Which vaccine(s) would you like to receive today? - Kinney Drugs
Which vaccine(s) would you like to receive today? - Kinney Drugs
Which vaccine(s) would you like to receive today? - Kinney Drugs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
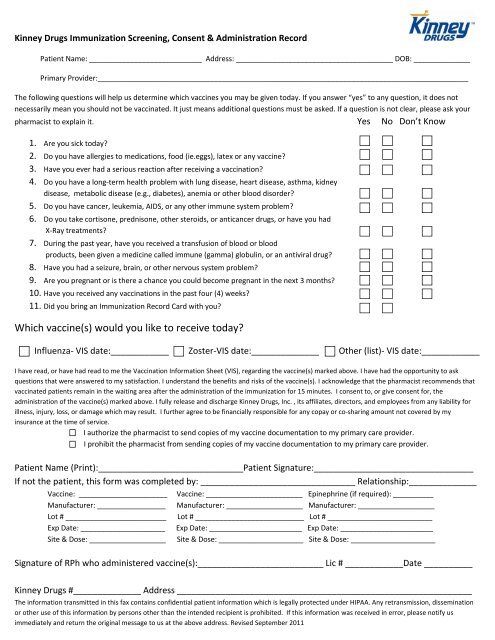
<strong>Kinney</strong> <strong>Drugs</strong> Immunization Screening, Consent & Administration Record<br />
Patient Name: ____________________________ Address: _______________________________________ DOB: ______________<br />
Primary Provider:____________________________________________________________________________________________<br />
The following questions will help us determine which <strong>vaccine</strong>s <strong>you</strong> may be given <strong>to</strong>day. If <strong>you</strong> answer “yes” <strong>to</strong> any question, it does not<br />
necessarily mean <strong>you</strong> should not be vaccinated. It just means additional questions must be asked. If a question is not clear, please ask <strong>you</strong>r<br />
pharmacist <strong>to</strong> explain it. Yes No Don’t Know<br />
1. Are <strong>you</strong> sick <strong>to</strong>day?<br />
2. Do <strong>you</strong> have allergies <strong>to</strong> medications, food (ie.eggs), latex or any <strong>vaccine</strong>?<br />
3. Have <strong>you</strong> ever had a serious reaction after receiving a vaccination?<br />
4. Do <strong>you</strong> have a long‐term health problem with lung disease, heart disease, asthma, kidney<br />
disease, metabolic disease (e.g., diabetes), anemia or other blood disorder?<br />
5. Do <strong>you</strong> have cancer, leukemia, AIDS, or any other immune system problem?<br />
6. Do <strong>you</strong> take cortisone, prednisone, other steroids, or anticancer drugs, or have <strong>you</strong> had<br />
X‐Ray treatments?<br />
7. During the past year, have <strong>you</strong> <strong>receive</strong>d a transfusion of blood or blood<br />
products, been given a medicine called immune (gamma) globulin, or an antiviral drug?<br />
8. Have <strong>you</strong> had a seizure, brain, or other nervous system problem?<br />
9. Are <strong>you</strong> pregnant or is there a chance <strong>you</strong> could become pregnant in the next 3 months?<br />
10. Have <strong>you</strong> <strong>receive</strong>d any vaccinations in the past four (4) weeks?<br />
11. Did <strong>you</strong> bring an Immunization Record Card with <strong>you</strong>?<br />
<strong>Which</strong> <strong>vaccine</strong>(s) <strong>would</strong> <strong>you</strong> <strong>like</strong> <strong>to</strong> <strong>receive</strong> <strong>to</strong>day?<br />
Influenza‐ VIS date:____________ Zoster‐VIS date:______________ Other (list)‐ VIS date:____________<br />
I have read, or have had read <strong>to</strong> me the Vaccination Information Sheet (VIS), regarding the <strong>vaccine</strong>(s) marked above. I have had the opportunity <strong>to</strong> ask<br />
questions that were answered <strong>to</strong> my satisfaction. I understand the benefits and risks of the <strong>vaccine</strong>(s). I acknowledge that the pharmacist recommends that<br />
vaccinated patients remain in the waiting area after the administration of the immunization for 15 minutes. I consent <strong>to</strong>, or give consent for, the<br />
administration of the <strong>vaccine</strong>(s) marked above. I fully release and discharge <strong>Kinney</strong> <strong>Drugs</strong>, Inc. , its affiliates, direc<strong>to</strong>rs, and employees from any liability for<br />
illness, injury, loss, or damage which may result. I further agree <strong>to</strong> be financially responsible for any copay or co‐sharing amount not covered by my<br />
insurance at the time of service.<br />
I authorize the pharmacist <strong>to</strong> send copies of my <strong>vaccine</strong> documentation <strong>to</strong> my primary care provider.<br />
I prohibit the pharmacist from sending copies of my <strong>vaccine</strong> documentation <strong>to</strong> my primary care provider.<br />
Patient Name (Print):______________________________Patient Signature:_________________________________<br />
If not the patient, this form was completed by: ________________________________ Relationship:______________<br />
Vaccine: ______________________<br />
Manufacturer: _________________<br />
Lot # _________________________<br />
Exp Date: _____________________<br />
Site & Dose: ___________________<br />
Vaccine: ________________________ Epinephrine (if required): __________<br />
Manufacturer: ___________________ Manufacturer: ___________________<br />
Lot # ___________________________ Lot # __________________________<br />
Exp Date: _______________________ Exp Date: _______________________<br />
Site & Dose: _____________________ Site & Dose: _____________________<br />
Signature of RPh who administered <strong>vaccine</strong>(s):__________________________ Lic # ____________Date __________<br />
<strong>Kinney</strong> <strong>Drugs</strong> #______________ Address _____________________________________________________________<br />
The information transmitted in this fax contains confidential patient information which is legally protected under HIPAA. Any retransmission, dissemination<br />
or other use of this information by persons other than the intended recipient is prohibited. If this information was <strong>receive</strong>d in error, please notify us<br />
immediately and return the original message <strong>to</strong> us at the above address. Revised September 2011
FAX<br />
Physician Notification of Vaccination Letter<br />
Dear Doc<strong>to</strong>r or Nurse at : _____________________________________<br />
Patient’s Primary Care Provider / Clinic<br />
Address: __________________________________________________<br />
Phone #: __________________________________________________<br />
Fax #: ____________________________________________________________________________________<br />
We have recently provided vaccination services <strong>to</strong> one of <strong>you</strong>r patients. A Vaccine Administration<br />
Record was filled out and given <strong>to</strong> the patient. We want <strong>to</strong> make certain that <strong>you</strong>, <strong>to</strong>o, have this<br />
information so that <strong>you</strong> can update <strong>you</strong>r patient’s medical record. Please contact us if <strong>you</strong> have<br />
any questions about this information.<br />
Patient’s Name: _____________________________ Patient’s Birthdate: __________________<br />
The <strong>vaccine</strong>s that were given on ___________________ are checked below.<br />
Date<br />
Influenza (injectable)<br />
Influenza (intranasal)<br />
Zoster (shingles)<br />
Other ___________________________<br />
Other ___________________________<br />
Other ___________________________<br />
Provider: <strong>Kinney</strong> <strong>Drugs</strong> # ____________<br />
Address: ___________________________________________________<br />
City, State, Zip: ______________________________________________<br />
Contact Person: _____________________________________________<br />
Phone Number: _____________________________________________<br />
Confidential Patient Information<br />
The information transmitted in this FAX is intended only for the person or entity <strong>to</strong> whom it is addressed and contains<br />
Confidential Patient Information and must be handled accordingly. Any retransmission, dissemination or other use of this information<br />
by persons other than the intended recipient is prohibited. If this information is <strong>receive</strong>d in error, please contact the sender and destroy<br />
the FAX immediately.