Advanced Hemodynamics - Orlando Health
Advanced Hemodynamics - Orlando Health
Advanced Hemodynamics - Orlando Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Advanced</strong> Hemodynamic Monitoring<br />
intrapulmonary pressures will increase on inspiration and decrease on expiration. Therefore, the<br />
point of end expiration will look different depending on how your patient ventilates. In the<br />
spontaneously breathing patient, end expiration will be the highest point on the waveform before it<br />
dips. Conversely, for the mechanically ventilated patient the end expiration will be the lowest point<br />
on the waveform before it rises.<br />
Keep in mind that the transducer must be properly leveled and zeroed prior to assessing any values.<br />
If too high, it will give a falsely low reading, and if too low, it will give a falsely high reading.<br />
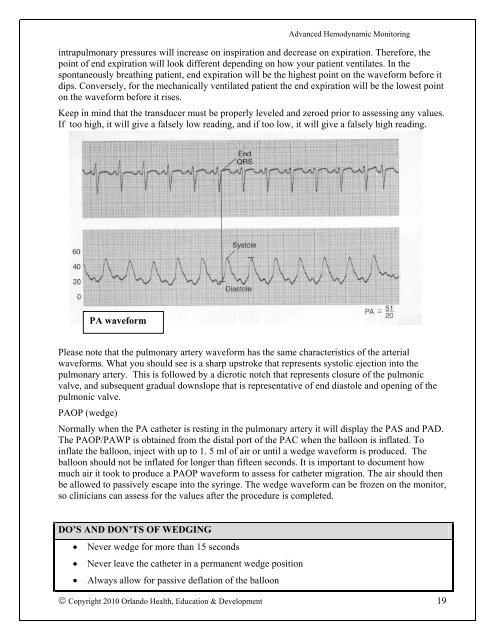
PA waveform<br />
Please note that the pulmonary artery waveform has the same characteristics of the arterial<br />
waveforms. What you should see is a sharp upstroke that represents systolic ejection into the<br />
pulmonary artery. This is followed by a dicrotic notch that represents closure of the pulmonic<br />
valve, and subsequent gradual downslope that is representative of end diastole and opening of the<br />
pulmonic valve.<br />
PAOP (wedge)<br />
Normally when the PA catheter is resting in the pulmonary artery it will display the PAS and PAD.<br />
The PAOP/PAWP is obtained from the distal port of the PAC when the balloon is inflated. To<br />
inflate the balloon, inject with up to 1. 5 ml of air or until a wedge waveform is produced. The<br />
balloon should not be inflated for longer than fifteen seconds. It is important to document how<br />
much air it took to produce a PAOP waveform to assess for catheter migration. The air should then<br />
be allowed to passively escape into the syringe. The wedge waveform can be frozen on the monitor,<br />
so clinicians can assess for the values after the procedure is completed.<br />
DO’S AND DON’TS OF WEDGING<br />
Never wedge for more than 15 seconds<br />
Never leave the catheter in a permanent wedge position<br />
Always allow for passive deflation of the balloon<br />
Copyright 2010 <strong>Orlando</strong> <strong>Health</strong>, Education & Development 19