment<br />
• limited treatment options<br />
• Corticosteroids, colchicine or<br />
immunosuppressant for some type<br />
• No evidence that any medications can help<br />
this condition (IPF)<br />
• because scarring is permanent once it has<br />
developed<br />
• Lung transplantation is the only therapeutic<br />
option available<br />
30
Prognosis<br />
• Life expectancy 2-5 years after diagnosis<br />
• Factors lengthen the life expectancy<br />
• A younger age (under 50 years old)<br />
• Female<br />
• Symptoms that began less than one year<br />
• If the pulmonary fibrosis i is associated with certain diseases<br />
(such as systemic sclerosis) compared to idiopathic<br />
pulmonary fibrosis<br />
• Minimal SOB at diagnosis<br />
• Less lung damage based on the high-resolution CT (HRCT)<br />
at the time of diagnosis<br />
• A positive response to treatment after three to six months<br />
31
Now you know the<br />
history and DNR<br />
Will you resuscitate the patient?<br />
And why?<br />
32
Guideline<br />
33
HAHO guideline on in-hospital<br />
resuscitation<br />
• Enable us to arrive at professionally and ethically<br />
sound resuscitation ti decision i and safeguard the best<br />
interests of the patient and clinician<br />
• Before arriving resuscitation decision<br />
• Consider ethical principles<br />
p<br />
• P. of beneficence<br />
• P. of nonmaleficience<br />
• P. of patient autonomy<br />
• P. of medical futility<br />
• P. of non-abandonment<br />
34
• Resuscitation decision should be based on<br />
• Patient’s medical condition<br />
• Overall treatment plan<br />
• Likelihood of patient benefit<br />
• Patient’s wishes<br />
• Should be initiated by doctor IC with his team<br />
members and review at regular interval or<br />
when there’s change in patient’s condition.<br />
35
DNR<br />
Ambulance Command<br />
Standing Orders<br />
ACP & AD<br />
36
• DNR<br />
• Forego resuscitation measures include chest compression,<br />
assisted ventilation, ETT, defibrillation, and using<br />
cardiotonic drugs regarding g patient’s decision/condition<br />
• Not affect the provision of life sustaining measures like<br />
artificial nutrition, hydration or other emergency care such<br />
as treatment t t of pain, haemorrhage, h dyspnoea, etc<br />
• Effective to that particular period only<br />
• Based on clinical i l judgment at a specific time point,<br />
• Need periodic review.<br />
• Unlikely l to be applicable to other clinicians i i and across<br />
medical institutions<br />
37
• Ambulance Command Standing Orders<br />
• There’s existing arrangement for HA terminal<br />
oncology pediatric patient between FSD and HA<br />
• Stating patient’s grave illness and agreement by<br />
parents known to both FSD and HA,<br />
• Will not be resuscitated if fall into Cardiac arrest.<br />
40
Advance Directives &<br />
Advance Care Planning<br />
41
• Advance Directives (AD)<br />
• Back in 2004, the Law Reform Commission recommended the<br />
concept of AD to medical treatment.<br />
• The Government accepted the Concept of Advance Directives<br />
under the common law framework but was not prepared to make<br />
AD statutory.<br />
• AD’s implemented July, 2010<br />
• A valid AD is legally binding,<br />
• Applicable across medical institutions if its validity can be<br />
ascertained on the spot.<br />
• A proxy health care directive does not have legal status in HK<br />
42
• Operation of AD<br />
• Terminally ill<br />
• In a state of irreversible coma<br />
• Persistent vegetative state<br />
43
• Advanced Care Plan (ACP)<br />
• A process enabling a patient t to express wishes<br />
about his or her future health care in consultation<br />
with their health care providers, family members and<br />
other important people in their lives.<br />
• Based on patient t autonomy and patient t consent, to<br />
help ensure that the concept of consent is respected<br />
if the patient becomes incapable of participating in<br />
treatment decisions.<br />
• ACP is traceable to specific doctor-patient<br />
relationship<br />
44
Thank you<br />
45