Parenteral Chemotherapy/Immunotherapy pre-printed order form
Parenteral Chemotherapy/Immunotherapy pre-printed order form
Parenteral Chemotherapy/Immunotherapy pre-printed order form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
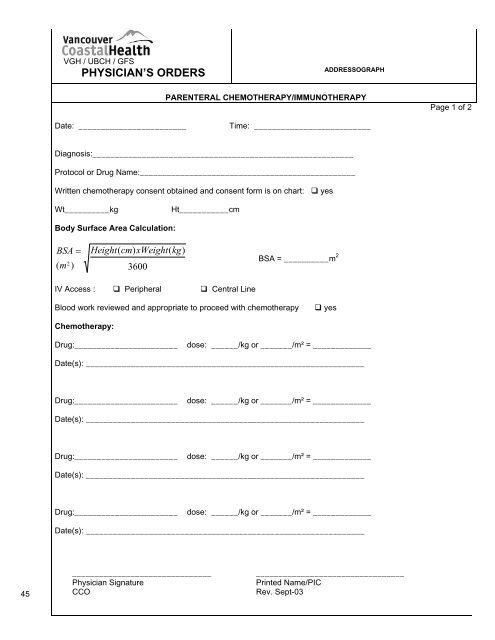
VGH / UBCH / GFS<br />
PHYSICIAN’S ORDERS<br />
ADDRESSOGRAPH<br />
PARENTERAL CHEMOTHERAPY/IMMUNOTHERAPY<br />
Page 1 of 2<br />
Date: ________________________<br />
Time: __________________________<br />
Diagnosis:__________________________________________________________<br />
Protocol or Drug Name:________________________________________________<br />
Written chemotherapy consent obtained and consent <strong>form</strong> is on chart: yes<br />
Wt__________kg<br />
Ht___________cm<br />
Body Surface Area Calculation:<br />
BSA =<br />
( m 2<br />
)<br />
Height( cm)<br />
xWeight(<br />
kg)<br />
3600<br />
BSA = __________m 2<br />
IV Access : Peripheral Central Line<br />
Blood work reviewed and appropriate to proceed with chemotherapy<br />
yes<br />
<strong>Chemotherapy</strong>:<br />
Drug:_______________________<br />
dose: ______/kg or _______/m² = _____________<br />
Date(s): ______________________________________________________________<br />
Drug:_______________________<br />
dose: ______/kg or _______/m² = _____________<br />
Date(s): ______________________________________________________________<br />
Drug:_______________________<br />
dose: ______/kg or _______/m² = _____________<br />
Date(s): ______________________________________________________________<br />
Drug:_______________________<br />
dose: ______/kg or _______/m² = _____________<br />
Date(s): ______________________________________________________________<br />
45<br />
_______________________________<br />
Physician Signature<br />
CCO<br />
_________________________________<br />
Printed Name/PIC<br />
Rev. Sept-03
VGH / UBCH / GFS<br />
PHYSICIAN’S ORDERS<br />
ADDRESSOGRAPH<br />
PARENTERAL CHEMOTHERAPY/IMMUNOTHERAPY<br />
Page 2 of 2<br />
Date: ________________________<br />
Time: __________________________<br />
Adjunctive Medications (including antiemetics):<br />
_______________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
________________________________________________________________________<br />
IV FLUIDS:_______________________________________________________________<br />
Bloodwork<br />
CBC + DIFF. + Platelets<br />
Lytes, Urea, Creatinine<br />
Magnesium/Calcium<br />
Bili T/D, AST, Alk Phos, LDH<br />
q____________<br />
q____________<br />
q____________<br />
q____________<br />
Other____________________ q____________<br />
Results to Dr. _________________________________<br />
45<br />
_______________________________<br />
Physician Signature<br />
CCO<br />
_________________________________<br />
Printed Name/PIC<br />
Rev. Sept-03