Heart disease in tHe fire service - West Valley City Firefighters, IAFF ...
Heart disease in tHe fire service - West Valley City Firefighters, IAFF ...
Heart disease in tHe fire service - West Valley City Firefighters, IAFF ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Heart</strong> Disease <strong>in</strong> the Fire Service<br />
cHaPter 5 • risk factOrs fOr <strong>Heart</strong> <strong>disease</strong><br />
Sudden cardiac death is the lead<strong>in</strong>g<br />
cause of on-duty deaths among <strong>fire</strong><br />
fighters. i The vast majority of these cases<br />
are due to coronary heart <strong>disease</strong> (CHD). ii<br />
Research has identified multiple risk<br />
factors <strong>in</strong> the general population for<br />
develop<strong>in</strong>g CHD that are universally<br />
accepted. Additionally, <strong>fire</strong> fighters face<br />
special occupational exposures and<br />
hazards that may contribute to the risk of<br />
CHD, and some of these exposures have<br />
been shown to <strong>in</strong>crease the odds of<br />
trigger<strong>in</strong>g acute cardiovascular events that<br />
can lead to premature retirement and<br />
death. Many of the standard CHD risk<br />
factors for the general population were<br />
derived from large scale, prospective<br />
cohort studies, such as the Fram<strong>in</strong>gham<br />
<strong>Heart</strong> Study and Nurses’ Health Study.<br />
Some CHD risk factors, like diet and<br />
physical activity, can be improved or<br />
worsened by changes <strong>in</strong> behavior, lifestyle<br />
and the work environment. Therefore,<br />
they are known as modifiable risk factors.<br />
Other risk factors, like age and gender,<br />
cannot be changed and are called<br />
non-modifiable risk factors. This chapter<br />
reviews major CHD risk factors,<br />
categoriz<strong>in</strong>g them <strong>in</strong>to standard risk<br />
factors- modifiable and non-modifiableand<br />
special occupational risk factors faced<br />
by <strong>fire</strong> fighters.<br />
STANDARD CHD RISKS<br />
IN FIRE FIGHTERS<br />
Studies of <strong>fire</strong> fighters who experience<br />
on-duty CHD events and premature<br />
retirements related to heart <strong>disease</strong> have<br />
identified several risk factors that are<br />
associated with an <strong>in</strong>creased probability<br />
or “odds ratio” of hav<strong>in</strong>g an on-duty<br />
CHD event. These are identical to many<br />
of the key risk factors previously<br />
identified dur<strong>in</strong>g research of the general<br />
population. Fire fighters who develop<br />
on-duty CHD events have an excess of<br />
these risk factors compared to <strong>fire</strong><br />
fighters who do not develop on-duty<br />
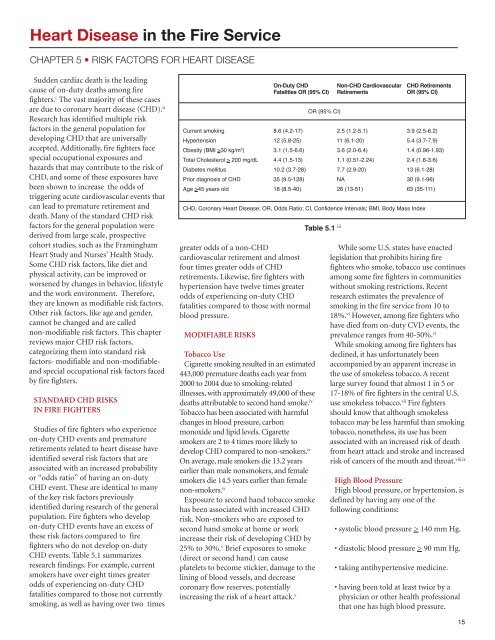
CHD events. Table 5.1 summarizes<br />
research f<strong>in</strong>d<strong>in</strong>gs. For example, current<br />
smokers have over eight times greater<br />
odds of experienc<strong>in</strong>g on-duty CHD<br />
fatalities compared to those not currently<br />
smok<strong>in</strong>g, as well as hav<strong>in</strong>g over two times<br />
greater odds of a non-CHD<br />
cardiovascular retirement and almost<br />
four times greater odds of CHD<br />
retirements. Likewise, <strong>fire</strong> fighters with<br />
hypertension have twelve times greater<br />
odds of experienc<strong>in</strong>g on-duty CHD<br />
fatalities compared to those with normal<br />
blood pressure.<br />
MODIFIABLE RISKS<br />
Tobacco Use<br />
Cigarette smok<strong>in</strong>g resulted <strong>in</strong> an estimated<br />
443,000 premature deaths each year from<br />
2000 to 2004 due to smok<strong>in</strong>g-related<br />
illnesses, with approximately 49,000 of these<br />
deaths attributable to second hand smoke. iv<br />
Tobacco has been associated with harmful<br />
changes <strong>in</strong> blood pressure, carbon<br />
monoxide and lipid levels. Cigarette<br />
smokers are 2 to 4 times more likely to<br />
develop CHD compared to non-smokers. iv<br />
On average, male smokers die 13.2 years<br />
earlier than male nonsmokers, and female<br />
smokers die 14.5 years earlier than female<br />
non-smokers. iv<br />
Exposure to second hand tobacco smoke<br />
has been associated with <strong>in</strong>creased CHD<br />
risk. Non-smokers who are exposed to<br />
second hand smoke at home or work<br />
<strong>in</strong>crease their risk of develop<strong>in</strong>g CHD by<br />
25% to 30%. v Brief exposures to smoke<br />
(direct or second hand) can cause<br />
platelets to become stickier, damage to the<br />
l<strong>in</strong><strong>in</strong>g of blood vessels, and decrease<br />
coronary flow reserves, potentially<br />
<strong>in</strong>creas<strong>in</strong>g the risk of a heart attack. v<br />
On-Duty CHD<br />
Non-CHD Cardiovascular CHD Retirements<br />
Fatalities OR (95% CI) Retirements OR (95% CI)<br />
OR (95% CI)<br />
Current smok<strong>in</strong>g 8.6 (4.2-17) 2.5 (1.2-5.1) 3.9 (2.5-6.2)<br />
Hypertension 12 (5.8-25) 11 (6.1-20) 5.4 (3.7-7.9)<br />
Obesity (BMI >30 kg/m 2 ) 3.1 (1.5-6.6) 3.6 (2.0-6.4) 1.4 (0.96-1.93)<br />
Total Cholesterol > 200 mg/dL 4.4 (1.5-13) 1.1 (0.51-2.24) 2.4 (1.6-3.6)<br />
Diabetes mellitus 10.2 (3.7-28) 7.7 (2.9-20) 13 (6.1-28)<br />
Prior diagnosis of CHD 35 (9.5-128) NA 30 (9.1-96)<br />
Age >45 years old 18 (8.5-40) 26 (13-51) 63 (35-111)<br />
CHD, Coronary <strong>Heart</strong> Disease; OR, Odds Ratio; CI, Confidence Intervals; BMI, Body Mass Index<br />
Table 5.1 iii<br />
While some U.S. states have enacted<br />
legislation that prohibits hir<strong>in</strong>g <strong>fire</strong><br />
fighters who smoke, tobacco use cont<strong>in</strong>ues<br />
among some <strong>fire</strong> fighters <strong>in</strong> communities<br />
without smok<strong>in</strong>g restrictions. Recent<br />
research estimates the prevalence of<br />
smok<strong>in</strong>g <strong>in</strong> the <strong>fire</strong> <strong>service</strong> from 10 to<br />
18%. vi However, among <strong>fire</strong> fighters who<br />
have died from on-duty CVD events, the<br />
prevalence ranges from 40-50%. vi<br />
While smok<strong>in</strong>g among <strong>fire</strong> fighters has<br />
decl<strong>in</strong>ed, it has unfortunately been<br />
accompanied by an apparent <strong>in</strong>crease <strong>in</strong><br />
the use of smokeless tobacco. A recent<br />
large survey found that almost 1 <strong>in</strong> 5 or<br />
17-18% of <strong>fire</strong> fighters <strong>in</strong> the central U.S.<br />
use smokeless tobacco. vii Fire fighters<br />
should know that although smokeless<br />
tobacco may be less harmful than smok<strong>in</strong>g<br />
tobacco, nonetheless, its use has been<br />
associated with an <strong>in</strong>creased risk of death<br />
from heart attack and stroke and <strong>in</strong>creased<br />
risk of cancers of the mouth and throat. viii,ix<br />
High Blood Pressure<br />
High blood pressure, or hypertension, is<br />
def<strong>in</strong>ed by hav<strong>in</strong>g any one of the<br />
follow<strong>in</strong>g conditions:<br />
• systolic blood pressure > 140 mm Hg.<br />
• diastolic blood pressure > 90 mm Hg.<br />
• tak<strong>in</strong>g antihypertensive medic<strong>in</strong>e.<br />
• hav<strong>in</strong>g been told at least twice by a<br />
physician or other health professional<br />
that one has high blood pressure.<br />
15