Adult and Pediatric Perioperative Antimicrobial Prophylaxis Guidelines
Adult and Pediatric Perioperative Antimicrobial Prophylaxis Guidelines
Adult and Pediatric Perioperative Antimicrobial Prophylaxis Guidelines

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
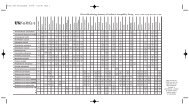
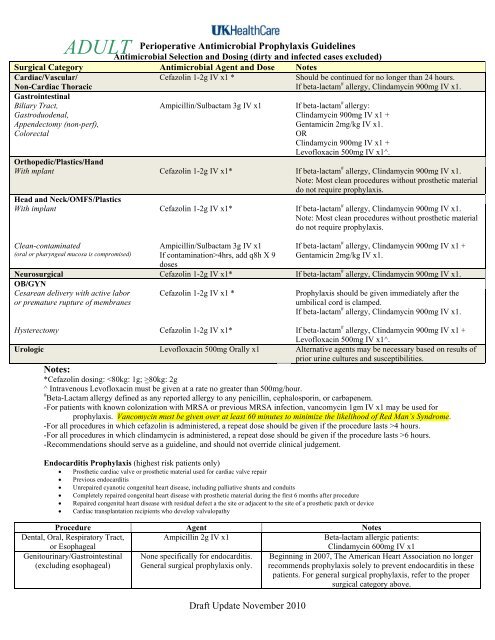
ADULT ive <strong>Antimicrobial</strong> <strong>Prophylaxis</strong> <strong>Guidelines</strong><br />
Antimi icrobial Selection <strong>and</strong> Dosing (dirty <strong>and</strong> infected cases excluded)<br />
Surgical Category<br />
Cardiac/Vascular/<br />
Non-Cardiac Thoracic<br />
Gastrointestinal<br />
Biliary Tract,<br />
Gastroduodenal,<br />
Appendectomy (non-perf),<br />
Colorectal<br />
<strong>Antimicrobial</strong> Agent <strong>and</strong> Dose<br />
Cefazolin 1-2g IV x1 *<br />
Ampicillin/Sulbactam<br />
3g IV x1<br />
Notes<br />
Should be continued for no longer than 24 hours.<br />
If beta-lactam allergy, Clindamycin 900mg IV x1.<br />
If beta-lactam allergy:<br />
Clindamycin 900mg IV<br />
x1 +<br />
Gentamicin 2mg/kg IV<br />
x1.<br />
OR<br />
Clindamycin 900mg IV<br />
x1 +<br />
Levofloxacin 500mg IV<br />
x1^.<br />
Orthopedic/Plastics/H<strong>and</strong><br />
With mplant<br />
Cefazolin 1-2g IV x1*<br />
If beta-lactam allergy, Clindamycin 900mg IV x1.<br />
Note: Most clean procedures without prosthetic material<br />
do not require prophylaxis.<br />
Head <strong>and</strong><br />
Neck/OMFS/Plastics<br />
With implant<br />
Cefazolin 1-2g IV x1*<br />
If beta-lactam allergy, Clindamycin 900mg IV x1.<br />
Note: Most clean procedures without prosthetic material<br />
do not require prophylaxis.<br />
Clean-contaminated<br />
(oral or pharyngeal mucosa is<br />
compromised)<br />
Neurosurgical<br />
OB/GYN<br />
Cesarean delivery with active labor<br />
or premature rupture of<br />
membranes<br />
Ampicillin/Sulbactam<br />
3g IV x1<br />
If contamination>4hrs, add q8h X 9<br />
doses<br />
Cefazolin 1-2g IV x1*<br />
Cefazolin 1-2g IV x1 *<br />
If beta-lactam # allergy, Clindamycin 900mg IV x1 +<br />
Gentamicin 2mg/kg IV<br />
x1.<br />
If beta-lactam # allergy, Clindamycin 900mg IV x1.<br />
<strong>Prophylaxis</strong> should be given immediately after the<br />
umbilical cord is clamped.<br />
If beta-lactam # allergy, Clindamycin 900mg IV x1.<br />
Hysterectomy<br />
Cefazolin 1-2g IV x1*<br />
If beta-lactam allergy, Clindamycin 900mg IV x1 +<br />
Levofloxacin 500mg IV<br />
x1^.<br />
Urologic<br />
Levofloxacin 500mg Orally x1 Alternative agents may<br />
be necessary based on results of<br />
prior urine cultures <strong>and</strong><br />
susceptibilities.<br />
Notes:<br />
*Cefazolin dosing: 80kg: 2g<br />
^ Intravenous Levofloxacin must be given at a rate no greater than 500mg/hour.<br />
# Beta-Lactam allergy defined as any reported allergy to any penicillin, cephalosporin, or carbapenem.<br />
-For patients with known colonization with MRSA or previous MRSA infection, vancomycin 1gm IV<br />
x1 may be used for<br />
prophylaxis. Vancomycin must be given over at least 60 minutes to minimize the likelihood of Red Man’s Syndrome.<br />
-For all procedures in which cefazolin is administered, a repeat dose should be given iff the proceduree lasts >4 hours.<br />
-For all procedures in which clindamycin is administered, a repeat dose should be given if the procedure lasts >6 hours.<br />
-Recommendations should serve as a guideline, <strong>and</strong> should<br />
not override clinical judgement.<br />
Endocarditis <strong>Prophylaxis</strong> (highest risk patients only)<br />
Prosthetic cardiac valve or prosthetic material used for cardiac valve repair<br />
Previous endocarditis<br />
Unrepaired cyanotic congenital heart disease, including palliative shunts <strong>and</strong> conduits<br />
Completely repaired congenital heart disease with prosthetic material during thee first 6 months after procedure<br />
Repaired congenital heartt disease with residual defect a the site or adjacent to the site of a prosthetic patch or device<br />
Cardiac<br />
transplantation recipients who develop valvulopathy<br />
Procedure<br />
Dental, Oral, Respiratory Tract,<br />
or Esophageal<br />
Genitourinary/Gastrointestinal<br />
(excluding esophageal)<br />
Agent<br />
Ampicillin 2g IV x1<br />
None specifically for endocarditis.<br />
General surgical prophylaxis<br />
only.<br />
Notes<br />
Beta-lactam allergic patients:<br />
Clindamycin 600mg IV x1<br />
Beginning in 2007, The American Heart Association no longer<br />
recommends prophylaxis solely<br />
to prevent endocarditis in these<br />
patients. For general surgical prophylaxis, refer to the proper<br />
surgical category above.<br />
Draft Update November 2010
PEDIA ATRIC<br />
<strong>Perioperative</strong> <strong>Antimicrobial</strong> <strong>Prophylaxis</strong>s <strong>Guidelines</strong><br />
<strong>Antimicrobial</strong> Selection <strong>and</strong> Dosing (dirty <strong>and</strong> infected cases excluded)<br />
Surgical<br />
Category<br />
<strong>Antimicrobial</strong> Agent <strong>and</strong>d <strong>Pediatric</strong> Dose<br />
(See opposite side for adult doses)<br />
Notes<br />
Cardiac/Vascular/<br />
Non-Cardiac Thoracicc<br />
Gastrointestinal<br />
Biliary Tract,<br />
Gastroduodenal,<br />
Appendectomy (non-perf),<br />
Colorectal<br />
Cefazolin 30mg/kg IV x1<br />
0-6 months: Ampicillin 50mg/kg IV +<br />
Gentamicin 2. .5mg/kg IV +<br />
Clindamycin 10-15mg/kg IV<br />
>6 months: Ampicillin/Sulbactam 50mg/kgg<br />
For beta-lactam allergic patients:<br />
Clindamycin 10mg/kgg x1<br />
For beta-lactam allergic patients:<br />
Clindamycin 15mg/kgg x1 +<br />
Gentamicin 2.5mg/kgg x1<br />
OR<br />
Metronidazole 10mg/ /kg IV x1<br />
(ampicillin component)<br />
Orthopedic/Plastics/H<strong>and</strong><br />
For beta-lactam allergic patients:<br />
Clindamycin 10mg/kgg x1.<br />
With implant<br />
Cefazolin 30mg/kg IV x1<br />
Most clean procedures without<br />
prosthetic material do<br />
not require<br />
prophylaxis.<br />
Head <strong>and</strong><br />
Neck/OMFS/Plastics<br />
With implant<br />
Cefazolin 30mg/kg IV x1<br />
For beta-lactam allergic patients:<br />
Clindamycin 10mg/kgg x1. Most clean<br />
procedures without prosthetic material<br />
do not require prophylaxis.<br />
Clean-contaminated<br />
(oral or pharyngeal mucosa is compromised)<br />
Cefazolin 30mg/kg IV x1 +<br />
Clindamycin 10-15mg/kg IV<br />
x1<br />
For beta-lactam allergic patients:<br />
Clindamycin 10mg/kgg IV x1 +<br />
Gentamicin 2.5mg/kgg IV x1<br />
Neurosurgical<br />
Cefazolin 30mg/kg IV x1<br />
For beta-lactam allergic patients:<br />
Clindamycin 10mg/kgg x1<br />
Urologic<br />
(for patients with knownn bacteriuria only)<br />
0-2 yrs: Gentamicin 2.5mg/kg IV x1<br />
>2 yrs: Sulfamethoxazole/Trimethoprim<br />
5mg/kg (trimethoprim component) IV<br />
Alternative agents may be necessaryy<br />
based on results of prior urine cultures.<br />
infusion over 60 minutes x1<br />
Notes:<br />
-For patients with known colonization with MRSA or previous MRSA infection, vancomycin 15mg/kg IVPB x1 may be used<br />
for prophylaxis. Vancomycin must<br />
be given over<br />
60 minutes to minimize the likelihood of Red Man’s Syndrome.<br />
-Sulfamethoxazole/Trimethoprim <strong>and</strong> Doxycycline should<br />
be administered as an infusion over 60 minutes.<br />
-For all procedures in which cefazolin is administered, a repeat dose should be given iff the proceduree lasts >4 hours.<br />
-For all procedures in which clindamycin is administered, a repeat dose should be given if the procedure lasts >6 hours.<br />
-Recommendations should serve as a guideline, <strong>and</strong> should<br />
not override clinical judgement.<br />
-Endocarditis<br />
<strong>Prophylaxis</strong>:<br />
Procedure<br />
Agent<br />
Notes<br />
Dental,<br />
Oral, Respiratory Tract, or Esophageal<br />
Ampicillin<br />
50mg/kg IV x1 or<br />
Beta-lactam allergic patients:<br />
Cefazolin 30mg/kg IV<br />
x1<br />
Clindamycin 10mg/kg IV x1<br />
Genitourinary/Gastrointestinal (excluding<br />
Ampicillin 50mg/kg IV x1, then<br />
Beta-lactam allergic patients:<br />
esophageal)<br />
25mg/kg IV 6 hrs later +<br />
Vancomycinn 20mg/kg IV infusion x1 +<br />
Gentamicin 2.5mg/kg<br />
gentamicin (dose at left)<br />
(max 120mg) x1 on induction<br />
OR<br />
>6 months: Ampicillin/Sul<br />
lbactam<br />
50mg/kg (ampicillin component)<br />
References:<br />
-Medical Letter. <strong>Antimicrobial</strong> <strong>Prophylaxis</strong> in Surgery. Med Lett Drugs Ther. October 29, 2001;43(1116-1117):92-7.<br />
-IDSA (Infectious Diseases Society of America). Quality St<strong>and</strong>ards<br />
Subcommittee of<br />
the Clinical Affairs Committee. Dellinger EP, Grosss PA, Barrett TL, et al. Quality st<strong>and</strong>ards<br />
for antimicrobial prophylaxis in<br />
surgical procedures. Released in 1994 (reviewed in 1998). Clin Infectt Dis 1994 Mar;18(3):422-7.<br />
-ASHP (American Society of Health System Pharmacists). ASHP Commission on Therapeutics: ASHPP Therapeutic <strong>Guidelines</strong> on <strong>Antimicrobial</strong> <strong>Prophylaxis</strong> in Surgery. Am J<br />
Health Syst Pharm 1999;56:1839-88.<br />
-American Heart Association. Wilson W, Taubertt KA, Gewitz M,, et al. Prevention of Bacterial Endocarditis. Circulationn 2007;106.<br />
Draft Update November 2010