SAFETY ASSESSMENT FORM TOOL – HAZARD IDENTIFICATION
SAFETY ASSESSMENT FORM TOOL – HAZARD IDENTIFICATION
SAFETY ASSESSMENT FORM TOOL – HAZARD IDENTIFICATION

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Client Health Record #<br />
Client Surname<br />
Given Name<br />
Community Health Services<br />
<strong>SAFETY</strong> <strong>ASSESSMENT</strong> <strong>FORM</strong> <strong>TOOL</strong> –<br />
<strong>HAZARD</strong> <strong>IDENTIFICATION</strong><br />
Date of Birth<br />
Gender<br />
MFRN<br />
PHIN<br />
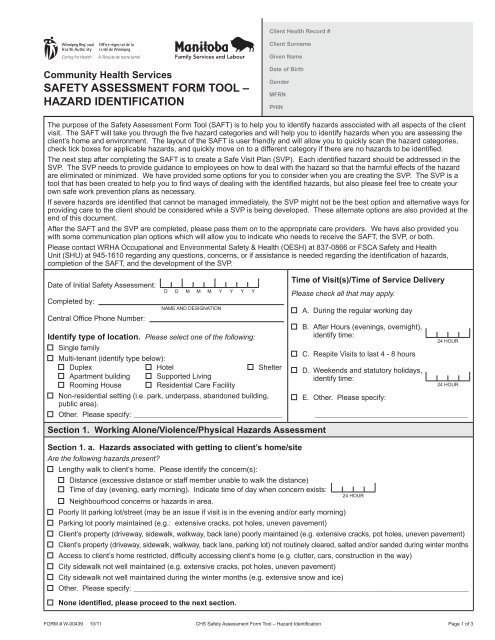
The purpose of the Safety Assessment Form Tool (SAFT) is to help you to identify hazards associated with all aspects of the client<br />
visit. The SAFT will take you through the five hazard categories and will help you to identify hazards when you are assessing the<br />
client’s home and environment. The layout of the SAFT is user friendly and will allow you to quickly scan the hazard categories,<br />
check tick boxes for applicable hazards, and quickly move on to a different category if there are no hazards to be identified.<br />
The next step after completing the SAFT is to create a Safe Visit Plan (SVP). Each identified hazard should be addressed in the<br />
SVP. The SVP needs to provide guidance to employees on how to deal with the hazard so that the harmful effects of the hazard<br />
are eliminated or minimized. We have provided some options for you to consider when you are creating the SVP. The SVP is a<br />
tool that has been created to help you to find ways of dealing with the identified hazards, but also please feel free to create your<br />
own safe work prevention plans as necessary.<br />
If severe hazards are identified that cannot be managed immediately, the SVP might not be the best option and alternative ways for<br />
providing care to the client should be considered while a SVP is being developed. These alternate options are also provided at the<br />
end of this document.<br />
After the SAFT and the SVP are completed, please pass them on to the appropriate care providers. We have also provided you<br />
with some communication plan options which will allow you to indicate who needs to receive the SAFT, the SVP, or both.<br />
Please contact WRHA Occupational and Environmental Safety & Health (OESH) at 837-0866 or FSCA Safety and Health<br />
Unit (SHU) at 945-1610 regarding any questions, concerns, or if assistance is needed regarding the identification of hazards,<br />
completion of the SAFT, and the development of the SVP.<br />
Date of Initial Safety Assessment:<br />
Completed by:<br />
Central Office Phone Number:<br />
D D M M M Y Y Y Y<br />
NAME AND DESIGNATION<br />
Identify type of location. Please select one of the following:<br />
Single family<br />
Multi-tenant (identify type below):<br />
Duplex Hotel Shelter<br />
Apartment building Supported Living<br />
Rooming House Residential Care Facility<br />
Non-residential setting (i.e. park, underpass, abandoned building,<br />
public area).<br />
Other. Please specify: ________________________________________________________<br />
Section 1. Working Alone/Violence/Physical Hazards Assessment<br />
Time of Visit(s)/Time of Service Delivery<br />
Please check all that may apply.<br />
A. During the regular working day<br />
B. After Hours (evenings, overnight),<br />
identify time:<br />
C. Respite Visits to last 4 - 8 hours<br />
D. Weekends and statutory holidays,<br />
identify time:<br />
E. Other. Please specify:<br />
24 HOUR<br />
24 HOUR<br />
____________________________________________________________<br />
Section 1. a. Hazards associated with getting to client’s home/site<br />
Are the following hazards present?<br />
Lengthy walk to client’s home. Please identify the concern(s):<br />
Distance (excessive distance or staff member unable to walk the distance)<br />
Time of day (evening, early morning). Indicate time of day when concern exists:<br />
24 HOUR<br />
Neighbourhood concerns or hazards in area.<br />
Poorly lit parking lot/street (may be an issue if visit is in the evening and/or early morning)<br />
Parking lot poorly maintained (e.g.: extensive cracks, pot holes, uneven pavement)<br />
Client’s property (driveway, sidewalk, walkway, back lane) poorly maintained (e.g. extensive cracks, pot holes, uneven pavement)<br />
Client’s property (driveway, sidewalk, walkway, back lane, parking lot) not routinely cleared, salted and/or sanded during winter months<br />
Access to client’s home restricted, difficulty accessing client’s home (e.g. clutter, cars, construction in the way)<br />
City sidewalk not well maintained (e.g. extensive cracks, pot holes, uneven pavement)<br />
City sidewalk not well maintained during the winter months (e.g. extensive snow and ice)<br />
Other. Please specify: ____________________________________________________________________________________________________________________________<br />
None identified, please proceed to the next section.<br />
<strong>FORM</strong> # W-00439 10/11 CHS Safety Assessment Form Tool – Hazard Identification Page 1 of 3
Client Health Record #<br />
Client Surname<br />
Given Name<br />
Community Health Services<br />
<strong>SAFETY</strong> <strong>ASSESSMENT</strong> <strong>FORM</strong> <strong>TOOL</strong> –<br />
<strong>HAZARD</strong> <strong>IDENTIFICATION</strong><br />
Date of Birth<br />
Gender<br />
MFRN<br />
PHIN<br />
Section 1. Working Alone/Violence/Physical Hazards Assessment (continued)<br />
Section 1. b. Reported/known/emerging site or neighborhood concerns.<br />
Please identify the concerns<br />
Gangs Solvent/alcohol/drug use, drug dealing/activity Weapons Observable street crime/history of crime<br />
Other. Please specify: ___________________________________________________________________________________________________________________________<br />
Are any of the above hazards impacted by the time of the day or day of the week? ................................................ No Yes<br />
If yes, please indicate time of day:<br />
24 HOUR<br />
None identified, please proceed to the next section.<br />
and Day of Week:<br />
Section 1. c. Abusive and Violent Behaviour<br />
Abusive or threatening behaviors that staff are exposed to:<br />
By whom Client, Type of abuse: Physical Verbal<br />
Family member, Relation to Client: _________________________ , Type of abuse: Physical Verbal<br />
Associate: lives in home................................... Type of abuse: Physical Verbal<br />
lives out of home............................. Type of abuse: Physical Verbal<br />
Neighbours........................................................................ Type of abuse: Physical Verbal<br />
None identified, please proceed to the next section.<br />
Section 1. d. Hazards Inside Client’s Home/Apartment<br />
Are the following hazards present in the home, check only those that are identified:<br />
Exits/doors are blocked<br />
Stairs poorly maintained, missing railing<br />
Floors are cracked, loose rugs, loose mats<br />
Cluttered work area affecting ability to perform tasks safely<br />
Cramped (lack of space) work area affecting ability to perform tasks safely<br />
Access to work area restricted or blocked<br />
Electrical appliances, other equipment required to perform tasks in poor working order<br />
Weapons (guns, knives) inside the home, visible and not safely stored<br />
Phone not available<br />
Other. Please specify: ___________________________________________________________________________________________________________________________<br />
None identified, please proceed to the next section.<br />
Section 1. e. Multi Tenant Dwellings Only<br />
Please fill in this section only if applicable, check only hazards that are identified. If not, please proceed to next section.<br />
Common stairs poorly maintained<br />
Poorly lit hallway/stairwell<br />
Common hallways are cluttered and full of debris<br />
Exits and emergency exits are not visible or marked<br />
Exits are blocked or non-functional<br />
The elevator is non-functional/requires excessive stair climbing<br />
A ‘buzzer’ system is not available/difficulty notifying client and entering building<br />
The external door is locked during the day (cannot notify client or gain access to building)<br />
There are no security cameras or a security guard on site/assistance not available in an emergency<br />
Phone on site not available to staff/cannot call for help in an emergency<br />
Other. Please specify: ___________________________________________________________________________________________________________________________<br />
None identified, please proceed to the next section.<br />
<strong>FORM</strong> # W-00439 10/11 CHS Safety Assessment Form Tool – Hazard Identification Page 2 of 3
Client Health Record #<br />
Client Surname<br />
Given Name<br />
Community Health Services<br />
<strong>SAFETY</strong> <strong>ASSESSMENT</strong> <strong>FORM</strong> <strong>TOOL</strong> –<br />
<strong>HAZARD</strong> <strong>IDENTIFICATION</strong><br />
Date of Birth<br />
Gender<br />
MFRN<br />
PHIN<br />
Section 2. Biological Hazards<br />
Section 2. a. Animals in the Home/Site<br />
Animals in the home/site ........................................................................................................................................... No Yes<br />
None identified, please proceed to the next section.<br />
If yes, identify the following:<br />
Type of animals: _______________________________________________________________________________________________________________________________________<br />
How many of each type: ______________________________________________________________________________________________________________________________<br />
Does the client follow guidelines regarding animals? ................................................................................................ No Yes<br />
If no, the Safe Visit Plan should be developed<br />
Section 2. b. Stray Needles (Sharps) in the Home/Site<br />
There are a significant number of stray/improperly disposed used needles/sharps/lancets in the home/site<br />
None identified, please proceed to the next section.<br />
Section 2. c. Infestation in the Home/Site<br />
Evidence of an infestation in the home/site<br />
If yes, please indicate the type of infestation: mice rats roaches bed bugs mould<br />
Other Biological Hazards. Please specify: ________________________________________________________________________________________________________<br />
None identified, please proceed to the next section.<br />
Section 3. Chemical Hazards<br />
Section 3. a. Smoking in the Home/Site<br />
Client/Household member(s) smoke in the home/site.<br />
Client/Household member(s) do not follow the WRHA non-smoking policy regarding cigarettes and marijuana.<br />
If box is checked, a Safe Visit Plan needs to be developed.<br />
Other chemical hazards. Please specify: _________________________________________________________________________________________________________<br />
None identified. Please proceed to next section.<br />
Musculoskeletal Injury Prevention/Ergonomics<br />
Ergonomic hazards for Manual Materials Handling (laundry, food prep, housekeeping) and Safe Patient Handling (HCA, wound<br />
care, etc.) can be dealt with via those specific processes. Should either of those services be required, please refer to their specific<br />
assessment processes and address the applicable hazards accordingly.<br />
SAFT<br />
Completed by:<br />
NAME AND DESIGNATION<br />
SAFT Reviewed<br />
and/or Updated by:<br />
NAME AND DESIGNATION<br />
Date:<br />
D D M M M Y Y Y Y<br />
Date:<br />
D D M M M Y Y Y Y<br />
SVP Completed: Yes No<br />
SVP Updated: Yes No<br />
<strong>FORM</strong> # W-00439 10/11 CHS Safety Assessment Form Tool – Hazard Identification Page 3 of 3